Fracture dislocation of the elbow AO Trauma Advanced

Fracture dislocation of the elbow AO Trauma Advanced Principles Course

Learning objectives • Understand the different types of elbow dislocations • Identify subtle signs of complex elbow injuries • Create surgical tactics based upon the injury type • DO NOTHING THAT INCREASES INSTABILITY

AO/OTA Classification Proximal Radius and Ulna 2 R 1 A 2 R 1 B 2 R 1 C 2 U 1 A 2 U 1 B 2 U 1 C 2 R 1 A Radius, proximal end segment, extraarticular fracture 2 U 1 A Ulna, proximal end segment, extraarticular fracture 2 R 1 B Radius, proximal end segment, extraarticular fracture 2 U 1 B Ulna, proximal end segment, partial articular fracture 2 R 1 C Radius, proximal end segment, complete articular fracture 2 U 1 C Ulna, proximal end segment, complete articular fracture Further Elbow dislocation can be classified with the help of list of universal modifiers

Elbow dislocation

Elbow dislocation • Traditional treatment: closed reduction • Active range of motion can reduce slight subluxation through use of muscles around elbow Courtesy of David Ring

Elbow dislocation Failure to maintain reduction: • Consider interposed tissue or incarcerated bony/cartilaginous fragments • Severe soft-tissue damage (avulsion of common flexor/extensor origins) may increase instability • CT scan may be helpful • Consider ligamentous and tendinous repair

Elbow dislocation

The “gang of four” • Terrible triad fracture dislocation • Transolecranon fracture dislocation • Monteggia variant fracture dislocation • Varus posteromedial fracture dislocation

Case 1



Terrible triad fracture dislocation • Historically poor outcomes • Injury “triad”: • Elbow dislocation (often posterior) • Radial head fracture • Coronoid fracture

Terrible triad • Treatment principles: • Repair coronoid/anterior capsular attachment • Repair or replace radial head • Repair LCL • NEVER CREATE MORE INSTABILITY: • Ignore “small” (fleck) coronoid fractures: • These are NOT “avulsion” fractures by brachialis, as radiologists often like to say on their x-ray reads • Resect radial head without replacing it • MCL does not usually need operative repair
 • LCL often avulsed from")
Terrible triad—tactic • Kocher approach to elbow (ECU-anconeus interval) • LCL often avulsed from lateral epicondyle: • “Bare epicondyle” • If resecting the radial head, do it now to improve access to coronoid ECU = extensor carpi ulnaris

Terrible triad—tactic • Repair coronoid or anterior capsule: • Suture tunnels through proximal ulna • Screws • Consider medial approach for plating type III coronoid fractures • Complete repair or replacement of radial head • Repair LCL during closure Regan et al (Orthopaedics. 1992; 15: 845– 848)


Case 2

Transolecranon fracture dislocation • Not a simple olecranon fracture • Do not treat with tension band wiring • Olecranon fracture with ANTERIOR dislocation but intact proximal radioulnar joint • Ligaments may be intact
")
Transolecranon—tactic • Extensile posterior exposure • Full-thickness cutaneous flaps: • Can access Kocher (ECUanconeus) interval for radial head repair/replacement if necessary

Transolecranon—tactic • Address coronoid fractures through olecranon fracture line • Anatomically reduce olecranon • Plate-and-screw constructs are often necessary (no tension band) • Normally, ligaments are relatively spared



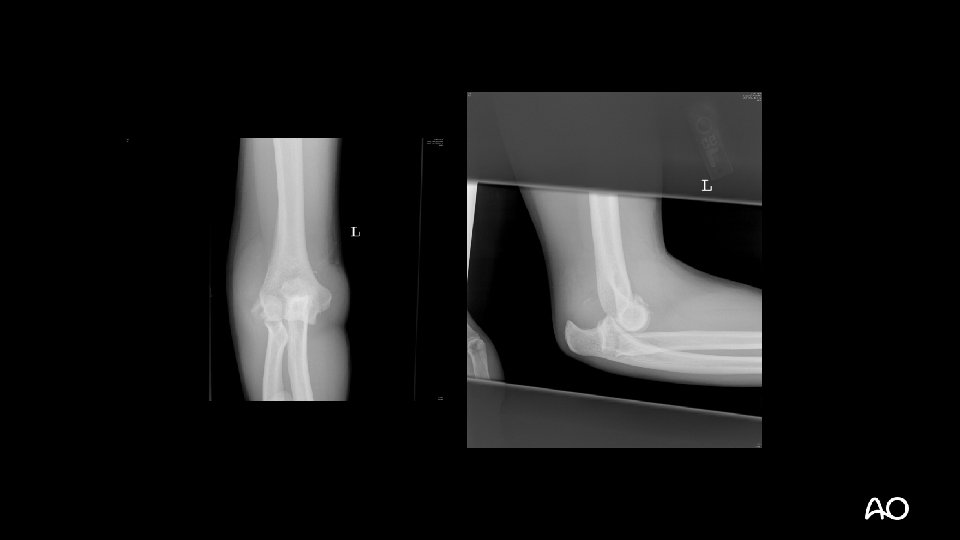
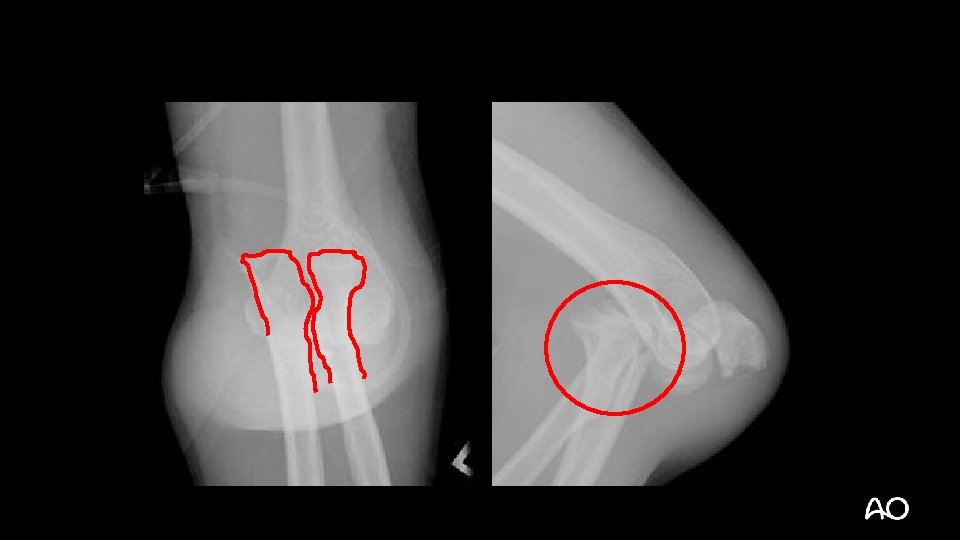
Case 3

Monteggia variant fracture dislocation • Most often posterior dislocations with associated proximal ulnar/olecranon fractures • May have associated radial head fractures • Principles are similar to treatment of standard Monteggia injuries of forearm

Monteggia variant—tactic • Principle: anatomical reduction of ulna is critical for maintenance of radial head reduction • Extensile posterior approach: • Can get to radial head for repair if necessary



Case 4


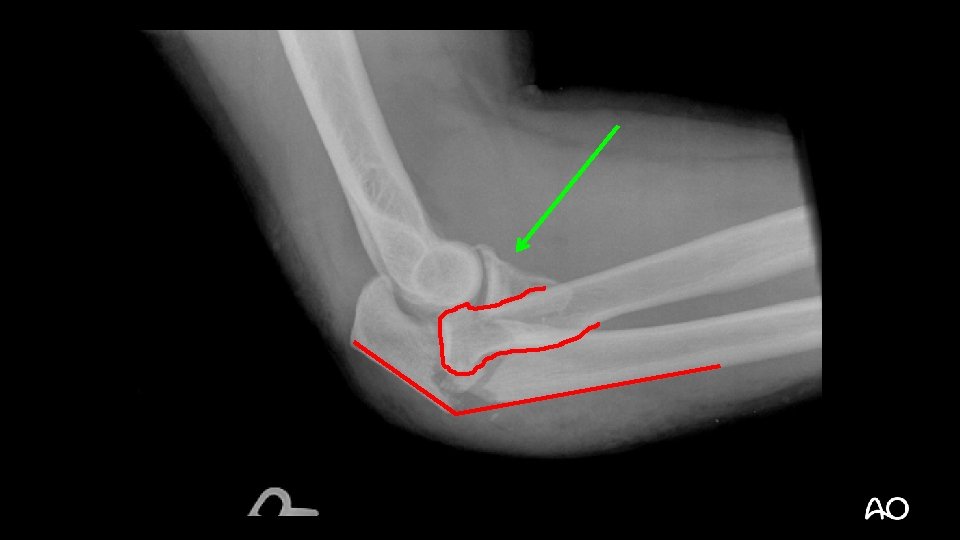
Varus posteromedial fracture dislocation • Recently described injury pattern • Failure to recognize can result in poor outcomes (arthrosis) • Easy to overlook (occasionally small coronoid fractures)

Varus posteromedial fracture dislocation Courtesy of David Ring • Stress views demonstrate that the LCL is ruptured and the elbow is unstable • Results can be poor without operative treatment

Varus posteromedial fracture dislocation—surgical tactic • Medial approach to elbow: • Split FCU, mobilize ulnar nerve • Sacrifice first motor branch? (Paulos et al [Surg Radiol Anat. 2015; 37: 1043– 1048]) • Dissect anterior to MCL • Buttress plating +/- lag screw(s) for coronoid • Stress elbow and repair LCL if instability remains: • Kocher approach

Varus posteromedial fracture dislocation





Not all fit into the “gang of four”

Not all fit into the “gang of four”

Be on the lookout for combined injuries
")
Take-home messages • Four main types of fracture dislocations (other odd ones exist too) • Look for subtle signs of complex elbow injuries • Create a surgical tactic that accomplishes your goal • DO NOTHING THAT INCREASES INSTABILITY— The radial head is more important than you may think
- Slides: 44