Gall bladder and biliary tract disorders Sampath Poreddy

Gall bladder and biliary tract disorders Sampath Poreddy, MD Gastroenterology/Advanced endoscopy University of Cincinnati

Gall bladder and sphincter functions • Fasting state: • Sphincter of Oddi offers a high pressure zone of resistance to bile flow • Post prandial state: • Cholecystokinin released from duodenum in response to ingested fats and aminoacids • CCK: • Powerful contraction of the gallbladder • Relaxes sphincter of Oddi

Question All of the following conditions need a cholecystectomy except for? A. Porcelain gall bladder B. Asymptomatic gall stones more than 3 cm in size C. Congenitally deformed gall bladder with stones D. Anomalous union of the pancreaticobiliary ductal system E. Asymptomatic holelithiasis in pregnant women

Question All of the following conditions need a cholecystectomy except for? A. B. C. D. E. Porcelain gall bladder Asymptomatic gall stones more than 3 cm in size Congenitally deformed gall bladder with stones Anomalous union of the pancreaticobiliary ductal system Asymptomatic cholelithiasis in pregnant women

Gallstones • Gall stones are formed due to abnormal bile composition • Two major types: • Cholesterol stones • Pigment stones • Cholesterol stones: • > 90% of all gallstones • Contain >50% cholesterol monohydrate • Pigment stones: • • Calcium bilirubinate Classified into “black” and “brown” Black: chronic indirect hyperbilirubinemia eg: hemolytic anemia Brown: secondary to chronic biliary infection
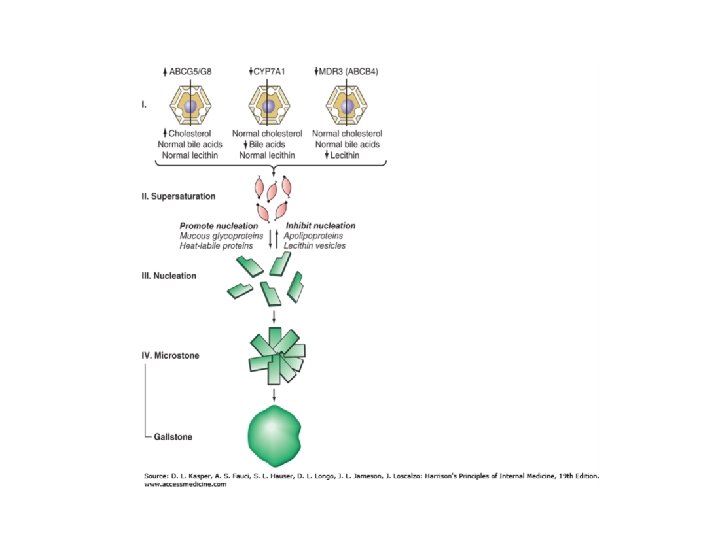

Cholesterol stones Risk factors: • North American Indians • Obesity, metabolic syndrome • Weight loss • Estrogens • Pregnancy • Increasing age • Gall bladder hypomotility: fasting, TPN, Octreotide • Clofibrate therapy • PBC • Spinal cord injury • Genetic defects: CYP 7 A 1, MDR 3 gene

Pigment stones Risk factors: • Asia, rural setting, Clonorchis sinensis and roundworm • Chronic hemolysis • Liver cirrhosis • Pernicious anemia • Cystic fibrosis • Chronic biliary tract infection • Increasing age • Ileal disease, ileal resection or bypass

GB sludge/microlithiasis • Thick, mucous material • Microscopic exam: • lecithin cholesterol liquid crystals, cholesterol monohydrate crystals, calcium bilirubinate, and mucin gel • precursor form of gallstone disease • US: • Crescent like layer in gallbladder • GB hypomotility: • surgery, burns, TPN, pregnancy, and BCPs • Biliary sludge implies supersaturation of bile with either cholesterol or calcium bilirubinate

Symptoms of Gallstone Disease • Asymptomatic – most common • Symptoms obstruction of cystic or CBD • Biliary colic begins suddenly and persist with severe intensity for 30 min to 5 h, subsiding gradually or rapidly • Pain is steady rather than intermittent • Nausea and vomiting • Biliary pain more than 5 hr should raise the suspicion of acute cholecystitis

Symptoms of Gallstone Disease • Fever or chills + biliary pain: indicates a complication • cholecystitis, pancreatitis, or cholangitis • Biliary colic is precipitated by: fatty meal, large meal or by normal meal • Tenderness at RUQ

Natural history 60 80% of asymptomatic gallstones remain asymptomatic over next 25 years 2 4% develops symptoms in 5 years then 1 2% per year Most patients develop biliary symptoms before developing complications requiring cholecystectomy

Diagnosis • LFTs are normal • Elevated bilirubin and/or alkaline phosphatase suggests a common duct stone • US has 95% of sensitivity and specificity for stones >2 mm

Treatment Surgical therapy: laparoscopic cholecystectomy Recommendation for cholecystectomy • • • symptoms that interfere daily routine h/o complications from gallstones calcified or porcelain gallbladder Patients with very large gallstones (>3 cm in diameter) gallstones in a congenitally anomalous gallbladder

Medical therapy Gall stone dissolution: • Functioning gallbladder • Radiolucent stones <10 mm • Complete dissolution can be achieved in ∼ 50% of patients within 6 24 months • UDCA can be used for recurrent choledocholithiasis after cholecystectomy

Acute Cholecystitis • Prolonged obstruction of the cystic duct by a stone • Inflammation • Increased intraluminal pressure: ischemia • Release of lysolecithin (action of phospholipase on lecithin in bile)and prostaglandins • Bacteria: Escherichia coli, Klebsiella spp. , Streptococcus spp. , and Clostridium spp.

Acute Cholecystitis Diagnosis: • RUQ pain, RUQ tenderness, fever, and leukocytosis highly suggestive • Ultrasound: sonographic murphy’s sign, calculi, signs of GB inflammation • HIDA scan: confirmatory if no visualization of the GB • CT scan: if suspicion for complications • emphysematous cholecystitis • Perforation of GB

Treatment • Medical management: NPO, IV fluids, NG prn and Abx • piperacillin tazobactam • ceftriaxone plus metronidazole • levofloxacin plus metronidazole • Early cholecystectomy

Acalculous cholecystitis • Cholecystitis with out stones • Critically ill • Ultrasound or CT • large, tense, static gallbladder • without stones and poor emptying • Complication rate is higher than calculous cholecystitis • Management: • early diagnosis • IR (cholecystostomy tube)/surgical intervention

Emphysematous Cholecystitis • Secondary infection of GB wall with gas forming organisms • Diabetics or older men with out cholelithiasis • GB Perforation risk is high • Emergency Abx with anaerobic coverage and early cholecystectomy

Porcelain Gallbladder • Intramural calcification of the gallbladder wall • Risk of GB cancer is high up to 20% of cases • Prophylactic cholecystectomy
 and into")
Cholecystoenteric Fistula • Stone erodes through the gallbladder wall (usually the neck) and into a hollow viscus • Entry points: duodenum, hepatic flexure of the colon, stomach and the jejunum • If the gallstone exceeds 25 m in diameter • small intestinal obstruction - gallstone ileus • ileocecal area is the most common site • Radiograph: pneumobilia, a dilated small bowel, and a large gallstone in the right lower quadrant • Bouveret's syndrome: gastric outlet obstruction from duodenal stone impaction

Choledocholithiasis • Stones in the bile ducts • biliary colic, jaundice, pruritus, cholangitis or acute pancreatitis • 15% with cholelithiasis have bile duct stones • Patients with CBD stones cholelithiasis in 95%

Choledocholithiasis Diagnosis: • US: • Bile duct stones in 50% • CBD dilation more than 6 mm in 75% • EUS: • sensitivity and specificity of about 98% as compared with ERCP • MRCP: • Sensitivity and specificity of about 93 to 94% compared with ERCP

Choledocholithiasis Treatment: • ERCP • Biliary sphincterotomy + stone extraction • All stones in CBD needs rx • PTC (Percutaneous transhepatic cholangiography): • when intrahepatic bile ducts are dilated • when ERCP is unavailable or has been technically unsuccessful

Special circumstances • HIV patients: • AIDS associated cholangiopathy & papillary stenosis • infection of the duodenal and biliary epithelium • cryptosporidia, CMV, microsporidia, or Isospora

Special circumstances High risk for cholecystectomy: • ERCP with sphincterotomy and stone removal without cholecystectomy • Cholecystectomy may be required in 10% of patients (due to recurrent symptoms)

Mirizzi's Syndrome • Compression of CBD/CHD due to stone in the neck of the gallbladder or cystic duct • Jaundice and RUQ pain • ERCP extrinsic compression on CHD +/ fistula • Preop diagnosis is important to minimize the risk of BD injury • Treatment open cholecystectomy

Question A 67 year old woman presented to ED with h/o intermittent right upper quadrant abdominal pain for last 3 months. Her pain got worsened over the last 3 days and became constant. Her vital exam showed mild tachycardia and temp of 102 f. Abdominal exam showed right upper quadrant tenderness. Lab work revealed total bili of 4 mg/dl, Alk phos: 300, AST: 110, ALT: 250, WBC of 17000 and normal lipase. An ultrasound exam showed findings suggestive of cholelithiasis and dilated biliary tree. All of the following are true in her management except for? A. B. C. D. E. Blood cultures Broad spectrum antibiotics Urgent ERCP MRCP Get surgery consult for cholecystectomy

Question • A 67 year old woman presented to ED with h/o intermittent right upper quadrant abdominal pain for last 3 months. Her pain got worsened over the last 3 days and became constant. Her vital exam showed mild tachycardia and temp of 102 f. Abdominal exam showed right upper quadrant tenderness. Lab work revealed total bili of 4 mg/dl, Alk phos: 300, AST: 110, ALT: 250, WBC of 17000 and normal lipase. An ultrasound exam showed findings suggestive of cholelithiasis and dilated biliary tree. All of the following are true in her management except for? A. Blood cultures B. Broad spectrum antibiotics C. Urgent ERCP D. MRCP E. Get surgery consult for cholecystectomy

Cholangitis • Charcot's triad: RUQ pain, jaundice, and fever • Altered mental status + hypotension + Charcot's triad – Reynold’s pentad (severe suppurative cholangitis) • Intra hepatic abscess • E. coli , Klebsiella , Pseudomonas , Proteus , and enterococci, Bacteroides fragilis and Clostridium perfringens

Diagnosis • Clinical exam • Ultrasound: 50% stones, 75% duct dilation • CT scan: exclude chlecystitis, pancreatitis, abscess • ERCP: definitive test for the diagnosis of bile duct stones and cholangitis

Treatment • Blood cultures and empiric broad spectrum antibiotics • ERCP with biliary sphincterotomy, stone removal and +/ stent placement • PTC if ERCP is unsuccessful • Cholecystectomy

Cholangiocarcinoma Risk Factors: • Definite: Caroli's disease, Choledochal cyst, Hepatolithiasis, Opisthorchis viverrini, PSC, Thorotrast • Probable: Biliary enteric drainage procedures, Cirrhosis, Clonorchis sinensis infection, Heavy alcohol consumption, Hepatitis C, Toxins (dioxins, polyvinyl chloride)

Gall bladder cancer Risk factors: • Anomalous union of the pancreaticobiliary ductal system • Carcinogens: methyl cholanthrene, O aminoazo toulene, nitrosamines Cholangiocarcinoma • Cholelithiasis (stone size > 1 m)

Gall bladder cancer Risk Factors: • • Salmonella typhi or Paratyphi carrier status First degree relative with gallbladder cancer IBD Intrahepatic biliary dysplasia Lynch syndrome Porcelain gallbladder PSC Segmental adenomyomatosis in patients ≥ 60 yrs

• Questions?
- Slides: 37