FOREIGN BODIES IN THE GI TRACT Rajeev Nagpal

FOREIGN BODIES IN THE GI TRACT Rajeev Nagpal M. D.



OBJECTIVES • Common foreign bodies in the GI tract • Clinical symptoms at presentation • Clinical examination findings • How to confirm the diagnosis • Should we remove it or let it pass • How to remove and when to remove it • And lastly how a tooth brush can turn into a shaving razor

CASE HISTORY • 7 WKS OLD MALE • PRESENTED TO THE ER • COUGH AND RUNNY NOSE FOR 2 DAYS • POOR FEEDING FOR 1 DAY • NO HISTORY OF VOMITING • PAST HISTORY UNREMARKABLE

• CHEST X RAY: METALLIC WASHER IN THE ESOPHAGUS • FLEXIBLE/RIGID ENDOSCOPY UNSUCCESSFUL • EDEMA AROUND THE WASHER • WASHER DROPPED INTO THESTOMACH • RETRIEVED AFTER 3 MONTHS, GOLD PLATED


GOLD PLATED WASHER

CLINICAL PRESENTATION • Peak incidence 6 months to 3 yrs • Very uncommon under 6 months • May occur in adolescent age group also • Autistic and also non autistic teenagers • Older children: food bolus common agent

CLINICAL SYMPTOMS • ASYMPTOMATIC • HISTORY OF INGESTION • HODGE ET AL: 31% CASES OF FB IN ESOPHAGUS ASYMPTOMATIC • LOCATION DICTATES THE SYMPTOMS • CHEST XRAY IN ALL CASES WITH A HISTORY

SYMPTOMS UES : DROOLING MID ESOPHAGUS; NS, CHEST PAIN, DYSPH LES : NS, CHEST PAIN, DYSPHAGIA STOMACH, SMALL INTESTINES , COLON NO SYMPTOMS

UPPER ESOPHAGEAL SPHINCTER

CONFIRM THE DIAGNOSIS • CONFIRM WITH CXR FOR RADIO OPAQUE OBJECTS • RADIOLUCENT : CT SCAN VS ENDOSCOPY

MANAGEMENT • SHOULD WE REMOVE IT • WHEN SHOULD WE REMOVE IT • HOW SHOULD WE REMOVE IT

ESOPHAGEAL FB SHOULD WE REMOVE IT Esophageal fbs should be removed: why

MANAGEMENT • OBSTRUCTIVE SYMPTOMS URGENT REMOVAL: ENT • MID/LOWER ESOPHAGUS WAIT • LOWER 3 RD SMOOTH MUSCLE relaxant: GLUCAGON • EGD REMOVAL

GLUCAGON FOR LES RELAXATION Glucagon 1 mg iv

GLUCAGON FOR LOWER ESOPHAGEAL FBS Glucagon 1 mg IV

HOW TO REMOVE • DO NOT FEED THE CHILD • RIGID ENDOSCOPY • FLEXIBLE ENDOSCOPY • FOLEY CATHETER

HOW TO REMOVE • Coin retriever • Rat tooth foceps • Roth Net • Over tube for sharp object

SHARP OBJECTS IN ESOPHAGUS • Sharp objects such as safety pins etc • Remove as soon as possible

FOREIGN BODIES IN STOMACH • Blunt objects less than 2. 5 -3 cm will pass thru May take weeks • Sharp objects should be removed(over tube) • objects in SI, leave it alone • Experimental evidence small bowel dilates when exposed to a sharp object like a pin

LITHIUM BATTERIES Simple round structure

ESOPHAGEAL BATTERY

LITHOUM BATTERIES

BUTTON BATTERIES • Liquefaction necrosis: due to sodium hydroxide produced by the generated current • Perforation has occurred in 6 hrs • 20 mm batteries are 3 V and produce a higher current

MANAGEMENT • Urgent removal • Always in the OR • ENT : rigid scopes are better • Thoracic surgeons; support on site

FOREIGN BODIES: MAGNETS If it looks pretty, it’s a toy, and if it’s little, it might be candy. Young children will put anything in their mouths, including shiny, highly powerful magnets smaller than a pea
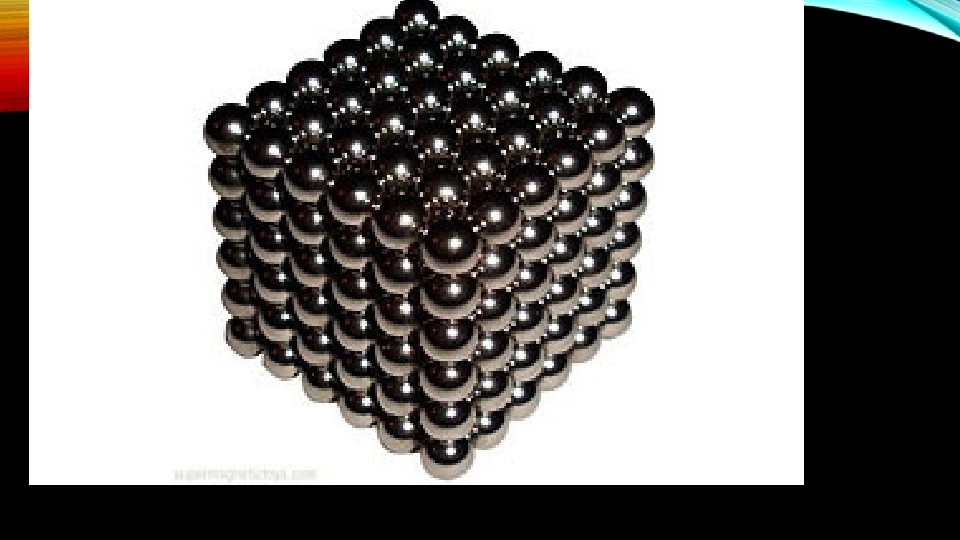
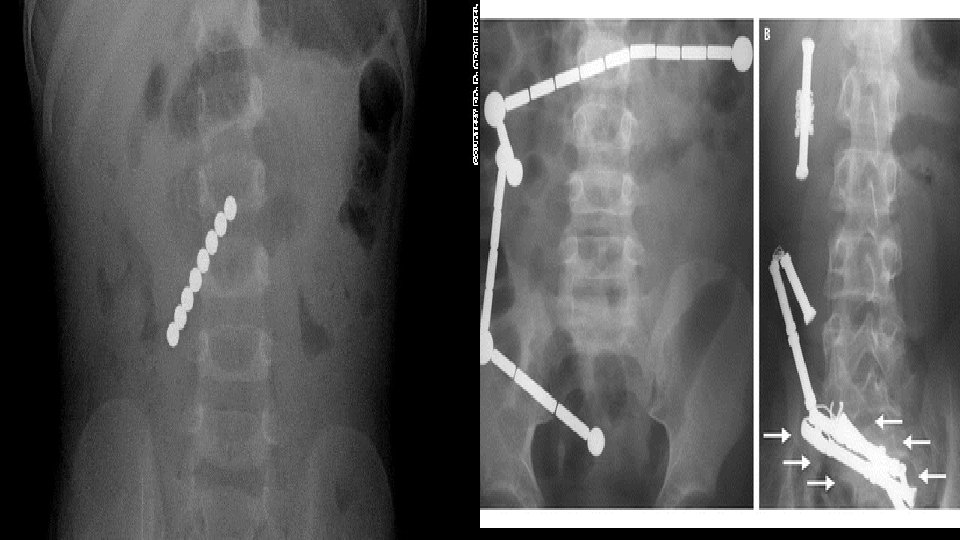

MAGNETS • WHEN INGESTED AS A SINGLE MAGNET: NO RISK • MORE THAN ONE MAGENT • OBSTRUCTION • PERFORATION
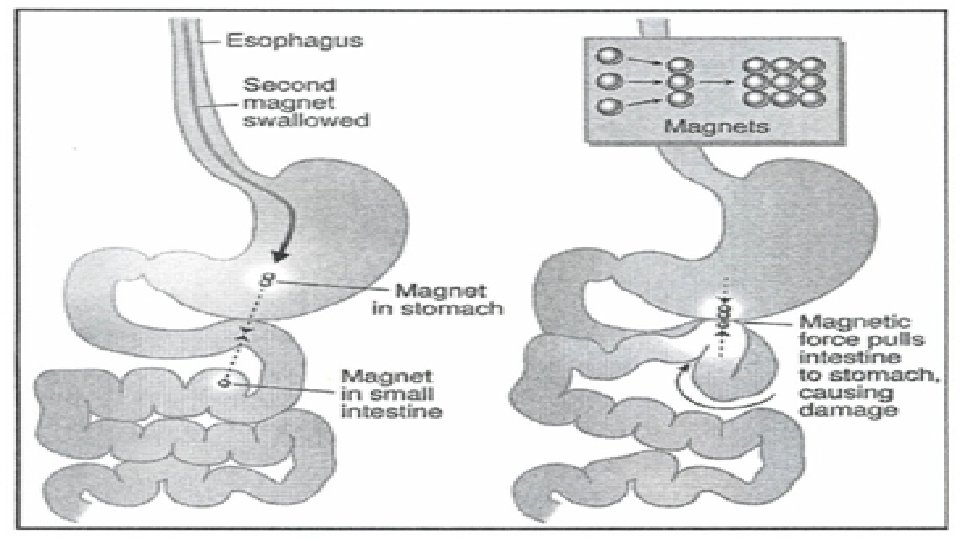

MAGNETS • ENSURE THAT THE MAGNET IS STILL IN THE STOMACH • ENSURE SURGICAL SUPPORT

A TOOTHBRUSH TURNED INTO A RAZOR • • • 16 yrs old female Swallowed her tooth brush She was really trying to clean her wisdom teeth Asymptomatic ER : CAT scan showed a tooth brush like structure in the stomach Under GA, with a over tube , we struggled to pull out it out, with surgeons as standby • It was the oddest tooth brush we had seen
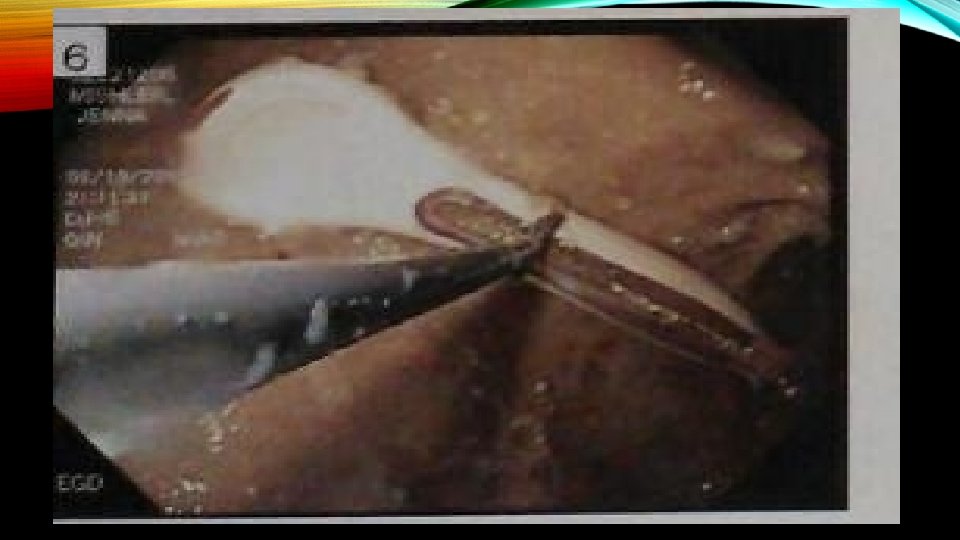


FOREIGN BODIES • We presented the razor to the parents • But where is the tooth brush ?
- Slides: 38