Food allergy in adults whats new on the





 Ø")





 2000/2001 (129) Medication 44 (34)")

 Ø Histamine fish poisoning (HFP) is a chemical intoxication")


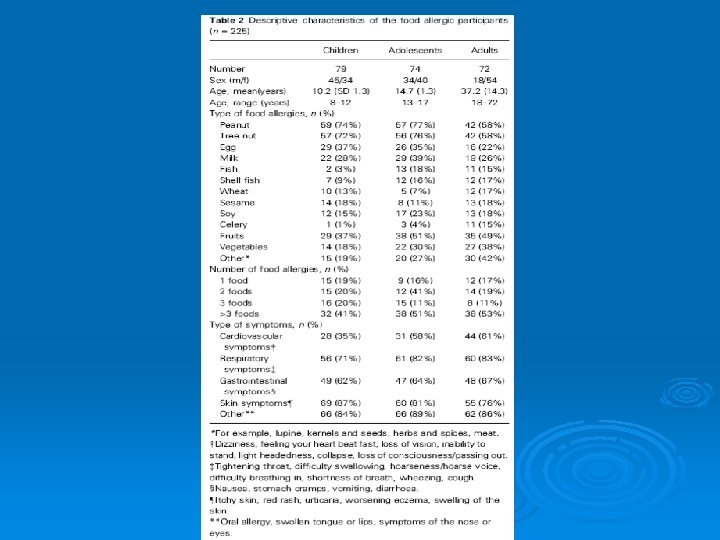
 Number of patients (%) Female Age (avg, range) European")





 Lack et al, NEJM 2003 348")







 not clinical allergy Used")





 Skin tests showed: weak positive (3 mm) wheat, RAST to wheat 2+,")
 is an effective treatment in")









 test where this")











- Slides: 77
Food allergy in adults: what’s new on the menu? Penny Fitzharris August 2010
Food allergy in adults Ø What is it? Ø What foods are involved? Ø Who is affected? Ø How, when and why does it develop? Ø How is it diagnosed and managed? Ø What treatment is available? Ø What problems are associated? Ø How do we improve services?
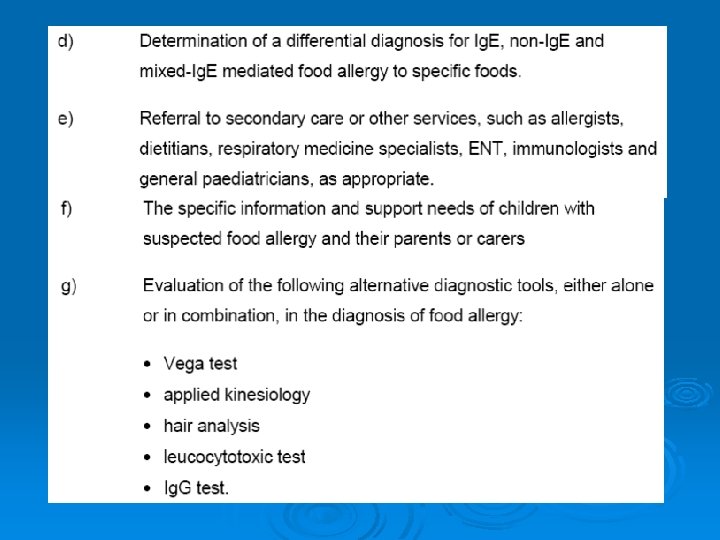
Food allergy is an immune-mediated adverse reaction to food – failure of immune tolerance Ø In developed countries food allergy present in 6 - 8 % of children, 2 - 3 % of adults Ø Immune mechanisms include: - Ig. E mediated e. g. anaphylaxis - non Ig. E mediated e. g. coeliac disease - reactions involving Ig. E and non-Ig. E e. g. eosinophilic oesophagitis
Ig. E mediated mast cell mediator release
Symptoms of Ig. E-mediated Food Allergy rapid onset (minutes, up to 2 hours) Ø multiple organ systems often involved Ø result from chemical mediators released from mast cells and basophils Ø manifestations include: - acute urticaria (hives), angioedema - throat tightness, stridor, chest tightness, wheezing, persistent cough, voice change, rhinitis, conjunctivitis - nausea, vomiting, abdominal pain, diarrhoea - alteration of consciousness, hypotension - anaphylaxis Ø
Food allergy in adults Ø What is it? Ø What foods are involved? Ø Who is affected? Ø How, when and why does it develop? Ø How is it diagnosed and managed? Ø What treatments are available? Ø What problems are associated? Ø How do we improve services?
Food allergens of plant origin - peanuts roasted > boiled or fried - soya - lentils, beans, peas, lupin Ø Cereal grains - wheat, barley, rye, oats, corn, rice Ø Legumes cross reactivity between cereal and grass pollens cereal allergens in bourbon, whisky Umbelliferae - celery, carrot, parsley, fennel, dill Ø Solanaceae - tomato, potato, peppers, aubergine, Ø coffee Tree nuts, seeds - hazel, almond, brazil, sesame Ø Fruits - increasingly common in Europe Ø
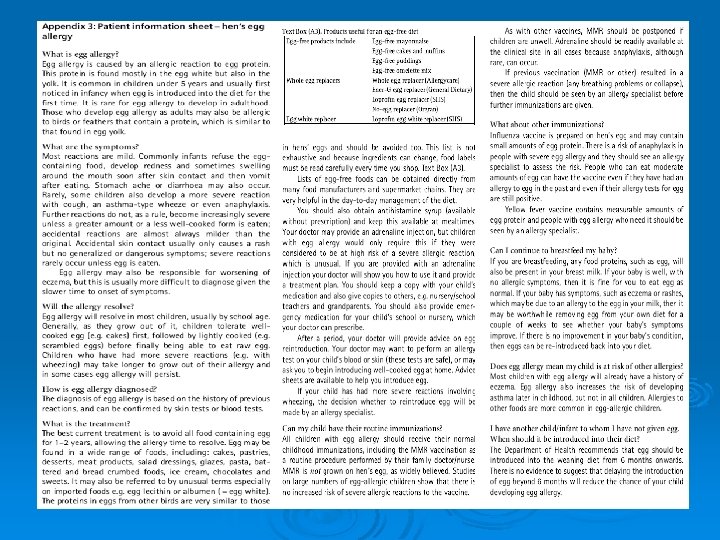
Allergens of animal origin Ø cow’s milk Ø hen’s egg - egg white > egg yolk but chicken allergy may - several allergens, heat labile and heat stable occur with yolk allergy (egg-bird syndrome) Ø fish Ø crustacea - cross reactions within crustacea family - cooking vapours may be a problem, not cross reactive with crustacea frequent Ø molluscs - true allergy not frequent - snails: cross reactivity with mite goat and sheep milk Ø meat e. g. pork, beef, chicken Ø
What makes a protein an allergen is still not known but… Ø Allergens have been mapped to only 5% of structural protein families: e. g. profilins from plants tropomyosins and caseins from animals pathogenesis related proteins from both Ø Biochemical functions of allergens are also limited and include enzymes, binding and storage proteins,
Prolamin family
Suspected precipitant for community onset anaphylaxis (Smith & Empson) 2000/2001 (129) Medication 44 (34) Antibiotic 18 (14) Β-lactam 14 (11) NSAID 11 (9) ACEI 5 (4) Food 40 (31) Shellfish / fish 21 (16) Peanut 7 (5) Treenut 2 (2) Other food 10 (8) Hymenoptera sting 10 (8) Honey bee 7/10 (5) Other* 2 (2) Unknown 32 (25) 2005/2006 (116) 27 (23) 9 (8) 7 (6) 11 (10) 5 (4) 32 (28) 15 (13) 4 (3) 3 (3) 10 (9) 7 (6) 4/7 (3) 2 (2) 48 (41) *This includes multiple possible precipitants, exercise etc
Allergy to fish/shellfish? Ø May develop in adult life. Ø Allergy to seafood (scaly fish, crustaceans and mollusks, including bivalves, cephalopods, gastropods) is more common where fish is commonly eaten. Ø Individuals may react only to scaly fish or crustaceans or mollusks, but some react to more than one group. Within each group there is often cross reactive allergy. Ø Other causes include…
Histamine fish poisoning (scombroid poisoning) Ø Histamine fish poisoning (HFP) is a chemical intoxication which occurs after eating fish of the dark meat varieties including tuna, kahawai, mackerel, bonito, butterfly kingfish, anchovies Ø Histamine is commonly the result of high temperature spoilage (>21°C), and often occurs if dead fish remain in set nets during warm sea temperatures, or improper or delayed refrigeration. Histamine is not destroyed by freezing, cooking, smoking, curing or canning. Ø Should be considered in a patient who regularly eats fish, without a previous reaction Ø
Anisakis: a nematode which infects marine animals
Food allergy in adults Ø What is it? Ø What foods are involved? Ø Who is affected? Ø How, when and why does it develop? Ø How is it diagnosed and managed? Ø What treatments are available? Ø What problems are associated? Ø How do we improve services?
Community-onset anaphylaxis (Smith & Empson) Number of patients (%) Female Age (avg, range) European NZ Maori Pacifika Asian Other Atopic disease Asthma Hx of allergic reaction Prev seen at allergy clinic Precipitant known Prev Anaphylaxis Had adrenaline autoinjector 2000/2001 77/129 (60) 40. 7 (15 -81) 81 (63) 8 (6) 13 (10) 14 (11) 13 (10) 60 (47) 44 (34) 68 (53) 8/68 (12) 47/68 (69) 55 (43) 6/55 (11) 2005/2006 73/116 (63) 43. 8 (15 -88) 71 (61) 5 (4) 16 (14) 17 (15) 7 (6) 34 (29) 29 (25) 59 (51) 15/59 (25) 43/59 (88) 40 (34) 10/40 (25)
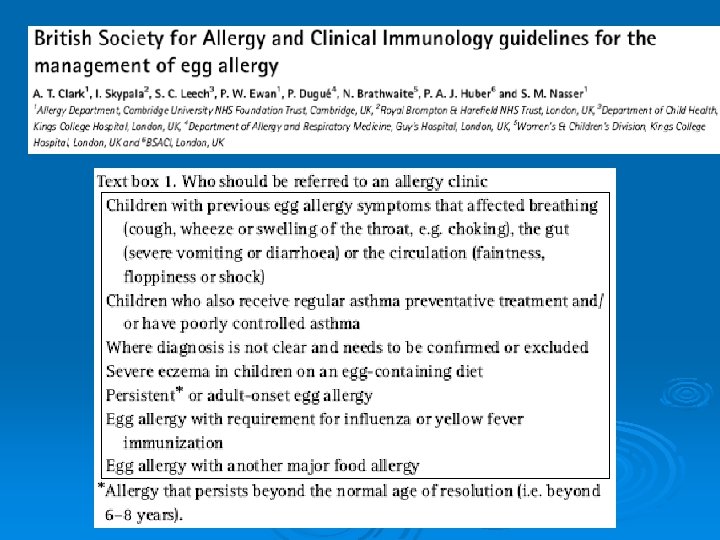
Food allergy in adults Ø What is it? Ø What foods are involved? Ø Who is affected? Ø How, when and why does it develop? Ø How is it diagnosed and managed? Ø Who should diagnose and manage? Ø What problems are associated? Ø How do we improve services?
Why has May become allergic to peanut? Ø Family history? Neither parents has atopic disease Ø As a first child she is at higher risk of allergy “Hygiene hypothesis” – microbial exposures Ø Infant diet? allergens and other nutrients Ø Weaning advice in the last decade? What aspects of route, timing, duration and extent of exposure may be relevant?
June 1998 COT recommended that “pregnant women who are atopic, or for whom the father or any sibling of the unborn child has an atopic disease, may wish to avoid eating peanuts and peanut products during pregnancy and lactation”. It was also recommended that these infants should avoid peanut and peanut products during weaning and until at least 3 years of age. In common with all children, exclusive breast feeding for 4 -6 months was recommended
Hourihane et al JACI 2007; 119: 1197202 Ø 1072 children born 1999 / 2000 (after COT advice) Ø 61% of mothers recalled hearing advice, unaffected by atopic status Ø Many mothers (42%) reduced peanut consumption Ø Few (3. 8%) avoided peanut entirely Ø Diet change more likely with first child and when child’s father was atopic
Ø 65% of the children had consumed peanut by age 4 -5 y Ø mean introduction of peanut was at 36 m Isle of Wight cohort born 1989/90 - 12. 6 m Ø 1. 8% had peanut allergy (challenge) 2. 8% were sensitised to peanut Ø children with peanut allergy had high likelihood of eczema history
Avon Longitudinal Study of Parents and Children (ALSPAC) Lack et al, NEJM 2003 348 977 -85 Ø Ø Ø Study children were history positive to age 38 m, studied at age 4 -6 y 23 of 29 with positive skin test had a positive DBPCFC (50 mg-8 g) (No responses to placebo) children with eczema were 4 times more likely to have peanut allergy if oozy, crusted eczema then 25 times more likely to have peanut allergy If had used creams containing peanut oil were 8 times more likely to have peanut allergy
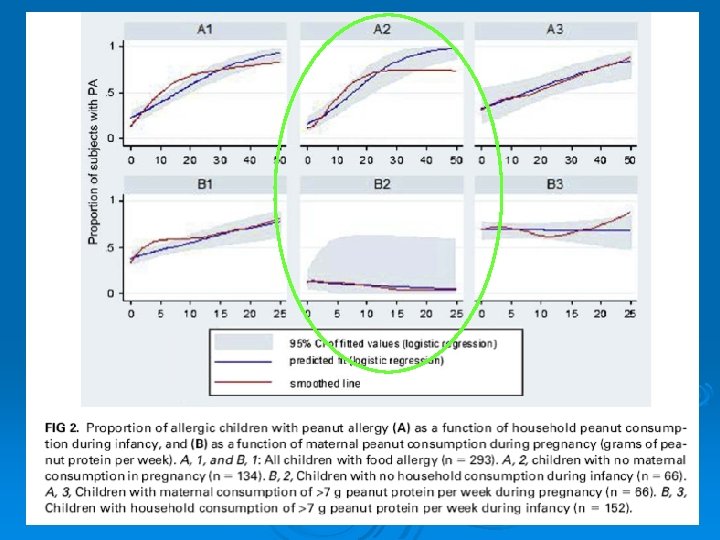
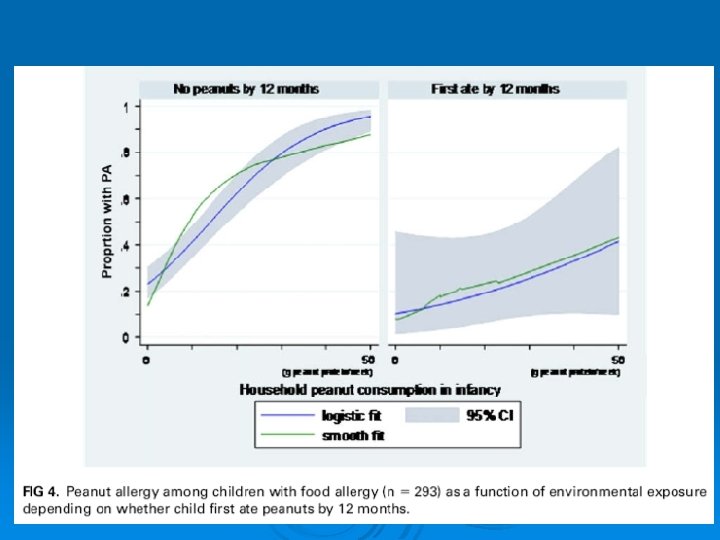
Household consumption as a risk factor for the development of peanut allergy - Fox AT JACI 2009; 123: 417 -23 Ø Study examined different routes of peanut exposure in the development of allergy Ø Questionnaires at time of allergy clinic attendance, usually with eczema. Known peanut allergy excluded. Routine investigations in clinic. Ø peanut allergy cases (133) high risk controls -egg allergy (160) low risk controls (150)
Fox AT JACI 2009; 123: 417 -23 Ø Eczema present in first year in 92% PA cases, 88% egg allergy cases, 42% low-risk controls Ø 90% breast fed (no group differences) Ø Median household peanut protein consumption: Household peanut protein consumption Low risk controls 6. 9 g/week High risk controls (egg allergic) 1. 9 g/week Peanut allergic cases 18. 6 g/week
Du Toit G et al, JACI 2008; 122: 984 -91 Ø Prevalence of peanut allergy: Jewish children in UK (5171) 1. 85% Jewish children in Israel (5615) 0. 17% (p<. 001) Ø Introduction of peanut by 9 months of age: 69% of Israelis v 10% of UK infants Ø Median monthly consumption in first year: 7. 1 g in Israel, 0 in UK
Du Toit G et al, JACI 2008; 122: 984 -91 Ø Introduction of egg, soya, wheat, vegetables, fruit and tree nuts was similar in both countries Ø Small differences in introduction of cow’s milk/dairy, breast feeding and exclusive breast feeding Ø Peanut protein and major peanut allergen content similar in commonly used products
COT Dec 2008 Ø “There is now limited human evidence, consistent with a larger body of animal data, suggesting that non-oral routes of exposure to peanut, such as the skin, may be relevant. ”
COT statement Dec 2008 Ø “The shift in the balance of evidence since 1998 is such that the Committee believes that the previous precautionary advice to avoid peanut consumption during pregnancy, breast feeding and infancy, where there is atopy or atopic disease in family members, is no longer appropriate. ” Ø Expert opinion in Europe, US and Australasia is similar
May Ø Is it possible to predict whether allergy will persist? whether she is at risk of a more severe reaction? can persisting allergy be treated?
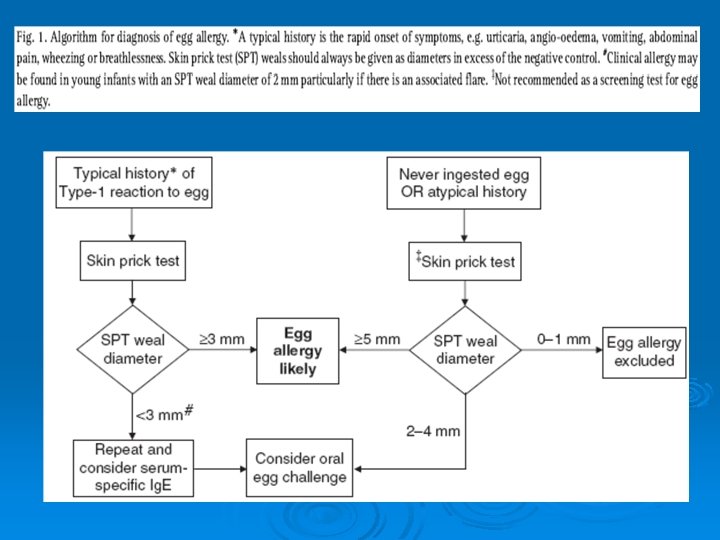
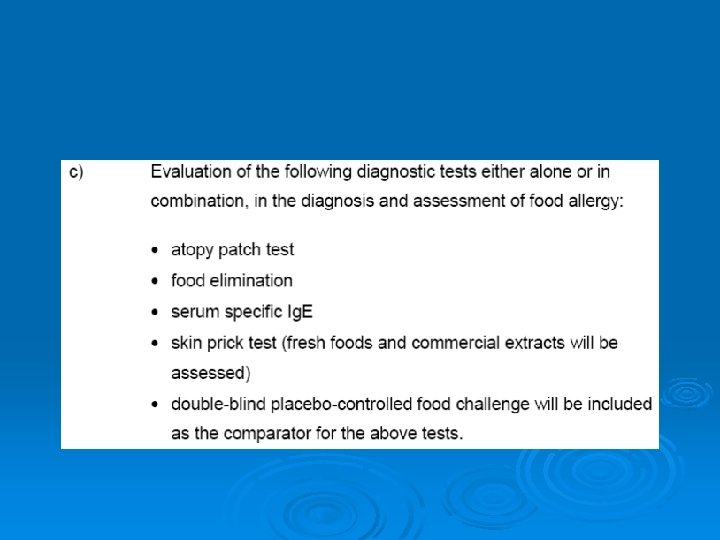
Skin prick tests – detect sensitisation (presence of Ig. E) not clinical allergy Used for inhalants, foods, venoms and some drugs Detect specific Ig. E bound to mast cells in the skin
Can skin tests predict clinical response? Ø 100% of children with wheals over a certain size reacted to food challenge (urticaria, severe eczema, asthma, rhinitis, vomiting, other g-I, anaphylaxis) Cow’s milk Egg Peanut 8 mm 7 mm 8 mm Ø Specificity of 100% Ø May’s skin test: Peanut 13 mm Sporik et al, Clin Exp Allergy, 1999 < 2 years <2 years < 2 years 6 mm 5 mm 4 mm
Measurement of specific Ig. E in the blood eg RAST HA Sampson 2004
Does further investigation of purified allergen component specificity help in prognosis? Ø Not yet- potential for the future. Peeters et al, Clin Exp Allergy 2007; 37: 108 -115
“Component resolved diagnosis” allergen specific diagnosis Gradual transition towards component resolved diagnosis seems inevitable. Many purified or recombinant allergens are now available for use in the Immuno. CAP RAST method. First available allergen at Lab+ is the wheat allergen r. Tri a 19 (omega-5 gliadin). Sensitisation to this allergen is associated with wheatdependent exercise induced anaphylaxis
Louise Ø 4 -6 episodes itching and urticaria in different circumstances since December 2007 Ø April 2008 - shopping at K-Mart after BK chicken fillet burger – collapse-adrenaline used at EM Ø September 2008 K-Mart, BK chicken fillet burger again and Nurofen. Collapse, Epipen used Ø Eats wheat, bread, chicken, many foods without problem
Louise (2) Skin tests showed: weak positive (3 mm) wheat, RAST to wheat 2+, 3 KU/L, wide range of other foods negative, negative to chicken Ø Clinical Impression: probably food-dependent exercise induced anaphylaxis advised to avoid wheat before exercise and NSAIDs before exercise Subsequently: Ø skin tested “fresh” BK burger and fries – negative Ø 2 further episodes anaphylaxis after eating small very amounts of wheat, followed by exercise (hospital treatment) Ø RAST to omega-5 gliadin peptide 4+, 13 KU/L Ø Subsequent exercise challenge (avoiding wheat) negative Ø
If allergy persists into older childhood? Ø Desensitisation (immunotherapy) is an effective treatment in Ig. E mediated allergy to insect venoms and inhalant allergens Ø Can it be used in Ig. E-mediated food allergy?
Successful oral tolerance induction in severe peanut allergy Clark AT et al, Allergy 2009 50 mg approx ¼ - 1/5 of a peanut 1 peanut approx 200 -240 mg protein 800 mg peanut protein=2. 5 mls smooth peanut butter
JACI 2009
Hofmann, 2009, JACI Safety aspects
Oral IT to foods Ø Large resource implications for paediatric and adult allergy services! Ø Not just peanut but many other foods Ø Safety concerns remain an issue Ø Will effects persist if oral intake is discontinued?
Food allergy in adults Ø What is it? Ø What foods are involved? Ø Who is affected? Ø How and When does it develop? Ø How is it diagnosed and managed? Ø What treatments are available? Ø What are the effects on quality of life? Ø How do we improve services?
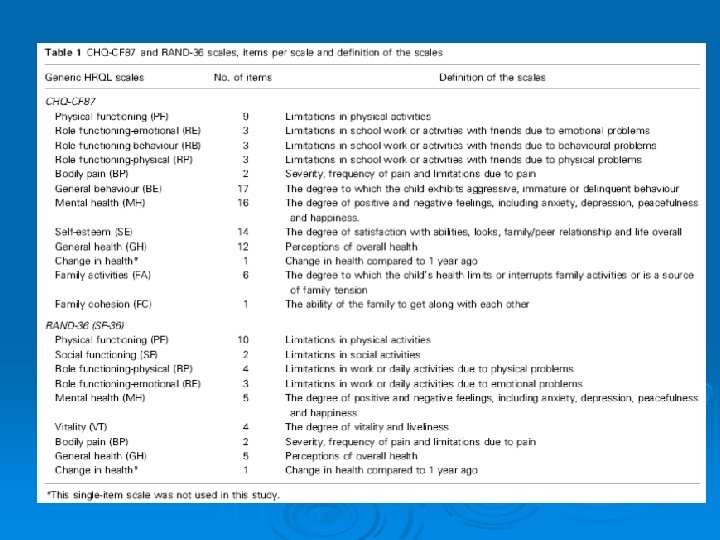
RB limitations due to behavioural problems BP severity/frequency of pain/limitations assoc GH perceptions of overall health
SF social functioning VT vitality and liveliness GH general health
SF social functioning RP physical problems BP pain GH general health
Food allergy in adults Ø What is it? Ø What foods are involved? Ø Who is affected? Ø How and When does it develop? Ø How is it diagnosed and managed? Ø What treatments are available? Ø What problems are associated? Ø How do we improve services?
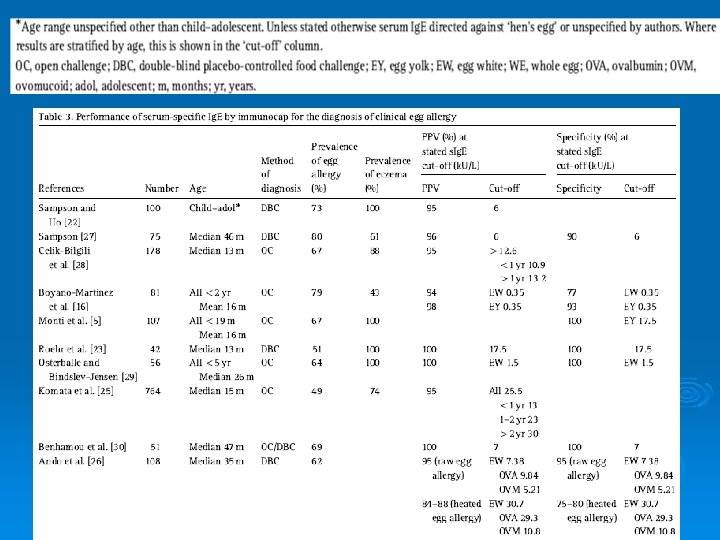
PPV – proportion of those identified as positive by the (skin) test where this is correct Specificity – proportion of those who don’t have the condition, correctly identified as negative
In summary Ø Ø Ø Ø Food allergy affects 1 -2% of the population Fish, shellfish, peanuts and nuts are the main offenders Food allergy is responsible for about 1/3 of anaphylaxis in Auckland Most (but not all) food allergy develops in childhood Food allergy strongly linked with early eczema Allergen entry through the skin may be important There is no evidence to advise maternal avoidance
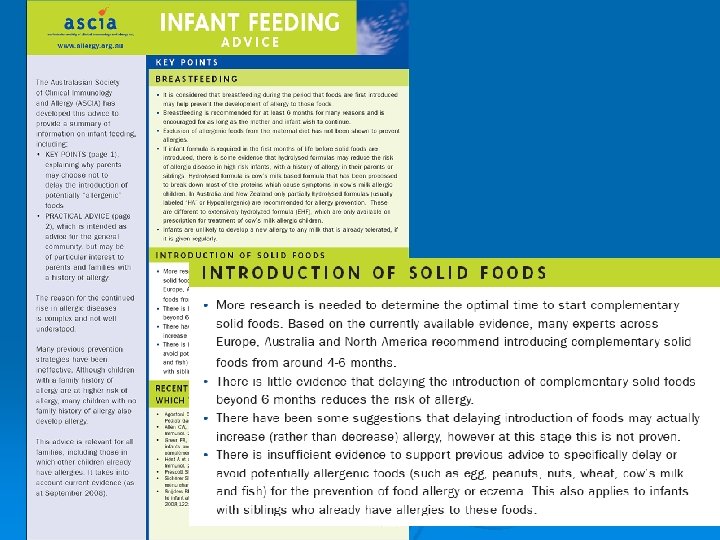
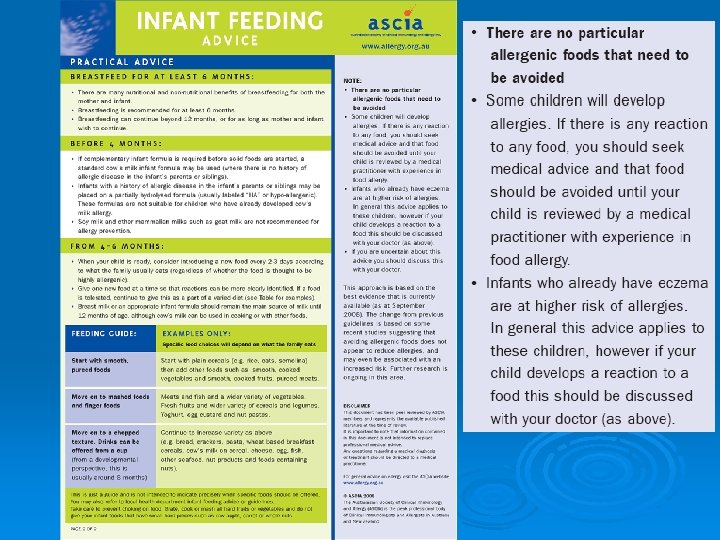
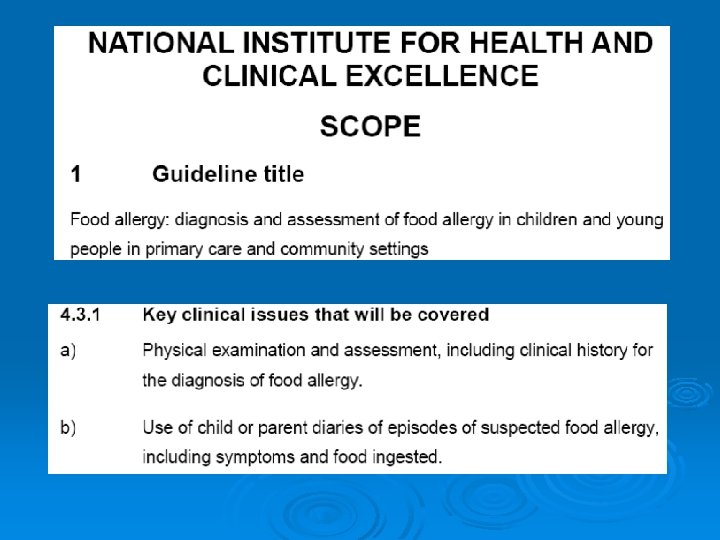
Ø Ø Ø There is no evidence to recommend maternal avoidance of allergens in pregnancy or breast feeding (unless allergy in mother or child) Early introduction of foods (not before 4 months) may help induce oral tolerance Oral desensitisation may become a useful treatment. More research needed. Quality of life affected in food allergy Several bodies are developing diagnosis and management guidelines which will be helpful. Still a complex area!
Lack et al, NEJM 2003 348 977 -85
Lack et al, NEJM 2003 348 977 -85
Component-resolved diagnosis from latex allergy by microarray Authors: Ebo, D. G. 1; Hagendorens, M. M. 2; De Knop, K. J. 1; Verweij, M. M. 1; Bridts, C. H. 1; De Clerck, L. S. 1; Stevens, W. J. 1 Source: Clinical & Experimental Allergy, Volume 40, Number 2, February 2010 , pp. 348 -358(11) Ø 26 healthy controls 22 latex allergic patients All showed specific Ig. E to Hev b 1, Hev b 3, Hev b 5 or Hev b 6. 02 Ø 20 latex sensitised but clinically non reactive None were sensitised to above allergens. >75% sensitised to Hev b 8 Ø
Tropomyosin family
Other candidates in the diet and geneenvironmental interactions? Ø Ø Ø Ø Folic acid – potential epigenetic regulation effects e. g. methylation influences IFNγ gene promoter, affecting TH 1 and Treg expression n-3 polyunsaturated fatty acids (fish oil) Prebiotics – oligosaccharides Probiotics – effects appear strain specific Vitamin D Antioxidants Role of breast milk TGFβ in inducing tolerance
Effects of oral IT with peanut Ø Reduced basophil activation Ø Initial rise then fall in specific Ig. E Ø Increase in specific Ig. G and Ig. G 4 Ø Changes in Fox. P 3+ T regulatory cells Ø Down-regulation of genes in apoptotic pathways
Prevalence of peanut allergy in three UK studies 1996 -2006 No of children Year of birth Age (y) when studied Prevalence of sensitisation peanut allergy (95% CI) Tariq et al 1996 981 1989 -90 4 -5 SPT 1. 1% (0. 5 -1. 6) 0. 5% (0. 1 -0. 8) Grundy et al 2002 1246 1994 -1995 3 -4 SPT, OFC 3. 3% (2. 3 -4. 3) 1% (0. 8 -2. 1) Hourihane et al 2007 1072 1999 -2000 4 -5 SPT, s. Ig. E, DBPCFC 2. 8% (1. 8 -3. 8) 1. 8% (1. 1 -2. 7) Hourihane et al JACI 2007; 119: 1197 -202
Increasing prevalence of allergy Hospital admissions data from 1990/91 to 2000/01 in England. Over 11 years total admissions for these disorders increased from 0. 02% - 0. 06%. (1960 to 6752 out of 49, 300 admissions in total). Gupta et al, BMJ 2003