Fractures Definition A break in the continuity of

Fractures

Definition • A break in the continuity of the bone caused by trauma, twisting as a result of muscle spasm or indirect loss of leverage, or bone decalcification and disease that result in osteopenia

Fractures of long bones

Management • Assess neurovascular status of the extremity • Splint or secure fracture segments • X-ray

Open Fractures

Management of Open Fractures • Open fractures require prompt antibiotic administration • studies show increased infection rate when antibiotics are delayed for more than 3 hours from time of injury • update tetanus prophylaxis as indicated • Control bleeding • Assessment soft-tissue damage • Neurovascular exam • if concern for vascular insult, ankle brachial index (ABI) should be obtained • normal ratio is >0. 9 • vascular surgery consult and angiogram is warranted if ABI <0. 9

Management cont’d • Dressing • remove gross debris from wound, do not remove any bone fragments • place sterile saline-soaked dressing on wound • little evidence to support aggressive irrigation or irrigation with antiseptic solution in the ED, as this can push debris further into wound • Stabilize • splint, brace, or traction for temporary stabilization • decreases pain, minimizes soft tissue trauma, and prevents disruption of clots • Surgery within 6 -24 hours

Pelvic Fractures

Pelvic Fractures • Occur in 20% of multi-trauma cases and most commonly in 15 to 30 year old and in the over 60’s, with 75% of all injuries occurring in men • Mortality in all of pelvic fractures is approximately 16% with hemorrhage being the major reversible factor in 42% of patients • Bleeding in pelvic fractures is from 3 sources; arterial, venous and/or from cancellous bones • The majority of bleeding is venous; however 70% of unstable patients with a pelvic fracture have arterial bleeding. • Disruption of the pelvic ring requires a high energy decelerative force of approximately 50 km/hr. • These forces cause other organ injuries in 90% of patients with an unstable pelvic fracture have other associated injuries and 50% have sources of hemorrhage other than the pelvic fracture

Signs of a significant pelvic fracture • bruising &/or swelling over bony prominences, pubis, perineum, and/or scrotum • leg length discrepancy or rotation deformity of a lower limb • wounds over the pelvis or bleeding from rectum vagina or urethra • neurological abnormality

Complications of unstable pelvic fractures • Unstable pelvic fractures sustained during high-energy incidents, such as car accidents, may result in significant complications, including severe bleeding • Complications may include injury to the bladder or vaginal trauma

Jaw Fractures

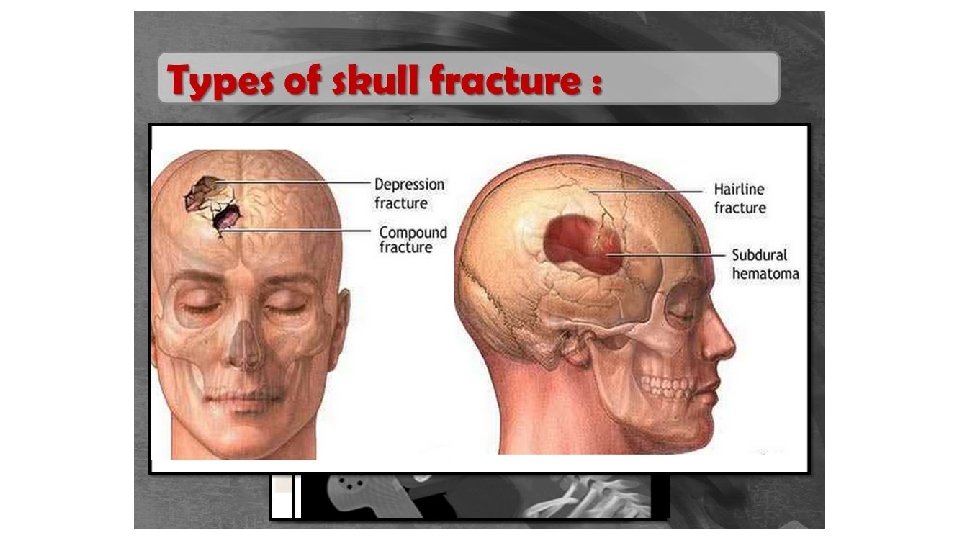
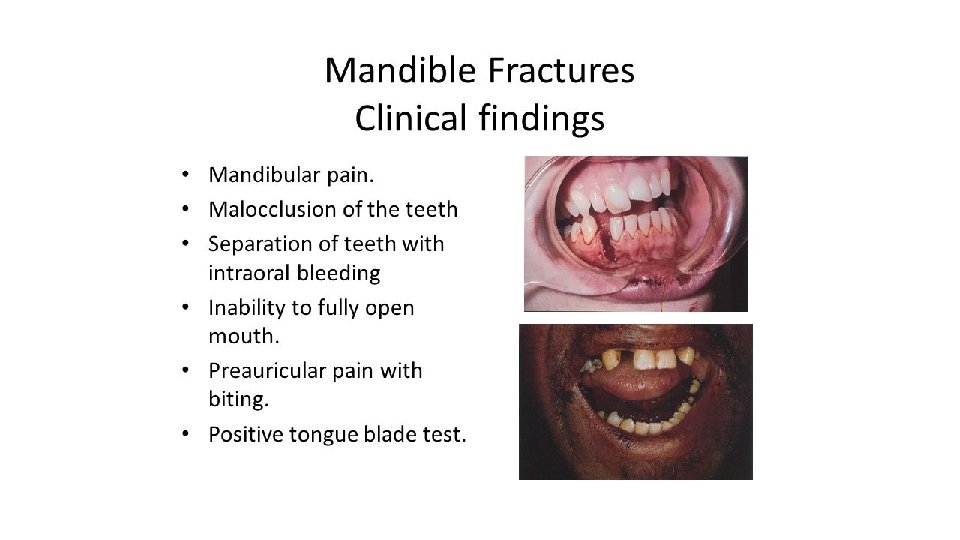
Mandible fractures • Depending on the force of the trauma and the ability of the bone to absorb the shock of the trauma, the resulting fracture may vary between a single hairline fracture and multiple fractures along the mandible. • The location and type of the fracture depends on the magnitude of the force, bone density, structurally weak parts of the bone, the state of the soft tissue surrounding the face and the direction in which the mastication muscles pull the fractured bone fragments

Associated injuries • C-spine injuries in patients presenting with facial fractures ranges from ∼ 2 to 10% • 32% of mandibular fractures are associated with abrasions or lacerations, 24% with neurologic injury, 20% with additional orthopedic injuries, and 12% with pulmonary, abdominal, or cardiac injury • The overall incidence of these accompanying injuries will differ based on the initial mechanism of injury

Primary survey: mandible fracture • Frequently assess airway • Isolated mandible fracture from a blunt mechanism usually does not require intubation, but frequent suctioning is mandatory • Early intubation before swelling occurs makes airway control much easier, rather than waiting until a problem arises from obstruction • This is usually a clinical decision based on projected course • Do not focus on obvious deformity, thereby forgetting to perform a complete primary survey • Rapidly diagnose other life threats and undertake appropriate resuscitation

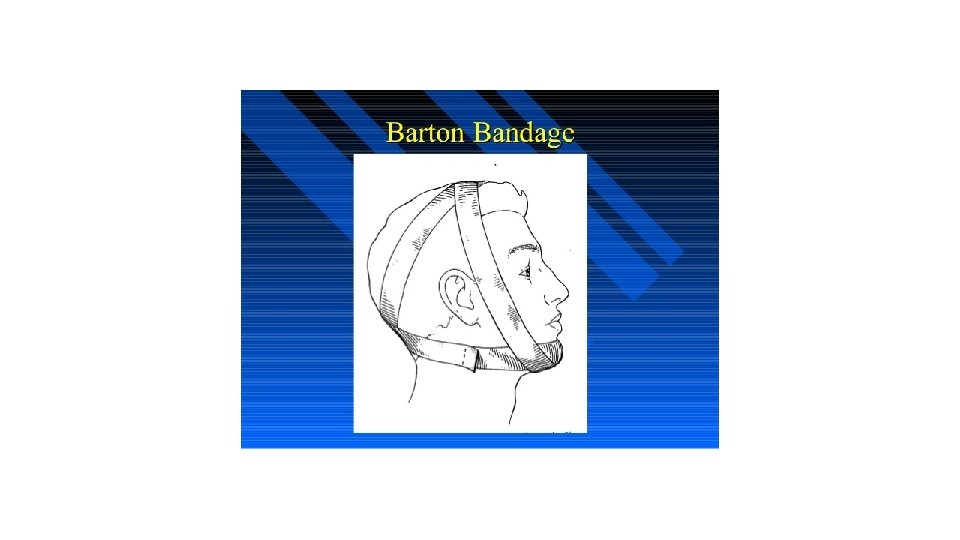
Secondary survey: mandibular fracture • Diagnosis of mandibular fracture is part of the secondary survey of ED care, though it should be kept in mind when evaluating the airway in the primary survey. • A Barton bandage can be placed if the patient has no airway compromise • Open fractures require antibiotics • Penicillin or one of the cephalosporins are current DOC. Penicillin-allergic patients can be given clindamycin.

Complications of Fractures

Fat Embolism • Fat globule is released from marrow into the bloodstream • Can occur within the first 48 -72 hours • Long bone fractures are at greatest risk • Symptoms similar to PE • A petechial rash may present over the upper chest and neck

Other complications of fractures • Avascular necrosis • Compartment syndrome • Infection and osteomyelitis • Pulmonary embolism

Concepts to remember • Bone fragments may be sharp and slice into other tissues • Patients can loose a significant amount of blood with a pelvic fracture
- Slides: 24