Frailty What are we talking about 14 th

Frailty What are we talking about? 14 th October 2015 Dr Jane Shoote Consultant Geriatrician

Setting the scene • Worldwide population is ageing • Impacts healthcare planning and provision • The most problematic expression of population ageing is the clinical condition of FRAILTY • Around 10% of over 65 s have frailty • Over 25 of over 85 s have frailty (in some studies >50%)

Formal definitions “a state of increased vulnerability to stressors due to age-related declines in physiologic reserves across neuromuscular, metabolic, and immune systems” American Geriatric Society 2004

Formal Consensus “a medical syndrome with multiple causes and contributors that is characterised by diminished strength, endurance, and reduced physiological function, that increases an individual’s vulnerability for developing increased dependency and/or death” J Am Med Dir Assoc 2013

The frailty condition • • Related to the ageing process Independently associated with adverse outcomes Common Progressive Episodic deteriorations Preventable components Impact quality of life Expensive Harrison J, Clegg A, Conroy S, Young J. Managing frailty as along-term condition. Ageing 2015; 44: 732 -5.

A frail individual Impacting quality of life

Pathophysiology of frailty • Accelerated decrease in physiological reserve • Failing homeostatic mechanisms Clegg A, Young J, Iliffe S, Rikkert M, Rockwood K. Frailty in elderly people. Lancet. 2013; 381: 752 - 762

Vulnerability of frail elderly people to a sudden change in health status after a minor illness. Clegg A, et al. Frailty in elderly people. Lancet. 2013; 381: 752 – 762.

Cycle of functional decline Sarcopaenia Less muscle mass Sensation of increased effort Lower muscle mass Fewer physical activities

Frailty Age Frailty lies outside the comfort zone of Guideline Based Medicine

Frailty • • State of increased vulnerability Not an inevitable part of ageing Is a chronic condition May be made better or worse • Identification is important and should form part of any health/social care interaction Read codes for CTV 3: mild frailty = Xabd. Y, moderate frailty = Xabdb, Severe frailty = Xabdd
 ◦ Structured, multidisciplinary assessment 2.")
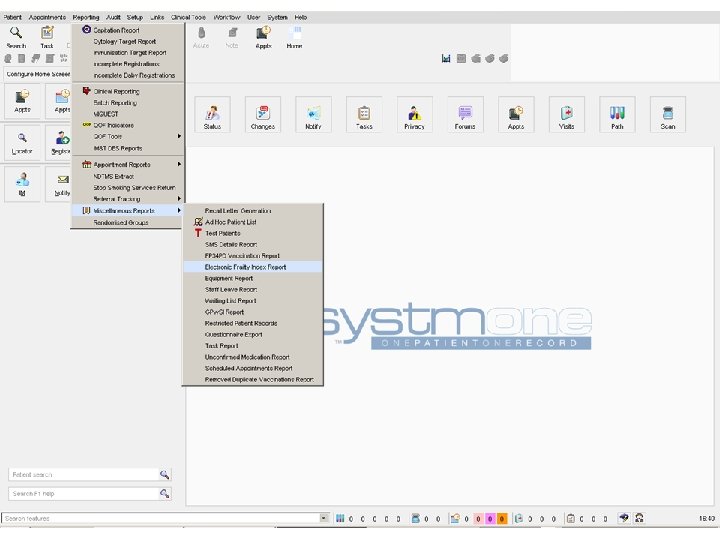
Identifying frailty in practice 1. Comprehensive geriatric assessment (CGA) ◦ Structured, multidisciplinary assessment 2. Simple assessment ◦ ◦ ◦ Gait speed Timed-up-and-go test (TUGT) PRISMA-7 Questionnaire 3. Routine data ◦ Electronic frailty index (e. FI)
")
Fit for Frailty Recommended Frailty Assessment Tools • Gait speed • Timed-up-and-go test (TUGT) • PRISMA-7 questionnaire • Sensitive but not specific • Good to exclude those not frail • Need further clarification on those positive

Gait speed Van Kan G, et al. Gait speed at usual pace as a predictor of adverse outcomes in community-dwelling older people. JNHA 2009; 13: 881 -9. Requires a stop watch and 4 metre distance Median life expectancy 0. 8 m/s > 5 seconds to walk 4 metres Good, valid, simple single tool to predict disability, long term care, falls, mortality • Studies suggest target further examination of gait speeds slower than 0. 6 m/s ? ? • Especially informative if no self report of function • • For identifying frailty: Gait speed <0. 8 m/s = Sensitivity 0. 99, specificity 0. 64

Timed up and go test Podsiadlo, D. et al. The timed, Up & Go: a test of basic functional mobility for frail elderly persons. Journal of American Geriatric Society 1991; 39: 142 -8. • • • TUGT > 10 seconds Positive predictive value = 0. 17 Negative predictive value = 0. 99 Very good for excluding frailty Similar to gait speed and PRISMA-7 would need further clarification of results For identifying frailty: TUGT>10 s = Sensitivity 0. 93, specificity 0. 62

PRISMA – 7 Raiche M, et al. PRISMA-7: A case finding tool to identify older adults with moderate to severe disabilities. Archives of Gerontology and Geriatrics 2008; 47: 9 -18. • • ≥ 3 or above at risk Sensitivity 78. 3% Specificity 74. 7%S Used to identify those who may benefit more comprehensive assessment For identifying frailty: PRISMA-7 = Sensitivity 0. 83, specificity 0. 83

Cumulative deficiency model aka the frailty index ‘The more things that are wrong with you, the more likely you are to be frail’ • Canadian study of health and ageing • Simple calculation of the presence of absence of a variable • Based on 92 baseline variables • Cumulative effect of individual deficits • 92 reduced to 36 without loss of predictability Rockwood K, Song X, Macknight C et al. A global clinical measure of fitness and frailty in elderly people. CMAJ 2005; 173: 489 -95.
 HSJ Supplement 22 November 2012 • Validated using 500,")
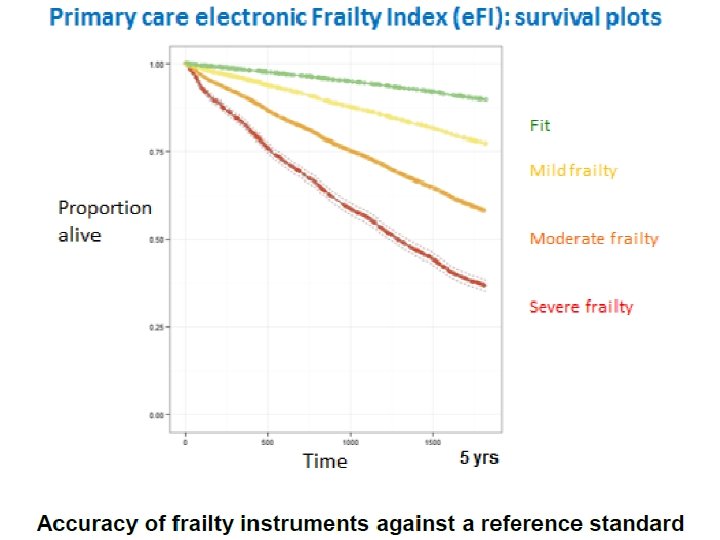
Electronic Frailty Index (e. FI) HSJ Supplement 22 November 2012 • Validated using 500, 000 patients • >2000 Read codes • Calculated as cumulative deficit model E. g. 18 deficits 18/36 = 0. 5 • Scoring: 0 - 0. 12 = Fit 0. 13 – 0. 24 = Mild Frailty 0. 25 – 0. 36 = Moderate Frailty >0. 36 = Severe Frailty • Runs through Systm. One • Relates to the risk of adverse outcomes

List of 36 deficits contained in the e. FI Activity limitation Anaemia & haematinic deficiency Arthritis Atrial fibrillation Cerebrovascular disease Chronic kidney disease Diabetes Dizziness Dyspnoea Falls Foot problems Fragility fracture Hearing impairment Heart failure Heart valve disease Housebound Hypertension Hypotension/syncope Ischaemic heart disease Memory & cognitive problems Mobility and transfer problems Osteoporosis Parkinsonism & tremor Peptic ulcer Peripheral vascular disease Polypharmacy Requirement for care Respiratory disease Skin ulcer Sleep disturbance Social vulnerability Thyroid disease Urinary incontinence Urinary system disease Visual impairment Weight loss & anorexia > 2000 Read codes
 CTV 3 X 76 Ao | Frailty Xabd.")
Read Codes for Frailty (Oct 2014) CTV 3 X 76 Ao | Frailty Xabd. Y | Mild frailty Xabdb | Moderate frailty Xabdd | Severe Frailty Read V 2 2 jd. . | Frailty 2 Jd 0. | Mild frailty 2 Jd 1. | Moderate frailty 2 Jd 2. | Severe frailty
 Young J. 2014")
Preliminary Predictive Validity of Primary Care Electronic Frailty Index (e. FI) Young J. 2014 Frailty is the future talk.

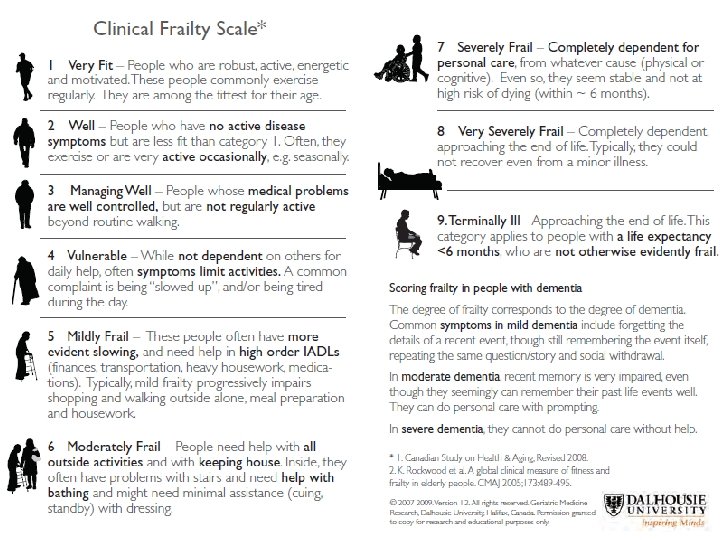
Clinical Frailty Scale Rockwood K, et al. A global clinical measure of fitness and frailty in elderly people. CMAJ 2005; 173: 489 -95. • • • Predictive validity similar to Frailty Index Good correlation with other scales Unclear inter-rater reliability Best used with CGA and geriatrician Timely assessment Ongoing studies

Shared Care Plan On transfer of care from FAB

Deficit accumulation and mortality link Shi et al. Analysis of frailty and survival. BMC Geriatr. 2011; 11: 17.

Frailty Syndromes • • • Non-specific presentations Multiple co-morbidities Communication barriers Disability and complexity Recognition and interpretation • 30 – 60% new dependency in ADLs following admission

Associations with frailty • • Adverse outcomes Worsening disability Falls Admission to hospital Increasing length of stay Risk of admission to long term care Death

Guideline based medicine or care and support planning?

Cumulative deficit impact Mrs A a 78 year old lady with COPD and Type II diabetes, previous MI, depression and osteoarthritis……………. • 11 drugs • 10 possible further drugs recommended • 9 lifestyle modifications advised • 8– 10 routine primary care appointments • 8– 30 psychosocial interventions • Smoking cessation appointments • Pulmonary rehabilitation Hughes et al. Guidelines for people not diseases. Ageing 2013; 42: 62 -9.


Once identified BGS Spring 2015 Prof J Young, Dr E Burns Categorise numerically �Mildly frail – Supported Self Management �eg Age UK a practical guide to healthy ageing �Moderately frail – Care and Support Planning �eg CGA and care plan �Severely frail – anticipatory care planning �eg Case management, ACP and end of life care

Supported self management plan for Healthy Living in Later Life Preventable components for ‘Frailty’ • Affect (Mood problems) • Alcohol excess • Cognitive impairment • Falls • Functional impairment • Hearing problems • Nutritional compromise • Physical inactivity • Polypharmacy • Smoking • Social isolation and loneliness • Vision problems Stuck et al. Soc Sci Med. 1999 (Systematic review of 78 studies) Additional topics: • Look after your feet • Make your home safe • Vaccinations • Keep warm • Get ready for winter • Continence ………others……? ?

NHS England in association with Age UK Produced to help people improve their health and general fitness, particularly those aged 70 or over with ‘mild frailty’. To reorder this guide please order for free online via www. orderline. dh. gov. uk or call 0300123 1002 quoting reference HA 2. Publication date 01/10/15.

Infolink http: //infolink. suffolk. gov. uk/kb 5/suffolk/infolink/home. page

“Right care, at the right time, in the right place” NHS England. Commissioning for carers principle 3

Admission avoidance • Improved access – The ‘Hot Phone’ ◦ � 07930181236 • Regular risk profiling / case finding • Named accountable GP / Care co-ordinator • Holistic care plan • Internal reviews / MDTs of unplanned admissions

Care and support planning • Clinicians and patient with LTC • Collaborative approach to identify ◦ ◦ What is important to that individual Goals Support needs Action plans • Progress is monitored • Continuous process not a one-off event

FAB at a glance ETT GP Routes in ED EAU phone The future: Hot phone Email/Phone Seen within 48 hours Centre of excellence and resource Education and outreach Staff development (GP, ENP etc) Extended management via virtual ward Incorporation of falls and other clinics Full 7 day working Inreach to IHT wards Frailty Assessment Base Comprehensive Geriatric Assessment Dr, Nurse, Therapy, Dietician, Pharmacist Routes out Shared Care Plan Frailty Score Problem list Action plan Admitted Front loaded assessment and management plans FAB team ward follow-up Home CHT CAT Voluntary sector DIST ACS Geriatrician follow-up ICB Interface geriatrician case management

Access • Hot Phone – advice/same day assessment 07930 181236 • Email – 2 working day review ihn-tr. FAB@nhs. net • SHARE Systm. One record

Frailty and end of life • Advanced frailty means EOL is close and should trigger a proactive care approach. • People in their last year of life are admitted an average of 3. 5 times 4 T’s - Reflective practitioner questions • Think Frailty • Timid – am I being timid? • Timeliness – is the right time? • Time – do I need to make time? Uncertainty causes anxiety

New care model for older people & frailty Young J. 2014 A primary care-based model for frailty. Kingsfund presentation.

Frailty is here • Is important to prepare for and aim to postpone • Important to recognise as a state of vulnerability to poor recovery from simple stressor events • Failure to detect frailty potentially exposes patients to interventions from which they might not benefit and may be harmed • Recognising advancing frailty should trigger a proactive care approach to EOL care planning

Thank You jane. shoote@ipswichhospital. nhs. uk Secretary: 01473 704137 Hot phone: 07930 181236

References: 1. 2. 3. 4. 5. NHS England. Toolkit for general practice in supporting older people with frailty. 2014. http: //www. bgs. org. uk/index. php/fit-for-frailty http: //www. york. ac. uk/inst/crd/effectivenessmatters. htm Report by the comptroller and auditor general. End of life care. HC 1043 Session 2007 -2008 | 26 November 2008. Morley et al. Frailty consensus: a call to action. J Am Med Dir Assoc 2013; 14: 392 -7.
- Slides: 46