Formation of body cavities development of the serous

Formation of body cavities, development of the serous membranes Mark Kozsurek, M. D. , Ph. D. ED I. , 21/03/2019

• Appearance of the common pericardio-pleuro-peritoneal cavity. • Isolation of the pleural and peritoneal cavities: the formation of the diaphragm. • Isolation of the pericardiac and pleural cavities. • Further development of the pericardium, pleura and peritoneum.
 Appearance of the common pericardiopleuro-peritoneal cavity Back to the 2 nd week: bilaminar")
A) Appearance of the common pericardiopleuro-peritoneal cavity Back to the 2 nd week: bilaminar embryonic disk composed of epiblasts and hypoblasts During the 3 rd week: proliferation of epiblasts results in gastrulation

Gastrulation: junctions among epiblasts become looser and due to the collision at the primitive node and primitive streak epiblasts sink below their original layer. Some of them replace the hypoblasts and differentiate into the ultimate endoderm, while others, the mesoblasts, form a third, middle layer, the intraembryonic mesoderm. Epiblast remaining in their original layer will form the ectoderm.

Initially the intraembryonic mesoderm is just a homogenous mass of tissue on the two sides of the notochord. Later a mediolateral differentiation gives arise to the somites, intermediate mesoderm and the lateral plate. Within the lateral plate cavities form and merge resulting in the isolation of the somatic (parietal) and splanchnic (visceral) layer of lateral plate mesoderm.

Oropharyngeal membrane Somatic and splanchnic layers of the lateral plate mesoderm enclose the horse-shoe shaped (or simply „U”-shaped) intraembryonic coelom, which posteriorly on the lateral sides of the embyo communicates with the extraembryonic coelom. With the further growth of the embryo the intraembryonic coelom will dilate anteriorly (the curve of U - future pericardium), the proximal limb of U remains narrow (pericardioperitoneal canal - the future pleural cavity), while the volume of the distal limb of U also increases (future peritoneal cavity).
 future")
Isolated intraembryonic coelom Oropharyngeal membrane future pericardiac cavity pericardioperitoneal canals (future pleural cavities) future peritoneal cavity connections between the intraand extraembryonic cavities

Oropharyngeal membrane A A B B In section B it is well seen that the extraembryonic mesoderm is continuous with the intraembryonic one, extra- and intraembryonic coeloms communicate.

During the 4 th week: folding of the embryo has the highest impact on the furter development of the intraembryonic cavity: heart primordium moves onto the ventral side of the embryo, septum transversum turns into the transverse plane caudal to the heart.

As a result of folding of the embryo the left and right limbs of the intraembryonic coelom get closer to the midline and to each other and at the same time, following the movements of the heart primordium, the dilated curve of the U-shaped tunnel turns onto the ventral side of the embryo. But at this stage the further pericardiac, pleural and peritoneal cavities are not isolated from one other (common pericardiaco-pleuro-peritoneal space).
 Isolation of the pleural and peritoneal cavities: the formation of the diaphragm Note")
B) Isolation of the pleural and peritoneal cavities: the formation of the diaphragm Note the central tendon and the sternal, costal, lumbar parts of the diaphragm. How is it made?

The narrow pericardiacoperitoneal canals are found behind the septum transversum. There are four structures contributing to the diaphragm: 1. septum transversum 2. pleuroperitoneal membranes – as they grow the pericardiaco-peritoneal canal narrows 3. dorsal mesentery of the esophagus – surrounds the aorta, the esophagus and the IVC 4. muscular ingrowth from body wall

septum transversum pleuroperitoneal folds esophageal mesentery muscular ingrowth Myoblast from C 3 -C 5 myotomes migrate into the septum transversum and take their nerve with themselves (phrenic nerve). But lower intercostal nerves also contribute to the innervation of the periphery of the diaphragm formed by the muscular ingrowth of the body wall.

Congenital diaphragmatic hernia Incomplete fusion of the four parts. Stomach and/or intestine ascend into the thoracic cage and compress the lungs.
 Isolation of the pericardiac and pleural cavities Formation of the diaphragm have isolated")
C) Isolation of the pericardiac and pleural cavities Formation of the diaphragm have isolated peritoneal cavity from the pericardiacopleural space. Diaphragm C 3 -C 5 common cardinal vein, phrenic nerve As the heart tube loops its caudal end with the common cardinal veins moves upward and the phrenic nerves migrate toward the midline forming the pleuropericardial fold.

Due to the changing position of the phrenic nerve and the common cardinal vein, the pleuropericardial membrane appears, which later completly isolates pleural and pericardiac cavities.

Summary 1. The most anterior part, the loop of the intraembryonic coelom gives the pericardial cavity enclosing the heart. 2. Rostral limbs of the intraembryonic coelom do not unite in the midline and as a result of this, two non-communicating, left and right pleural cavities develop. 3. Caudal limbs of the intraembryonic coelom remain paired structures anteriorly but they merge caudally. This explains why the ventral mesentery is only observable in the upper onethird of the abdominal cavity, while the dorsal mesentery exists along the whole length of it.
 Further development of the pericardium As the heart tube loops, its arterious and")
D) Further development of the pericardium As the heart tube loops, its arterious and venous ends approach each other. Pericardial reflections (visceral layer – parietal layer transition) are found around both ends. Between the two reflections the transverse sinus (T) is found.
 Further development of the pleura Developing lungs grow into the left and right")
E) Further development of the pleura Developing lungs grow into the left and right pleural cavities. Transition between the visceral and parietal layers (pleural reflection) surrounds the root of lung and descents to the diaphragm as the pulmonary ligament
 Further development of the peritoneum")
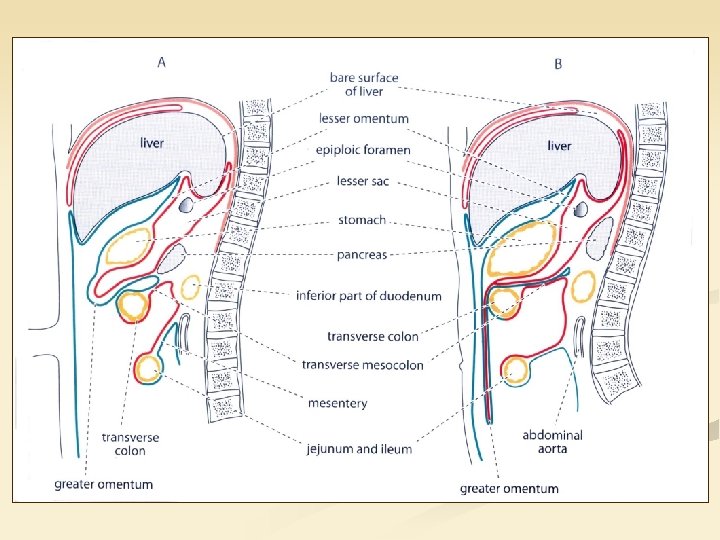
E) Further development of the peritoneum

A 3 D model of the peritoneal cavity demonstrating that in the upper one-third the left and right body cavities remain separated (both ventral and dorsal mesogastrium is seen), but caudally they merge and only the dorsal mesentery persists.

right left In the upper one-third of the abdominal cavity the liver and the spleen develops within the ventral and dorsal mesogastrium, respectively. As the result of the rotation of the foregut and related transposition of epigastric structures, the lesser sac or the omental bursa appears. According to the colour code that is derived from the right body cavity (Please note, that the sides are not labelled correctly in Prof. Réthelyi’s Functional anatomy textbook).

Thank you for your attention!
- Slides: 24