FREELIVING AMOEBAE CAUSING HUMAN INFECTIONS are normal inhabitants

FREE-LIVING AMOEBAE CAUSING HUMAN INFECTIONS _ are normal inhabitants of soil and water where they feed on bacteria. _ A few members have the ability to become facultative parasites when an opportunity to enter a vertebrate exists. _They are able to infect humans
 are small, freely living, widely distributed in soil and water.")
Free-living amoebae (FLA) are small, freely living, widely distributed in soil and water. �FLA of the genera Naegleria, Acanthamoeba, Balamuthia and Sappinia can cause disease in humans and other animals.

�Normally, they live as �Phagotrophs- in aquatic habitats where they feed on bacteria. �Opportunists- in humans, they may produce serious infection of the central nervous system (CNS) and the eye.

They are termed as ‘amphizoic’ has ability to live in two worlds, as free-living organisms and as endoparasites.

�Naegleria fowleri �Acanthamoeba spp. �Balamuthia mandrillaris �Sappinia pedata

FLAs are aerobic, eukaryotic protists that comprise several genera. �Worldwide Geographic distribution. �Found in fresh water, mud and moist soil and normally feeding on bacteria.
 invasion by Naegleria fowleri, Acanthamoeba spp.")
Hundreds of patients with Central nervous system (CNS) invasion by Naegleria fowleri, Acanthamoeba spp. , and Balamuthia mandrillaris and thousands of. Acanthamoeba keratitis has been reported in worldwide. ��

�In India, 2 cases of Primary Amoebic Meningoencephalitis reported by Pan and Ghose in 1971. �In India, >20 cases were reported so far from Mangalore, Kolkata and Rajasthan.

NAEGLERIA FOWLERI Naegleria fowleri is a free living braineating amoeba. _ Typically found in warm fresh water (thermo tolerant amoeba). _ worldwide distribution. _ It exists in trophozoite and cyst forms and in a transient flagellate stage. _ _
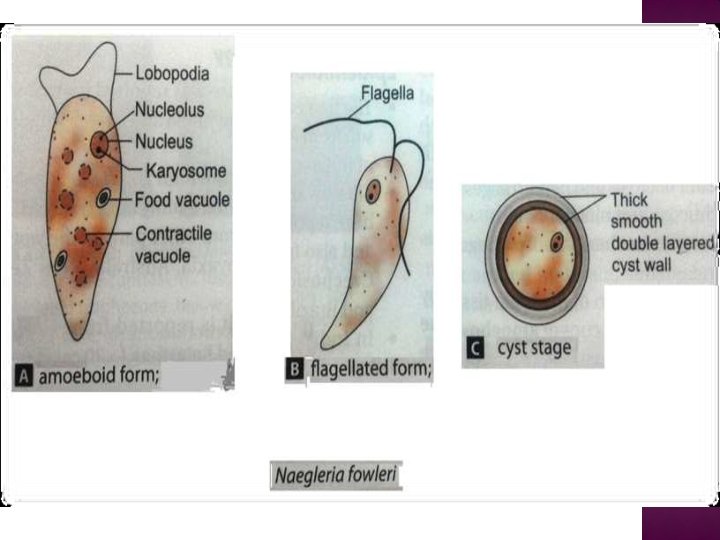

Naegleria -has three stages �Trophozoite- an amoeboid form, shows brisk progressive movements at 21 o. C by means of rounded pseudopodia (lobopodia). � 9 - 15μm in diameter,

�Slud-shaped with one broad and one pointed extremity and known as LIMAX amoebae. �Cyst- dormant form, thick smooth double layered cyst wall. �Flagellate form.

Pear shaped cell with 2 flagella • Found in surface layer of the water • Rapidly motile • Not found in CSF or brain

They are uninucleated and possess double cyst wall. • Found on the surface of vegetation and mud. • Not found in CSF or in brain.

Naegleria fowleri has three stages, cysts , trophozoites , and flagellated forms , in its life cycle. • In the soil amoeba gets transformed from trophozoite form to flagellate form in the water.

• Trophozoites can turn into temporary nonfeeding flagellated forms which usually revert back to the trophozoite stage. • The trophozoites multiply by binary fission

NAEGLERIA FOWLERI When a victim swims or sinks into freshwater. All victims have had a history of swimming in freshwater lakes or ponds or swimming pools a few days before the onset of symptoms
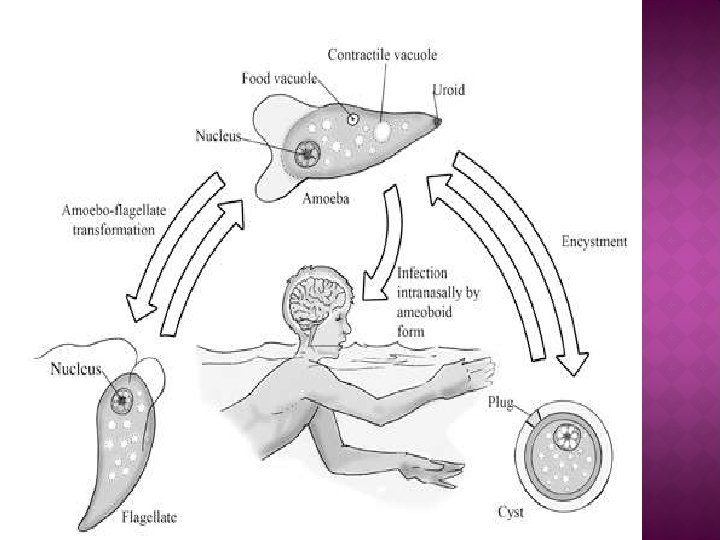

NAEGLERIA FOWLERI Trophozoites encyst under unfavorable condition and excyst under favorable condition. • Trophozoites infect humans or animals by penetrating the nasal mucosa and migrating to the brain via the olfactory nerves causing primary amoebic meningoencephalitis (PAM).
 and tissue, while")
• N. fowleri trophozoites are found in cerebrospinal fluid (CSF) and tissue, while flagellated forms are occasionally found in CSF.

�Reproduction is by simple binary fission of the trophozoite. �Nuclear division is promitotic. During this process, the nuclear membrane remains intact.
. _ The period")
Naegleria fowleri is the causative agent of primary amebic meningoencephalitis (PAM). _ The period incubation is short, the symptoms are acute, and death is almost certain and rapid. _Naegleria fowleri invades the C. N. S. via penetration of the olfactory mucosa and nasal tissues (nose).

Since Naegleria fowleri trophozoites and cysts are susceptible to chlorine, swimming pools should be adequately chlorinated.

NAEGLERIA FOWLERI

Naegleria fowleri causes an acute, fulminating hemorrhagic meningoencephalitis principally in healthy children and young adults with a history of recent exposure to warm fresh water.

• The striking feature of PAM is the rapid onset of symptoms following exposure. • The disease progresses rapidly, and, without prompt diagnosis and intervention, death usually occurs within a week or less

NAEGLERIA FOWLERI-DIAGNOSIS • Most symptoms involving fever , headache, stiff neck and confusion. • Diagnosis with X-ray , IHAT in CSF. • Occasionally, a C. T scan may be ordered to rule out cerebral hematoma. culture of CSF and PCR.

NAEGLERIA FOWLERI-DIAGNOSIS A wet-mount of the CSF - for the presence of actively moving trophozoites. • Smears of CSF should be stained with Giemsa or Wright stains to identify the trophozoite.

Few patients have survived PAM. • Large dose of antifungal agent amphotericin-B (1 mg/Kg/day I. V. for several days) or ketoconazole (800 mg daily orally for one month). • Azithromycin, a macrolide antimicrobial, has been shown to be effective against Naegleria both in vitro and in vivo

ACANTHAMOEBA Several species of Acanthamoeba, including A. culbertsoni, A. polyphaga, A. castellanii, A. astronyxis, A. hatchetti, A. rhysodes, A. divionensis, A. lugdunensis, and A. lenticulata are implicated in human disease. • The important species is A. culbertsoni

ACANTHAMOEBA CULBERTSONI Free-living trophozoites and cysts occur in both the soil and freshwater. Trophozoites occur only as amoeboid forms

ACANTHAMOEBA CULBERTSONI Free-living amoeba Lives in water have been found in soil; sea water; sewage; swimming pools; contact lens equipment; medicinal pools; dental treatment units and air conditioning systems
Trophozoite-A trophozoite is 2050μm in size -Rough exterior")
There are two morphological forms (a)Trophozoite-A trophozoite is 2050μm in size -Rough exterior with several spine like projections(acanthopoda). (b)Cyst-Spherical and 15μm in diameter. • Both forms can be the source of infection
 by using")
ACANTHAMOEBA CULBERTSONI Contact lens wearers can get keratitis (infection of the cornea) by using tap water for lens disinfection or by swimming when wearing lenses

Acanthamoe ba

ACANTHAMOEBA _ Cysts are common and are very resistant to chlorine. _ opportunists can cause infections in human. _ Infections with these amoebae are more common in immunocompromised patients. .

Acanthamoeba has only two stages, cysts and trophozoites , in its life cycle. No flagellated stage exists as part of the life cycle. • The trophozoites replicate by mitosis.

When Acanthamoeba spp. enters the eye it can cause severe keratitis in otherwise healthy individuals, particularly contact lens users.

• When it enters the respiratory system or through the skin, it can invade the central nervous system by hematogenous dissemination causing granulomatous amebic encephalitis (GAE) or disseminated disease , or skin lesions in individuals with compromised immune systems
. 2 - Disseminated granulomatous amebic disease (eg,")
ACANTHAMOEBA 1 - granulomatous amebic encephalitis (GAE). 2 - Disseminated granulomatous amebic disease (eg, skin, sinus, and pulmonary infections). 3 - Amebic keratitis: a sightthreatening disease. Most cases occur in people who wear contact lenses
 and disseminated infection primarily affect people with compromised immune")
Granulomatous Amebic Encephalitis (GAE) and disseminated infection primarily affect people with compromised immune systems. • Commonly seen in immunocompromised patients, including those with neoplasia, systemic lupus erythematosus, human immunodeficiency virus and tuberculosis

Incubation period unknown but estimated at weeks to months. The route of infection is aerosol or direct inoculation with hematogenous spread to the CNS.

Acanthamoeba results in lesions of the skin, eye, brain, etc.


THE SYMPTOMS OF GAE INCLUDING : ALTER MENTAL STATUS, HEADACHE , FEVER, NECK STIFFNESS, SEIZURES, FOCAL NEUROLOGICAL SIGNS AND COMA LEADING TO DEATH

keratitis : corneal inflammation and corneal perforation often followed by blindness.
motile trophozoites • Culture-Agar plates")
CSF wet mount (usually lymphocyte predominance and low glucose)motile trophozoites • Culture-Agar plates seeded with E. coli • Immunofluorescence or polymerase chain reaction (PCR). • Corneal scrape or biopsy

GAE is treated with pentamidine, usually in combination with one or more of the following: ketoconazole, hydroxystilbamidine, paromomycin, 5 -fluorocytosine polymyxin, sulfadiazine, trimethoprim sulfamethoxazole and azithromycin

• CAK-Therapy should include the cationic antiseptic agents, of which chlorhexidine or polyhexamethylene biguanide (PHMB) is the most effective. • Ocular lesions –enucleation of ulcer and corneal transplant

It was first identified in 1986 in a specimen from the brain of a baboon that died in the San Diego Wild Animal Park. • Since then, approximately 200 cases of Balamuthia disease have been reported worldwide. • Little is known at this time about how a person becomes infected.

Trophozoite- Two forms of pseudopodia either broad lobose or finger like. - 12 -60μm in length - sluggishly motile • Cyst – It is spherical -6 -30μm in size

Balamuthia amoebas are thought to enter the body when soil containing Balamuthia comes in contact with skin wounds and cuts, or when dust containing Balamuthia is breathed in or gets in the mouth.

• Once inside the body, the amoebas can then travel to the brain and cause Granulomatous Amebic Encephalitis (GAE).

• GAE is a severe disease of the brain that is fatal in over 95% of cases. • It can take weeks to months to develop the first symptoms of Balamuthia GAE after initial exposure to the amoebas.

Some early symptoms might include a combination of the following: • Severe headache • Stiff neck, or neck pain with neck movement • Sensitivity to light • Nausea and vomiting

Unusual fatigue • Fever • Difficulty walking or talking • Sudden one-sided weakness • Behavioral changes • Seizures • Unusual skin lesions that persist over months •

Microscopical examination of CSF –Trophozoites • Tissue culture • The indirect Immunofluorescence assay (IFA) is a test used to detect antibodies attached to Balamuthia amoebas in body tissues. • PCR

A combination of flucytosine, pentamidine, fluconazole, sulfadiazine and either azithromycin or clarithromycin. • Surgical excision of the lesion may reduced the parasite load.
 reported the first and only case of Sappinia amoebic")
Gelman et al. (2001) reported the first and only case of Sappinia amoebic encephalitis in a 38 - year-old previously healthy, immunocompetent male.

• It had been isolated from soil, fresh water, forest litter, mammalian faeces and the rectum of lizard. • It has been described from Europe, North America, Egypt, the Middle East, the West Indies, and Japan

Both trophozoite and cyst stages are binucleate. • The trophozoite measures 40– 80 mm, is ovoid or oblong, and appears to be flattened with occasional wrinkles on the surface. • The mature cyst is round and measures 15– 30 mm

Description - meningoencephalitis associated with cerebral tumor-like lesion, described in one case only. • Incubation period, mode of spread and risk factors - all remain unknown. It is likely to be reach the CNS either through the nasal mucosa or the bloodstream.

Epidemiology - only one case described in the literature. • Presentation - sinus infection was followed by headache, vomiting and photophobia.

CT brain scan in the single reported case revealed a tumorlike mass. • PCR is likely to be a very important tool in diagnosing this particular infection.

In the reported case, the cerebral lesion was surgically removed and azithromycin, pentamidine, itraconazole and flucytosine were also administered
- Slides: 65