Functions of blood 1 Place of exchange of

Functions of blood 1. Place of exchange of substances between interstitial fluid and external environment 2. Transport 3. Buffer function 4. To keep body temperature relatively constant 5. Hemostasis 6. Defense function

Blood properties and its components
 Specific gravity blood: 1. 050~ 1. 060.")
Physical and chemical properties of blood (1) Specific gravity blood: 1. 050~ 1. 060. (RBC number) plasma: 1. 025~ 1. 030. (Content of plasma proteins) RBC: 1. 090 ~ 1. 092. (hemoglobin) (2) Viscosity of plasma is 1. 2 -1. 3 times that of water, viscosity of whole blood is 2. 4 times of plasma.
 Plasma osmolality Colloid osmotic pressure: maintain intra-and extracapillary water equilibrium Crystal osmotic pressure:")
(3) Plasma osmolality Colloid osmotic pressure: maintain intra-and extracapillary water equilibrium Crystal osmotic pressure: maintain intra-and extracellular water equilibrium 4. RBC fragility 5. Plasma p. H 7. 35 -7. 45

 - White")
Components of blood • Plasma • Cells - Red blood cells (erythrocytes) - White blood cells (leukocytes) - Platelets (thrombocytes) Blood volume: 70 -80 ml/Kg
 Alpha and")
Components of Plasma 90% Water 8% Solutes: • Proteins Albumin (60 %) Alpha and Beta Globulins Gamma Globulins Fibrinogens • Gases • Electrolytes

• Organic Nutrients Carbohydrates Amino Acids Lipids Vitamins • Hormones • Metabolic waste CO 2 Urea
")
Formed elements of blood (Cells)

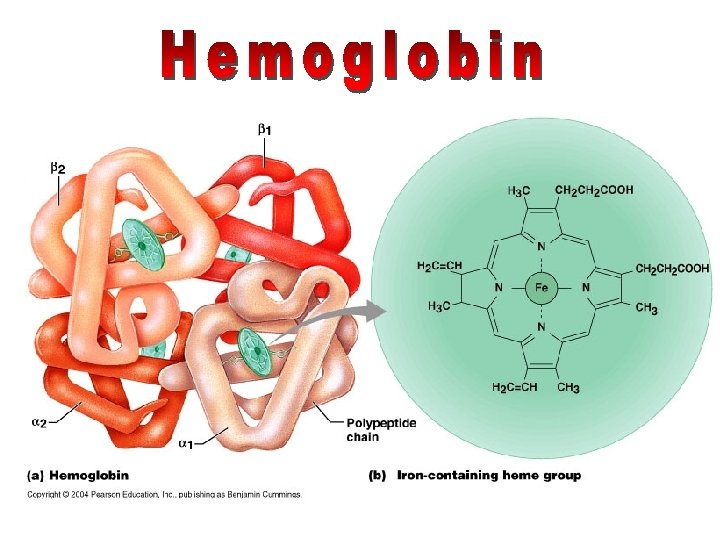
Erythrocytes • RBCs are flattened biconcave discs – Shape provides increased surface area for diffusion – Lack nuclei & mitochondria – Each RBC contains hemoglobin 13 -9

Erythrocyte 7. 5 m in diameter · Men- 5. 5 million cells/mm 3 · Women- 4. 5 million cells/mm 3 · Life span 100 -120 days and then destroyed in spleen.
: blood cell formation – Occurs in red bone marrow of")
Hematopoiesis • Hematopoiesis (hemopoiesis): blood cell formation – Occurs in red bone marrow of axial skeleton, girdles and proximal epiphyses of humers and femur
 – Give rise to all formed elements –")
Hematopoiesis • Hemocytoblasts (hematopoietic stem cells) – Give rise to all formed elements – Hormones and growth factors push the cell toward a specific pathway of blood cell development • New blood cells enter blood sinusoids

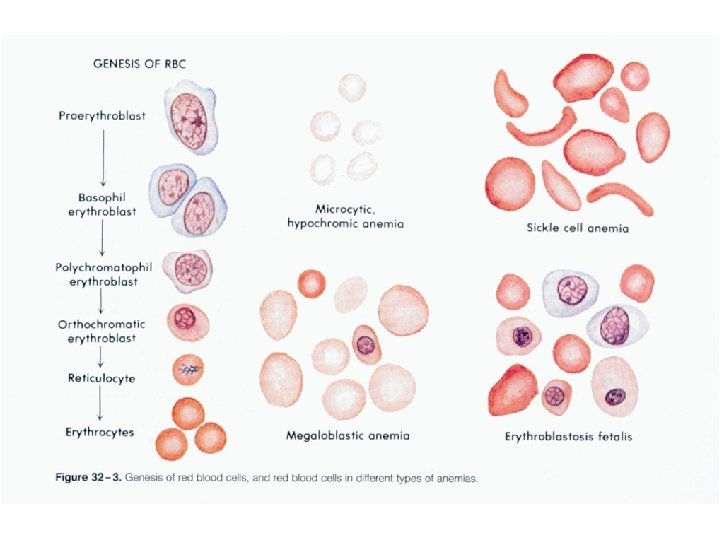
Erythropoiesis • Erythropoiesis: red blood cell production – A hemocytoblast is transformed into a proerythroblast – Proerythroblasts develop into early erythroblasts

Erythropoiesis – Phases in development 1. Ribosome synthesis 2. Hemoglobin accumulation 3. Ejection of the nucleus and formation of reticulocytes – Reticulocytes then become mature erythrocytes

Stem cell Hemocytoblast Committed cell Developmental pathway Proerythroblast Early Late erythroblast Phase 1 Ribosome synthesis Phase 2 Hemoglobin accumulation Phase 3 Ejection of nucleus Normoblast Reticulo- Erythrocyte

Regulation of Erythropoiesis • Too few RBCs leads to tissue hypoxia • Too many RBCs increases blood viscosity • Balance between RBC production and destruction depends on – Hormonal controls – Adequate supplies of iron, amino acids, and B vitamins
 – Direct stimulus for erythropoiesis – Released")
Hormonal Control of Erythropoiesis • Erythropoietin (EPO) – Direct stimulus for erythropoiesis – Released by the kidneys in response to hypoxia

Causes of hypoxia – Hemorrhage or increased RBC destruction reduces RBC numbers – Insufficient hemoglobin (e. g. , iron deficiency) – Reduced availability of O 2 (e. g. , high altitudes)

• Effects of EPO – More rapid maturation of committed bone marrow cells – Increased circulating reticulocyte count in 1 – 2 days • Testosterone also enhances EPO production, resulting in higher RBC counts in males

Formation & Destruction of RBCs

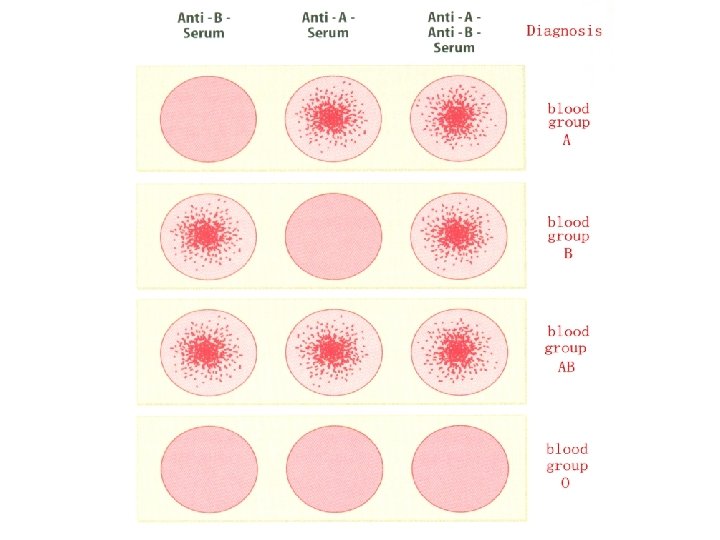
RBC Antigens & Blood Typing • Antigens present on RBC surface specify blood type • Major antigen group is ABO system – Type A blood has only A antigens – Type B has only B antigens – Type AB has both A & B antigens – Type O has neither A or B antigens 13 -15

Transfusion Reactions • People with Type A blood make antibodies to Type B RBCs, but not to Type A • Type B blood has antibodies to Type A RBCs but not to Type B • Type AB blood doesn’t have antibodies to A or B • Type O has antibodies to both Type A & B • If different blood types are mixed, antibodies will cause mixture to agglutinate

Transfusion Reactions • If blood types don't match, recipient’s antibodies agglutinate donor’s RBCs • Type O is “universal donor” because lacks A & B antigens – Recipient’s antibodies won’t agglutinate donor’s Type O RBCs • Type AB is “universal recipient” because doesn’t make anti-A or anti-B antibodies – Won’t agglutinate donor’s RBCs

Rh Factor RH+ indicates protein RH- indicates no protein

Type AB- universal recipients Type O- universal donor Rh factor: Rh+ 85% dominant in pop Rh- 15% recessive Blood Type Clumping Antibody A antigen A anti-A serum antibody anti-b B antigen B anti-B serum antibody anti-a AB antigen A & B anti A & B serum O neither A or B no clumping w/ either anti A or B anti-a, anti-b -

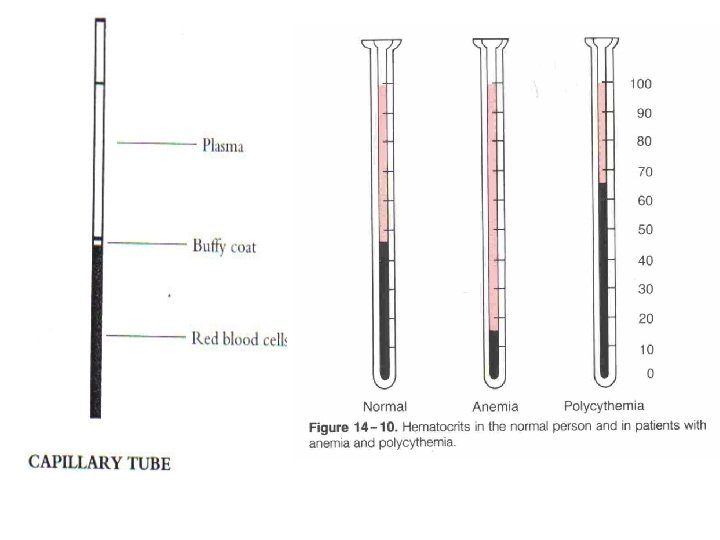
Anemia- when blood has low O 2 carrying capacity; insufficient RBC or iron deficiency. Factors that can cause anemia as B 12 deficiency Polycythemia- excess of erythrocytes, viscosity of blood; 8 -11 million cells/mm 3 Usually caused by cancer, tissue hypoxia, dehydration (naturally occurs at high elevations)

Anemia • Inability of blood to supply tissues with adequate oxygen for proper metabolic function. • Diagnosis made by patient history, physical examination, signs and symptoms, and hematological laboratory findings. • Usually associated with decreased levels of hemoglobin or hematocrit (packed red cell volume) - Abnormal hemoglobin may give appearance of anemia (methemoglobin). • Usually associated with decreased RBCs. 30
 or severe (Hb <7 g/dl).")
Anemia • Classified as moderate (Hb 7 -10 g/dl) or severe (Hb <7 g/dl). • Physical signs include difficulty breathing (dyspnea), vertigo, muscle weakness and headaches. Rapidly developing anemia may be associated with hypotension and tachycardia. • Two general forms of anemia: Absolute anemia (decrease in red cell mass) and relative Anemia (increased plasma volume gives appearance of anemia). 31
 Infection Toxicity")
Causes of Anemia Nutritional deficiencies Hemolytic disorders Blood loss Bone marrow (hypoproliferative) Infection Toxicity Hemopoetic stem cell damage (maturation disorder) • Heredity or acquired defect • • 32

Classification of Anemias • Have a variety of ways - depending on criteria used: – Functional – Morphological – Clinical – Quantitative 33
 – Defective hemoglobin synthesis •")
Functional Classification of Anemias • Decreased RBC production (hypoproliferative) – Defective hemoglobin synthesis • Fe deficiency • B 12 deficiency • Folate deficiency – Impaired bone marrow or stem cell function, as in leukemia • Increased RBC destruction, as in sickle cell anemia or glucose 6 phosphatase deficiency or hemolytic anemia 34

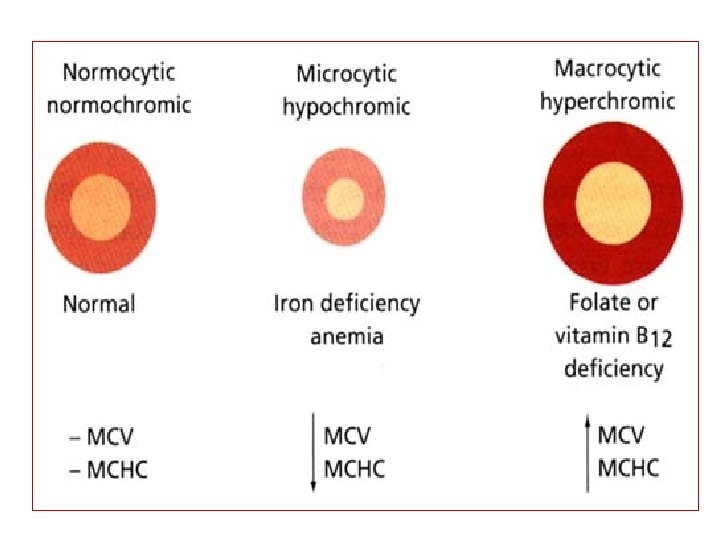
Morphological Classification of Anemias • Morphological based on sizes and color of RBCs – Normochromic – Hypochromic 35 Normocytic Microcytic Macrocytic Microcytic

Clinical Classification of Anemias • According to their associated causes: – Blood loss – Iron deficiency – Hemolysis – Infection – Nutritional deficiency – Metastatic bone marrow replacement 36

Quantitative Classification of Anemias • Quantitatively by: – Hematocrit – Hemoglobin – Blood cell indices – Reticulocyte count 38
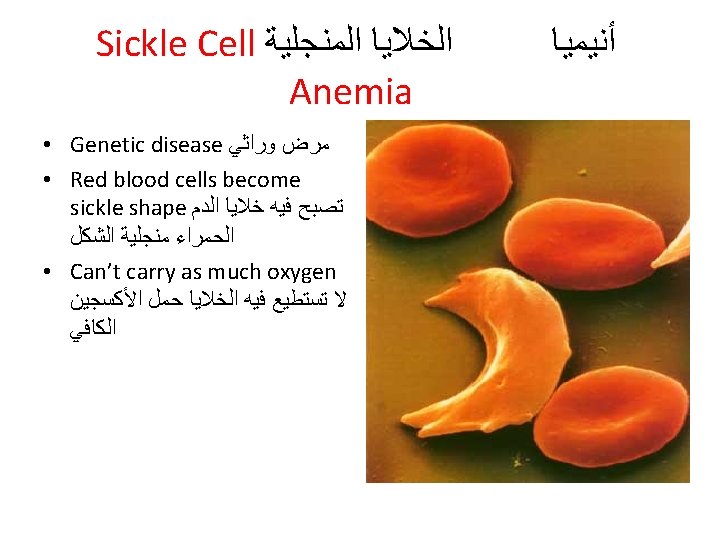

Sickle-cell anemia • Sickle cell disease: genetic disease – Defect in hemoglobin (The beta subunit has the amino acid valine at position 6 instead of the glutamic acid that is normally present ) 43

Blood Tests
 • Hematocrit (Hct)")
• Component of the CBC: • Red Blood Cells (RBCs) • Hematocrit (Hct) • Hemoglobin (Hgb) • Mean Corpuscular Volume (MCV) • Mean Corpuscular Hemoglobin Concentration (MCHC) • White Blood Cells (WBCs) • Platelets

Hemoglobin : M: 14 to 16 gm/d. L F: 12 to 14 gm/d. L Hematocrit : (packed cell volume) It is ratio of the volume of red cell to the volume of whole blood. M: 40 to 50 % F: 36 to 44 %
 Tests (In the Diagnosis of Anemia) Hgb is the main component of")
Hemoglobin (Hgb) Tests (In the Diagnosis of Anemia) Hgb is the main component of RBCs and carries oxygen to tissues. Three methods to measure hemoglobin: • • – Cyan-met-hemoglobin (recommended method) – Oxyhemoglobin – Iron Content 48
 • • • 1. Blood is diluted in a")
Cyan-met-hemoglobin (method to measure Hgb) • • • 1. Blood is diluted in a solution of potassium ferricyanide and potassium cyanide, which oxidizes the hemoglobin to form methemoglobin. 2. Then methemoglobin forms cyanmethemoglobin in the presence of the potassium cyanide. 3. Absorbance of solution is read in spectrophotometer at 540 nm.
 PCV")
Hematocrit (packed cell volume) PCV
 – Mean Corpuscular")
RBC Indices • RBC indices include: – Mean Corpuscular Volume (MCV) – Mean Corpuscular Hemoglobin (MCH) – Mean Corpuscular Hemoglobin Concentration (MCHC) 52

– MCV = mean corpuscular volume HCT/RBC count= 87 f. L • small = microcytic • normal = normocytic • large = macrocytic - MCH (mean corpuscular hemoglobin) HB/RBC count = 27 -32 pg – MCHC= mean corpuscular hemoglobin concentration HB/HCT= 26 -34% • decreased = hypochromic • normal = normochromic

MCV • Mean cell volume • MCV is average size of RBC • MCV = Hct x 10 RBC (millions) • If 80 -100 f. L, normal range, RBCs considered normocytic • If < 80 f. L are microcytic • If > 100 f. L are macrocytic • Not reliable when have marked anisocytosis 54

MCH • MCH is average weight of hemoglobin per RBC. • MCH = Hgb x 10 RBC (millions) = 27 -32 pg 55

MCHC • MCHC is average hemoglobin concentration per RBC • MCHC = Hgb x 100 Hct (%) = 26 -34% • If MCHC is normal, cell described as normochromic • If MCHC is less than normal, cell described as hypochromic • There are no hyperchromic RBCs 56

• This important value is needed in the evaluation of any anemia. • Normal range 1 -2% • count goes up with Hemolytic anemia • goes down with Nutritional deficiencies • Diseases of the bone marrow itself

Erythrocyte Sedimentation Rate • It is the distance sedimented by R. B. Cs. In a vertical blood column at the end of one and two hours. • It is measured by the height of clear plasma formed at the top of blood which is kept fluid by adding an anticoagulant
")
Blood being tested Type AB (contains agglutinogens A and B; agglutinates with both sera) Anti-A Serum Anti-B RBCs Type A (contains agglutinogen A; agglutinates with anti-A) Type B (contains agglutinogen B; agglutinates with anti-B) Type O (contains no agglutinogens; does not agglutinate with either serum) Figure 17. 16
- Slides: 60