Follicular lymphoma with blastoid transformation with concurrent MYC

Follicular lymphoma with blastoid transformation, with concurrent MYC and BCL-2 gene rearrangements (Double -Hit Lymphoma) Changlee S. Pang, M. D. Wake Forest School of Medicine, USA

Clinical History � 71 -year-old female � PMH: type 2 diabetes, hypertension, GERD, hypertriglyceridemia and left shoulder pain. � Left cervical lymphadenopathy of six weeks duration with B symptoms of fatigue, night sweats and 20 pounds weight loss over three months. � Lab: Hemoglobin 11. 8, WBC 8. 7, Platelets 292, LDH 315

PET CT Imaging � Extensive cervical, bilateral axillary, mediastinal, retroperitoneal, mesenteric and inguinal lymphadenopathy � Hepatosplenomegaly � Hypermetabolic lesions throughout the axial and appendicular skeleton consistent with bone involvement � Soft tissue mass in the right popliteal fossa � Bilateral pleural effusions
")
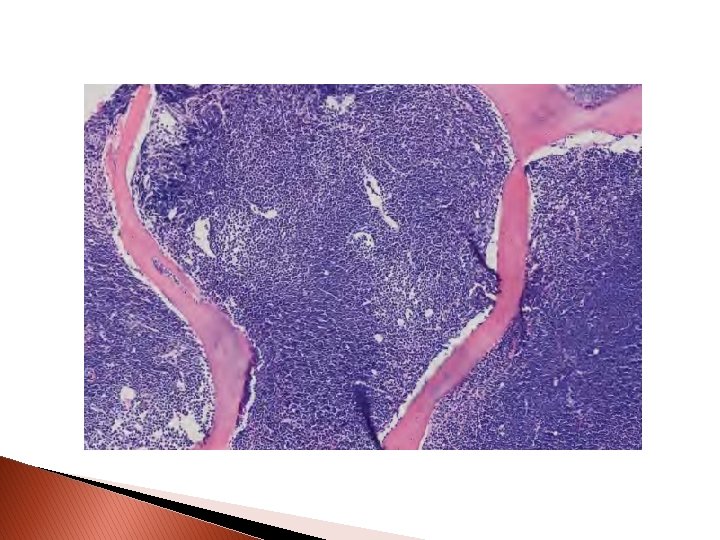
Salivary Gland (‘Lymph Node’)

CD 3 CD 20 BCL-2 CD 10

PAX 5 BCL-6 Ki 67

PAX 5 BCL-6 CD 10 BCL-2
: Follicular lymphoma, low-grade (grade 1 -2 of 3)")
Diagnosis � Salivary gland (“lymph node”): Follicular lymphoma, low-grade (grade 1 -2 of 3) positive for Ig. H (14 q 32)/BCL 2 (18 q 2); negative for MYC break-apart � FISH

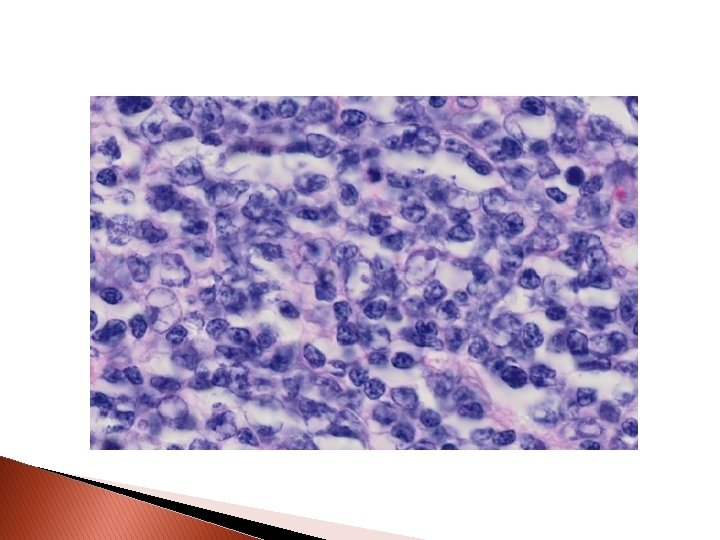
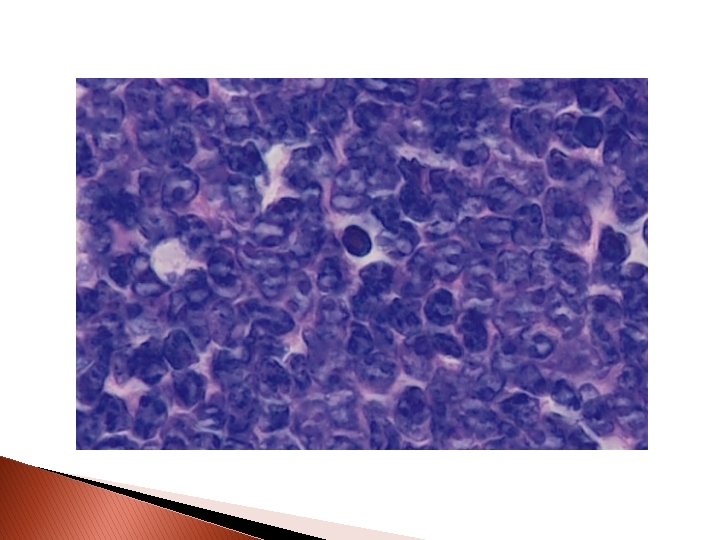
Bone Marrow Core Biopsy

CD 19 CD 10 CD 34 Td. T

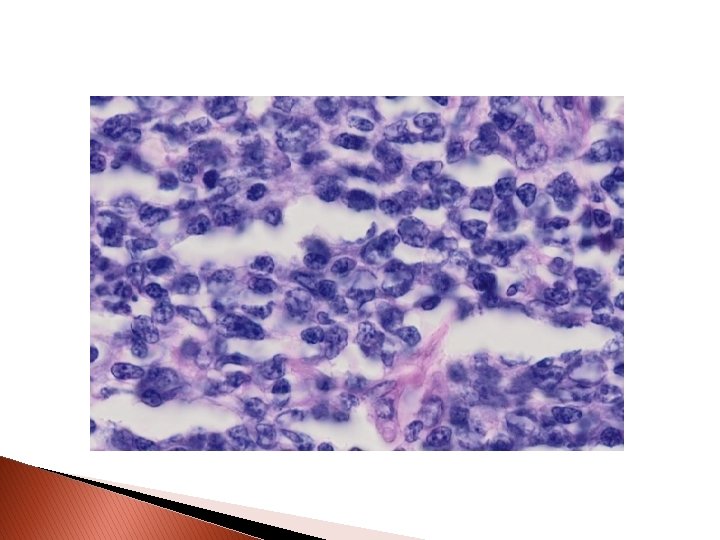
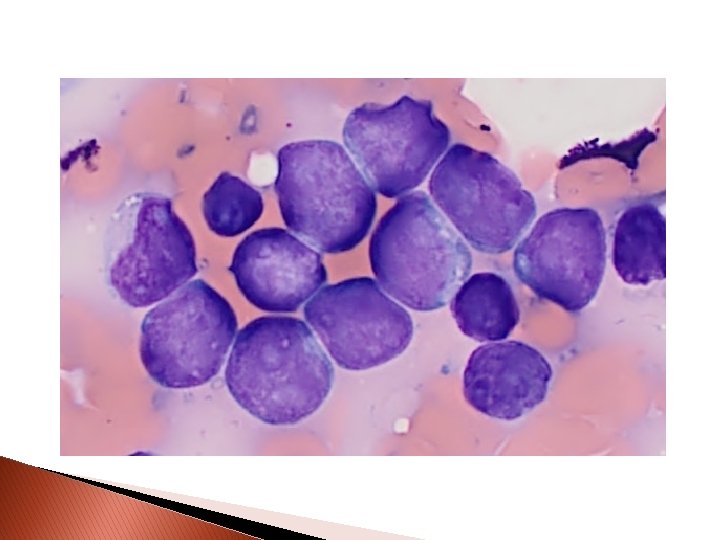
Bone Marrow Touch Prep

Peripheral Blood

Molecular analysis-FISH: Ig. H/BCL 2

Molecular analysis-FISH: c. MYC

Diagnosis � Bone Marrow and Peripheral Blood: Follicular lymphoma with blastoid transformation; Concurrent MYC and BLC-2 gene rearrangements (Double-Hit lymphoma).

Clinical Course � Patient received R-EPOCH x 4 cycles. � PET CT scan after two cycles showed significant interval response to therapy. � Significant complications after each cycle of R -EPOCH including mucositis, nausea, vomiting, dehydration, UTI, neutropenic fevers and sepsis. � Patient died five months after the initial diagnosis.
- Slides: 21