FORENSIC SOCIAL WORK IN THE JUVENILE JUSTICE FIELD



 � Forensic social work is the")





 is an independent, scientific, and")







 -")


 abstract")
 recommends that children and youths who enter the")


 is to reduce the recidivism rate of the juveniles detained at")




 (1094) (1008) (48. 49% IS THE AVERAGE NUMBER OF INTAKES")
 (1094) 151 (1019) (1008) THE PERCENTAGE OF")
 YOUTH WHO(1019)")
 (1145) (1094) (1008)")
 SERVICES (ASSESSMENT, CRISIS INTERVENTION, BRIEF THERAPY, ETC)")














- Slides: 49
FORENSIC SOCIAL WORK IN THE JUVENILE JUSTICE FIELD IN ARKANSAS AR NASW Conference Hot Springs, AR April 5, 2012 Compiled by Shelley Clingan, BSW, MSW, LCSW, CCDP-D, RTC (Forensic) Social Worker Washington County Juvenile Detention Center 885 Clydesdale Fayetteville AR 72701 (479) 444 -1670 ext 29 sclingan@co. washington. ar. us HTTP: //WWW. CO. WASHINGTON. AR. US
� Background � Housekeeping – *temperature *bathrooms *cell phones *timekeeper � Content Overview and eliciting expectations
The purpose to this workshop is to explore the dynamics and potential for impact of Social Work in the Juvenile Justice field in Arkansas by taking a closer look at the role of the Social Work Intervention Program at the Washington County Juvenile Detention Center and the statistical outcomes of this program.
� National Organization for Forensic Social Workers (NOFSW) � Forensic social work is the application of social work to questions and issues relating to law and legal systems. This specialty of our profession goes far beyond clinics and psychiatric hospitals for criminal defendants being evaluated and treated on issues of competency and responsibility. � A broader definition includes social work practice which in any way is related to legal issues and litigation, both criminal and civil. Child custody issues, involving separation, divorce, neglect, termination of parental rights, the implications of child and spouse abuse, juvenile and adult justice services, corrections, and mandated treatment all fall under this definition.
� Can any social worker be a forensic social worker? � Forensic social work is based on specialized knowledge drawn from established principles and their application, familiarity with the law, painstaking evaluation, and objective criteria associated with treatment outcomes. What the social worker offers must be of utility and couched in language to which the court can relate. The conclusions and recommendations must withstand critical review and rebuttal from opposing parties. � The training of social work practitioners has not traditionally included familiarity with the adversary process nor the issues that civil and criminal justice systems confront. Without such training, social workers called onto provide forensic services may find themselves at a disadvantage.
� Functions of the forensic social work practitioner may include… �Providing consultation, education, or training to: Criminal justice, juvenile justice, and correctional systems Law makers Law enforcement personnel Attorneys, law students, and paralegals Members of the public
� Functions of the forensic social work practitioner may include… �Diagnosis, treatment, and recommendations: Diagnosing, assessing, and treating criminal and juvenile justice populations Diagnosing, treating, or making recommendations about mental status, childrens’ interests, incapacities, or inability to testify Serving as an expert witness Screening, evaluating, or treating law enforcement and other criminal justice personnel
� Functions of the forensic social work practitioner may include… �Other functions: Policy and program development Mediation, advocacy, and arbitration Teaching, training, and supervising Behavioral Science Research and Analysis
� Forensic social work practitioners engage only in forensic activities within their areas of competence and expertise. � http: //nofsw. org/
� The American College of Forensic Examiners Institute (ACFEI) is an independent, scientific, and professional association representing 11 different specialty boards, including the American Board of Forensic Social Workers. � Certification �Certified Opportunities Forensic Social Worker, CFSW℠ �Certified Forensic Master Social Worker, CFMSW℠
� Forensic social work is the application of social work to questions and issues relating to the law and legal system, both criminal and civil. � Forensic social workers help children and families involved in custody issues, including but not limited to separation, divorce, neglect, and the termination of parental rights. The social workers also deal with the implications of child and spouse abuse. � Forensic social workers may work in a number of settings, including juvenile and adult justice services, corrections, and mandated treatment programs. � http: //www. abfsw. us/
� History �Initially � Current seen as adults Trends �Developmentally Different than adults Brain developing thru age 24
� Who are the juveniles involved in JJS? Nature vs Nurture? � “Bad Kids” ? � Dysfunctional Families � Mental Health Issues � Educational Issues � Systemic Barriers (DMC; Violent Neighborhoods) � Psychosocial Trauma � Normal Adolescent Development
"There is no single cause of delinquency and violence. Delinquents, especially chronic delinquents, exhibit a variety of social and psychological deficits in their backgrounds. These deficits, often referred to as risk factors, stem from breakdowns in five influential domains in juveniles' lives: neighborhood, family, school, peers, and individual characteristics. . . Some youth lack healthy parental guidance and monitoring. Some youth have cognitive and psychological deficits that make social and academic success difficult. Some attend disorganized and disruptive schools and fail to engage in academic pursuits. Some live in chaotic neighborhoods with few resources or outlets for positive social activities. Some are excluded from prosocial peer groups and have few, if any, wholesome friends. . . These risk factors, particularly when several are present, increase the likelihood of delinquency and violence. Conditions such as maltreatment or neglect by family members and others, a community with a large population of delinquent juveniles and gangs, ready access to drugs and guns, and an unsafe school increase the chance that a youth will make unhealthy or unlawful choices. . . Additionally, when a child's family life is filled with violence, problem behaviors, poor parental monitoring, and inconsistent disciplinary practices or maltreatment, a child's risk of delinquency increases. . . Youth exhibiting combinations of these deficits in multiple domains of their lives are at highest risk of delinquency". OJJDP National Criminal Justice Reference Service report ‘Combating Violence and Delinquency: The National Juvenile Justice Action Plan
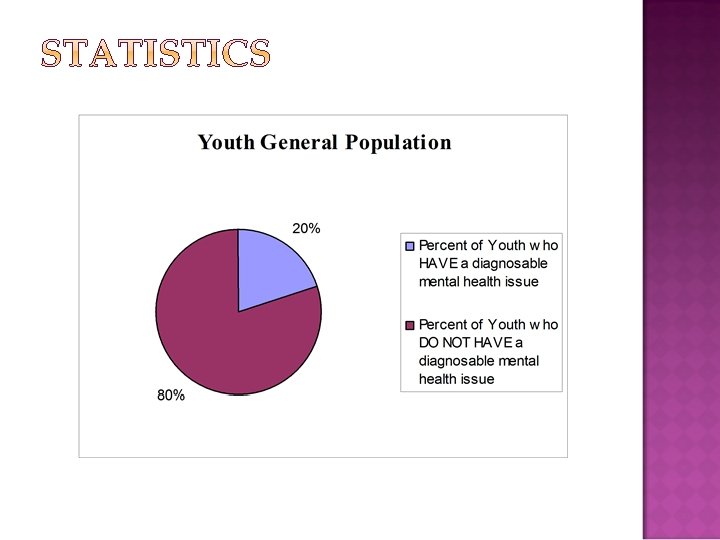
1. The prevalence of mental disorder among youth in the juvenile justice system is two to three times higher among youth in the general population (NCMJJ) 1. Series of studies over the past 5 years have consistently found rates of mental health issues to be between 65% and 70% (some higher) (NCMJJ) 2. Suicide is the 3 rd leading cause of death for 15 -24 year olds, BUT youth suicides in juvenile detention and correctional facilities are more than four times greater than youth suicides in the general public (CJJ)
� � Research consistently shows that 70% of Youth involved in the Juvenile Justice System have diagnosable mental health issues. This number remains high (60%-65%), even when behavior disorders are excluded. (CJJ, OJJDP, NIMH, NCMHJJ)
Ø Research demonstrates that a high proportion of youth in the corrections system have never been identified as having a (learning) disability or have been misidentified (EDJJ, 1999). Ø Experiencing childhood abuse and neglect increases the likelihood of arrest as a juvenile by 53 percent (National Institute of Justice) Ø Girls are three times more likely than boys to be sexually abused, and sexual abuse has been recognized as a cause of mental health disorders. Sexual abuse is also related to increased truancy, prostitution and violence, among other destructive behaviors
Ø Nearly half of incarcerated girls meet criteria for posttraumatic stress disorder (PTSD) - (National Mental Health Association) Ø Up to two-thirds of children who have mental illnesses and are involved with the juvenile justice system have cooccurring substance abuse disorders, making their diagnosis and treatment needs more complex (National Mental Health Association)
� Emotional, behavioral, and mental health issues, learning and developmental disabilities, cognitive impairment, substance abuse issues, and traumatic psychosocial factors effecting functioning in Youth who are involved in the juvenile justice system are disproportionately high compared to the general population and significantly effect accountability for youth involved in the juvenile justice system. Additionally, the Youth and their families also face barriers in navigating the mental health, educational, and social services systems to obtain the resources and interventions needed to address these issues. (Shelley Clingan) � For numerous reasons, these dynamic issues are often misidentified, unidentified, or unaddressed resulting in repeated involvement with the juvenile justice system (Coalition for Juvenile Justice; National Center on Education, Disability, and Juvenile Justice; Office of Juvenile Justice and Delinquency Prevention).
The most successful mental health programs —those that treat young offenders in their families and communities— reduce recidivism up to 80% (CJJ)
According to the Social Work Speaks (National Association of Social Workers Policy Statements) abstract for Juvenile Justice and Delinquency Prevention: Public demand to get “tough on crime” has undermined the key concept of the juvenile court system — that children are developmentally different from adults and therefore more amenable to treatment and rehabilitation.
National Association of Social Workers (NASW) recommends that children and youths who enter the juvenile justice system be treated differently from adults through every phase, including: �Prevention �Early intervention �Diversion �Detention �Probation �Residential care �Incarceration �Postrelease care
Children who do not receive… Effective and responsive screening § Assessment § Treatment § Aftercare protocol § progressively move through stages of delinquency development and ongoing adult criminal behavior
� � � Legislative changes in 1995 allowed juvenile judges to sentence Youth to local detention centers for up to 90 days The Arkansas Juvenile Code mandates that mental health needs are addressed within Detention facilities. 1995 SWIP est. utilizing interns from U of A and supervision funded by JABG monies In 2004, the Washington County Quorum Court had the insight to determine that it would be more economical and beneficial to hire a full time professional to provide on-site services. The Social Work Intervention Program (SWIP) not only addresses the Juvenile Code standard, but currently also plays a role statistically in the reduction of recidivism for the Juveniles of NWA and a reduction in the commitment rate to the AR Division of Youth Services.
The goal (vision) is to reduce the recidivism rate of the juveniles detained at the Regional Detention Center by providing supportive and empowering services Social Work Intervention Program (SWIP) crisis intervention Therapy services behavior modification recommendations screenings Services Provided referrals and case management assessments Non-profit program SWIP is used per referral from the County Judge, court staff, detention staff, and/or by triage services
� MISSION STATEMENT THE PURPOSE OF THE SOCIAL WORK INTERVENTION PROGRAM IS TO PROVIDE CASE MANAGEMENT SUPPORT AND CLINICAL SOCIAL WORK SERVICES TO ASSIST RESIDENTS DETAINED AT THE REGIONAL JUVENILE DETENTION CENTER, MEET THEIR PHYSICAL, MENTAL, EMOTIONAL, AND SPIRITUAL NEEDS THROUGH CULTURALLY COMPETENT AND GENDER SPECIFIC PRACTICE. THE PROVISION OF THESE SERVICES IS A COLLABORATIVE EFFORT WITH THE DETENTION PROGRAMMING TO ENSURE THAT THE JUVENILES DETAINED AT THE CENTER ARE OFFERED A REHABILITATIVE EXPERIENCE. � Funding
micro mezzo macro � A primary service of the program is completing court ordered multi systems life course assessments (evaluating the biological, psychological, social, spiritual, cultural, and generational functioning across various domains and systems to include the environmental impact of traumatic incidents on psychosocial development) of juveniles who are detained and then making recommendations to the AR Fourth Judicial District Circuit Chancery Court, Juvenile Division about the needs of the juveniles, with subsequent referral and case management assistance to obtain services. The program also provides assessments for acuity and referral for acute hospitalization, crisis intervention, counseling, brief therapy, psychoeducational/therapeutic groups, resource linkage and referral services for the juveniles and their families, and supportive services to detention and SWIP staff.
� Developmental, Cognitive, Mental Health, & Behavioral Functioning � Trauma / Psychosocial Experiences � Family Dynamics � Educational Implications � Gender Specific Programming � Diversity paradigms � Medical Needs / Organic Factors � Risk & Resiliency Factors
SWIP SERVICES STATISTICS (1145) (1094) (1008) (48. 49% IS THE AVERAGE NUMBER OF INTAKES AND STATUS CHANGES WHO RECEIVED SWIP SERVICES JUNE 2007 – DECEMBER 2011 19)
SWIP SERVICES STATISTICS 272 229 218 (1145) (1094) 151 (1019) (1008) THE PERCENTAGE OF YOUTH RECEIVING SERVICES HAS INCREASED OVER THE YEARS AS THE NUMBER OF INTAKES AND STATUS CHANGES HAS DECREASED.
WASHINGTON COUNTY HAS HAD A 23% DECREASE IN THE NUMBER OF (1145) YOUTH WHO(1019) COMPLETED AN INTAKE(1094) OR STATUS (1008) CHANGE AT THE WASHINGTON COUNTY JUVENILE DETENTION CENTER FROM 2004 TO 2011. THIS DECREASE SUGGESTS A CORRELATION TO THE EFFECTIVENESS OF THE DIVERSION PROGRAMMING, SWIP, AND TREND TOWARD REFORM IN JUVENILE JUSTICE SYSTEM
SWIP SERVICES STATISTICS (1019) (1145) (1094) (1008)
SWIP SERVICES STATISTICS 3, 744 SWIP (CLINICAL) SERVICES (ASSESSMENT, CRISIS INTERVENTION, BRIEF THERAPY, ETC) WERE PROVIDED TO SWIP (1019) (1145) (1094) 2011(1008) YOUTH IN JDC FROM JULY 2007 – DECEMBER
SWIP SERVICES STATISTICS Without controlling for extraneous variables, the SWIP program shows a 16% recidivism rate of juveniles who returned to detention after receiving SWIP services beyond group attendance for the timeframe of Jan – Dec 2011 which, while although preliminary, is promising when compared to the nearly 60% recidivism rate defined as re-referral to juvenile court by age 18 (1019) (1145) (1094) (1008) quoted in the OJJDP “Juvenile Offenders and Victims: 2006 National Report”.
SWIP SERVICES STATISTICS HOWEVER, LONGITUDINAL STUDY IS REQUIRED TO EFFECTIVELY ASSESS THE EFFICACY OF THE SWIP PROGRAM. MANY OF THE JUVENILES WHO DID RETURN TO DETENTION SHOWED SUBJECTIVE SUCCESS IN FUNCTIONING, AND MOST OF THE JUVENILES HIGHLIGHTED FAMILY DYSFUNCTION; FACED SYSTEMIC BARRIERS, SUCH AS LACK OF AVAILABLE SERVICES, FUNDING ISSUES, OR LONG WAITING LISTS FOR OUTPATIENT/INPATIENT SERVICES; AND/OR THE JUVENILES PROVED THAT THEY NEEDED MORE RESTRICTIVE INTERVENTIONS THAN ORIGINALLY RECOMMENDED AS LEAST RESTRICTIVE INTERVENTIONS WHICH ARE ETHICALLY MANDATED WHEN INITIATING SERVICES (FOR EXAMPLE JUVENILES WHO CONTINUED TO USE DRUGS DESPITE ADVERSE CONSEQUENCES PROVED THAT THEY NEEDED DRUG REHAB, RATHER THAN (1019) CLINICAL (1145) SERVICES). (1094) (1008) OUTPATIENT
JDC Recidivism of Intakes* 359 358 329 325 263 *Same Calendar Year
JDC Recidivism of Intakes* 60% OJJDP Cross Analysis 2006 263 *Same Calendar Year
60% OJJDP Cross Analysis 2006 263
60% OJJDP Cross Analysis 2006 � According to the Arkansas Department of Human Services, Division of Youth Services Statistics, overall DYS had a decrease of 26. 92% in the number of commitments from all Counties in the State for the time period of 2005 to 2011, which suggests reform efforts and a trend of juvenile justice being administered locally. However, 263 in population, juvenile Washington County, one of the largest Counties in the State population, and area, had the largest decrease at 80. 49% in DYS Commitments from 2005 to 2011 of the top ten largest counties. This sizeable decrease may help to support the hypothesis that on-site clinical services and programming, like those offered by the Social Work Intervention Program (SWIP) in Washington County, are effective with our youth and their families. � The Social Work Intervention Program, not only provides on-site clinical services, but also helps families to navigate and address barriers in the mental health, educational, and social services systems that previously resulted in commitments to the AR Division of Youth Services to address. The Court allows and encourages the Social Work Intervention Program and Court Staff to have this role in exhausting local resources and utilizes commitment to DYS as a last resort. � The most populous Counties with the largest decrease of commitments to DYS have access to clinical programming. Benton County (72. 41% decrease) had the third largest decrease and has licensed Clinicians (LPC/LCSW) in both their JDC and on Courtside. Pulaski County (75. 15% decrease), Sebastian (20%), and Faulkner County (14. 29% decrease) are also showing significant decreases as part of the ten largest populated Counties in the State.
Future Goals • Program expanded to allow more on-site interventions, groups, vocational, 1: 1 therapy • 100% of Youth entering JDC receive SWIP (on-site clinical) Services • Youth do not have to enter JDC to receive SWIP (on-site clinical) Services (ie Youth can receive services on court side) and FINS families can also receive SWIP services • Youth and their families have a case manager follow them to assist with system navigation and resource linkage and referral throughout the time that they are involved in the juvenile justice system • Expand services to court side • More preventative services (crisis oriented) • Aftercare plans and case management to follow through SOC • Longitudinal Study to replicate effectiveness • Database
� Wrap Up � Q&A � Satisfaction � CODE Survey
� 15 Y. O. ALICE HAS CONTINUOUSLY ELOPED FROM HOME, USED MARIJUANA WITH HER MOM, AND IS PROMISCUOUS (FOR HER, A FORM OF POST TRAUMATIC STRESS DISORDER). SHE HAS MENTAL HEALTH DIAGNOSES OF ADHD AND BI-POLAR DISORDER AND HAS BEGUN TO DEVELOP TRAITS OF A PERSONALITY DISORDER. IN APRIL, SHE TOOK PILLS IN A SUICIDE ATTEMPT TO OVERDOSE AND HAS A HISTORY OF SELF-MUTILATION. SHE RECENTLY MADE ALLEGATIONS OF RAPE AGAINST TWO MALES. IN APRIL, SHE TESTED POSITIVE FOR MARIJUANA AND COCAINE. SHE HAS BEEN IN AND OUT OF FOSTER CARE FOR ABUSE AND NEGLECT ISSUES, INCLUDING BEING SEXUALLY ABUSED AS A YOUNG GIRL. SHE HAS OFTEN TAKEN ON THE PARENTIFIED ROLE WITH HER MOM. SHE WAS RECENTLY UNSUCCESSFULLY DISCHARGED FROM HER INPATIENT SUBSTANCE ABUSE TREATMENT PROGRAM AND IS CURRENTLY WAITING TO ENTER A LONG TERM RESIDENTIAL TREATMENT PROGRAM.
� 17 y. o. Mike has mild mental retardation. He was held back in 1 st grade. his diagnoses include depression, adhd, sexual abuse of child (victim), cannabis abuse, and a tic disorder. He has been sexually abused twice – at age 4 and age 14 and has a conflictual relationship with his 18 yo brother who is a negative influence on him. He reportedly was made to do sexual acts with his brother at age 4. He reported having significant issues with anger and violence and burns his arms when “bored”. Last month he learned the person that he believed to be his biological dad is not his dad and that his biological dad has already passed away. He spent about 8 months in dhs custody at age 7 due to drug use of mom and her boyfriend. He has been acutely hospitalized 5 times for suicidal thoughts. His legal charges have included shoplifting a wallet, loitering, and possession of marijuana. He does not have any planning or services in place for independent living skills, housing, or ways to make a living after he turns 18 yo.
� 17 y. o. Mike has mild mental retardation. He was held back in 1 st grade. his diagnoses include depression, adhd, sexual abuse of child (victim), cannabis abuse, and a tic disorder. He has been sexually abused twice – at age 4 and age 14 and has a conflictual relationship with his 18 yo brother who is a negative influence on him. He reportedly was made to do sexual acts with his brother at age 4. He reported having significant issues with anger and violence and burns his arms when “bored”. Last month he learned the person that he believed to be his biological dad is not his dad and that his biological dad has already passed away. He spent about 8 months in dhs custody at age 7 due to drug use of mom and her boyfriend. He has been acutely hospitalized 5 times for suicidal thoughts. His legal charges have included shoplifting a wallet, loitering, and possession of marijuana. He does not have any planning or services in place for independent living skills, housing, or ways to make a living after he turns 18 yo.
� 16 Y. O. JAKE WHOSE DIAGNOSES INCLUDE BI-POLAR DISORDER, SEXUAL ABUSE OF CHILD (VICTIM), POST TRAUMATIC STRESS DISORDER, AND SEXUAL ABUSE OF CHILD (PERPETRATOR) HAS NOT BEEN ON HIS MEDICATION IN ABOUT 6 MONTHS, AND HE HAS A NEW CHARGE FOR SEXUALLY ACTING OUT …. � 16 Y. O. MITCHELL HASN’T SEEN HIS MOM SINCE HE WAS 7. HE LIVES WITH HIS DAD WHO WORKS DILIGENTLY TO MAKE SURE MITCHELL RECEIVES TREATMENT. MITCHELL HAS A HISTORY OF ACUTE HOSPITALIZATIONS FOR SUICIDAL IDEATIONS AND OF OUTPATIENT CLINICAL SERVICES FOR ADHD, BEHAVIOR ISSUES, AND DRUG AND ALCOHOL PROBLEMS HAS MADE A SUICIDAL GESTURE AND INDICATED THAT HE WANTS TO KILL HIMSELF … � 15 Y. O. ALVIN HAS A HISTORY OF BEING DIAGNOSED WITH BIPOLAR DISORDER, SEXUAL ABUSE OF CHILD (VICTIM), AND POST TRAUMATIC STRESS DISORDER AND HAS EXHAUSTED MANY ACUTE AND RESIDENTIAL TREATMENT PROGRAMS BUT HIS RECENT DISCHARGE FROM THE ARKANSAS STATE HOSPITAL INDICATES THAT HE IS TOO AGGRESSIVE TO RETURN HOME. HE HAS TRAITS OF A PERSONALITY DISORDER ALREADY FORMING …
� 15 Y. O. JACOB WHO HAS A BABY WITH HIS GIRLFRIEND BUT HAS GRADUATED FROM MARIJUANA TO USING METHAMPHETAMINE. HE HAS A HISTORY OF DEPRESSION AND OF SELF-MUTILATION. THERE IS A HISTORY OF SIGNIFICANT SUBSTANCE USE IN HIS FAMILY … � 16 Y. O. SARA HAS BEEN USING IV (NEEDLE) METHAMPHETAMINE. SHE NEEDS TO RECEIVE INPATIENT DRUG AND ALCOHOL TREATMENT (REHAB) AND NEEDS ASSISTANCE WITH OBTAINING A PCP REFERRAL, PHYSICAL EVALUATION, AND STD TESTING … � 15 Y. O. RON HAS RESIDED WITH HIS GRANDPARENTS SINCE AGE 4. HIS BIOLOGICAL MOTHER, WHO WAS REPORTEDLY DIAGNOSED WITH BI-POLAR DISORDER AND “MULTIPLE PERSONALITY DISORDER”, REPORTEDLY USED ILLEGAL DRUGS, INCLUDING METHAMPHETAMINE DURING PREGNANCY AND REPORTEDLY GAVE RON ALCOHOL IN HIS BOTTLE AND BLEW MARIJUANA IN HIS FACE AS AN INFANT/TODDLE TO CALM HIM DOWN …
� 14 Y. O. TODD HAS BEEN HAVING SIGNIFICANT PROBLEMS AT SCHOOL AND IS BECOMING MORE PHYSICALLY AND VERBALL AGGRESSIVE AT HOME. HE HAS A HISTORY OF BEING PICKED ON / BULLIED AT SCHOOL. HE HAS NOW HAD 31 SCHOOL WRITE UPS AND 22 DAYS OF OUT OF SCHOOL SUSPENSION SINCE DECEMBER 2009. HE HAS AN IEP IN SCHOOL FOR BEHAVIOR PROBLEMS. HIS MOTHER AND THERAPIST ARE CONCERNED THAT HE HAS BI-POLAR DISORDER AND IS ON THE AUTISM SPECTRUM (PERVASIVELY DEVELOPMENTALLY DELAYED / ASPERGERS SYNDROME) BUT THIS HAS NOT BEEN DIAGNOSED AND TREATED … � 14 Y. O. DENISE IS 9 MONTHS PREGNANT. SHE HAS ALREADY RECEIVED TREATMENT AT CHILDREN’S HOSPITAL IN LITTLE ROCK DUE TO PROBLEMS WITH HIS HIGH RISK PREGNANCY. HER INVOLVEMENT WITH THE COURT BEGAN FOR NOT GOING TO SCHOOL AND FOR USING MARIJUANA WITH HER BROTHER WHO IS INVOLVED IN A GANG. DENISE WANTS TO KEEP HER BABY TO HAVE SOMEONE TO LOVE.