Fractures and dislocations of the shoulder girdle and





















 Open fractures n Holstein-Lewis distal 1/3 fractures n")







- Slides: 31
Fractures and dislocations of the shoulder girdle and elbow and fractures of the humerus H. Sithebe
Anterior shoulder dislocation
Two Views. n AP n Lateral
REDUCTION
POST REDUCTION CONTROL X-RAY n SLING 2 -3 WEEKS n AVOID EXTERNAL ROTATION AND ABDUCTION n
COMPLICATIONS AXILLARY NERVE INJURY n VASCULAR INJURY n FRACTURE DISLOCATION n RECURRENT DISLOCATION n BRACHIAL PLEXUS INJURY n
Posterior shoulder dislocation AP Lateral
REDUCTION ARM PULLED AND EXTERNALLY ROTATED n HUMERAL HEAD IS PUSHED FOREWARD n ARMSLING 3 WEEKS n AVOID ADDUCTION, FOREWARD FLEXION AND INTERNAL ROTATION n
COMPLICATIONS AXILLARY NERVE INJURY n VASCULAR INJURY n FRACTURE DISLOCATION n RECURRENT DISLOCATION n BRACHIAL PLEXUS INJURY n
AC joint injuries - Mechanism Direct – fall on point of shoulder with arm aducted n Indirect – upward force on outstretched arm is transmitted up the arm (rare) n Indirect – downward force pull with heavy weight (rare) n
AC DISLOCATION
Fractures of the Clavicle.
Fractures of the clavicle
Fractures of the clavicle n Treatment- conservative. – Sling or collar and cuff. q. Surgery. – Open fractures. – Neurovascular injuries. – 21 st Century.
Complications of clavicle #’s Neurovascular n Non-union 1. 9% n Mal-union > 20 mm shortening leads to pain n Post-traumatic arthritis n
SCAPULA FRACTURES
SCAPULAR FRACTURES n n n n ASSOCIATED INJURIES 35 -98% 10 -15% MORTALITY SEVERELY INJURED PATIENT C-Spine injury! ARTERIAL INJURY BRACHIAL PLEXUS INJURY PNEUMOTHORAX FRACTURED RIBS
Humeral Shaft Fractures Non-Operative Treatment n n n Modified U slab Hanging cast Functional bracing (Sarmiento)
Hanging Arm Cast n n n Mid-shaft fractures with shortening Oblique or spiral pattern Should extend 2 cm proximal to fracture NOT transverse fractures 96% union
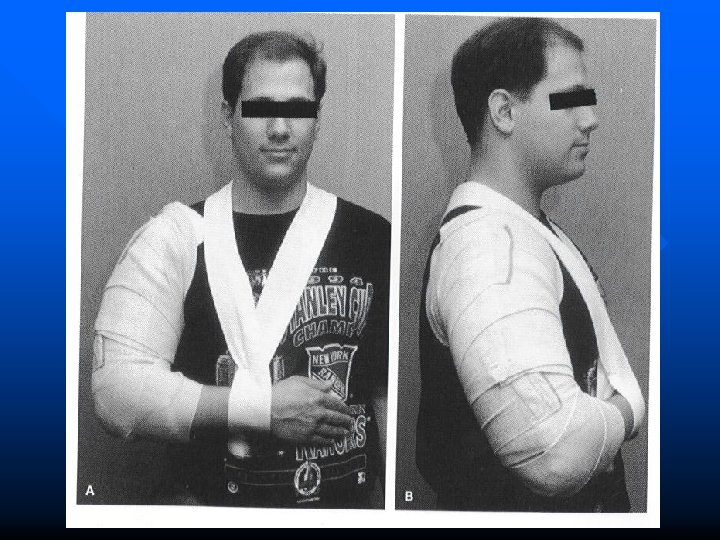
Modified U splint Fractures with minimal shortening n Can be exchanged for functional brace 2 weeks after injury n Disadvantages: lost shoulder movement, axillary irritation, patient discomfort and bulkiness n
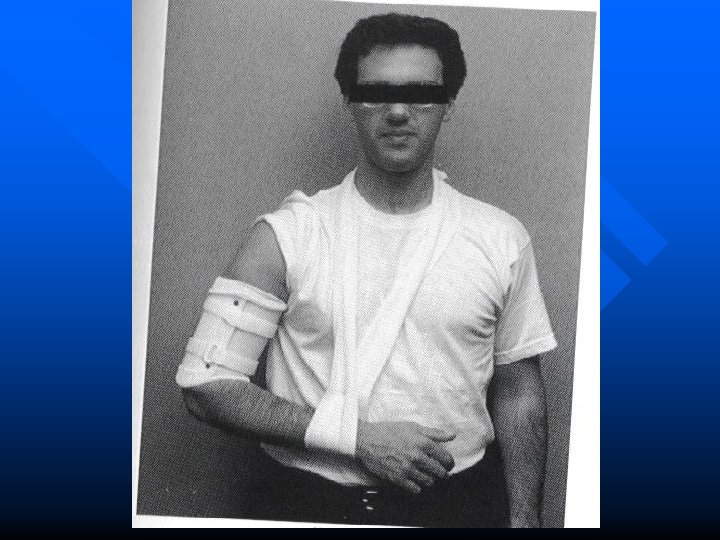
Functional Bracing Fracture reduction through soft tissue compression n Prefabricated anterior shell and posterior shell n Velcro straps n Contraindications: massive soft tissue injury or bone loss, unreliable patient, and inability to maintain alignment n
Indications – surgery (radial nerve palsy) Open fractures n Holstein-Lewis distal 1/3 fractures n Secondary palsies developing after closed reduction n
ELBOW DISLOCATION A FALL ON THE ELBOW n MOST COMMON POST LATERAL n DEFORMITY OBVIOUS n NEURO VASCULAR EXAM n X-RAY n
ELBOW DISLOCATION
ELBOW FRACTURE DISLOCATION
COMPLICATIONS ASSOCIATED FRACTURES RADIAL HEAD CORONOID OLECRANON MEDIAL EPICONDYLE n HETEROTOPIC BONE FORMATION n NEUROVASCULAR n RECURRENT DISLOCATION n STIFF ELBOW n
TREATMENT GENTLE TRACTION WITH COUNTERTRACTION n CORRECT MEDIAL/ LATERAL DISPLACEMENT n ELBOW FLEXED WHILE GUIDING OLECRANON REDUCTON n
CLOSED REDUCTION ELBOW
THE END THANK YOU