FNA of BREAST The 6 th ArabBritish School


FNA of BREAST The 6 th Arab-British School of Pathology Nina S Shabb, M. D. American University of Beirut Medical center, Beirut Lebanon

Objectives • Overview of breast FNA • AUBMC data 2003 -200 • CNB vs FNA of palpable and non palpable lesions

Status of breast FNA • • • 1930: Introduced 1980 -90: ↑ ↑ ↑ Late 90’s-now: ↓ Non palpable masses: Replaced CNB Palpable masses: CNB = FNA ? (institution dependent)

Reasons for ↓ popularity • Lack of experienced cytopathologists – – – ↑ Diagnostic errors ↑ Insufficient samples False positives False negatives Medico legal issues • Inability to distinguish In situ from invasive carcinoma

Trend of FNA of breast at AUBMC Total number: 1794

AUBMC data • All breast FNAs with corresponding surgical pathology material were reviewed over 5 years (Jan 2003 - Dec 2007) • FNA reports were categorized C 1 -C 5 • Palpable and non palpable masses were segregated • Data analyzed

Diagnostic categories • • • C 1: Unsatisfactory C 2: Benign lesion C 3: Atypical, probably benign C 4: Suspicious for malignancy C 5: Malignant The uniform approach to breast FNA. NCI recommendations

“Triple test” • FNA results • Clinical findings • Radiologic findings Combining these 3 tests improves false negative and false positive results

FNA/Pathology correlation, AUBMC, 2003 -2007 PATHOLOGY FNA Negative Positive Total C 1 4 5 9 C 2 56 1 57 C 3 9 0 9 C 4 0 13 13 C 5 1 92 93 Total 70 111 181 FN: 6. FP: 1. Unsatisfactory: 5%

Who should perform the FNA? • The person who is going to read it! (pathologist adequately trained) – Gleans information from gross findings and feel of the needle – Less unsatisfactory results (multiple passes as needed) – Less interpretative errors – Highest sensitivity and specificity









Complications of FNA • Very rare – Pain – Bleeding/hematoma: Pressure – Infection: Proper cleaning – Pneumothorax: Tangential aspirate – Vasovagal reaction: Legs up – Needle tract seeding? No

C 1 Unsatisfactory

FNA/Pathology correlation, AUBMC, 2003 -2007 PATHOLOGY FNA Negative Positive Total C 1 4 5 9 C 2 56 1 57 C 3 9 0 9 C 4 0 13 13 C 5 1 92 93 Total 70 111 181 C 1: 5%

C 1 palpable vs non palpable PATHOLOGY Total FNA non palpable Negative Positive Total 2 5 C 1 1 3 4 35 1 36 C 2 21 0 21 C 3 6 0 6 C 3 3 0 3 C 4 0 12 12 C 4 0 1 1 C 5 0 73 73 C 5 1 19 20 Total 44 88 132 Total 26 23 49 FNA Palpable Negative Positive C 1 3 C 2 C 1: 3. 5% (2. 3%pos) C 1: 8%
 • When FNA does not explain the mass • Lesions responsible")
C 1 (Unsatisfactory) • When FNA does not explain the mass • Lesions responsible for C 1 – Small – Fibrotic – Hypocellular benign and malignant • Operator dependent • Range in literature: 0. 7 -47% (5%) • CNB: advantage

C 1 • Management: More tissue

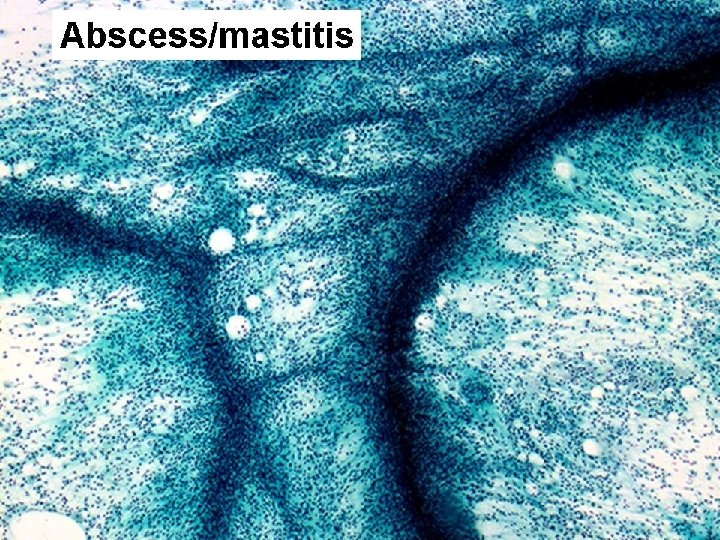
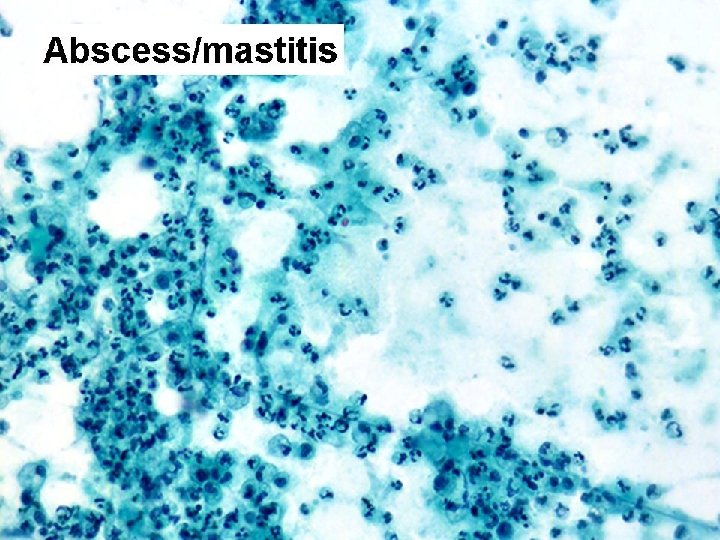
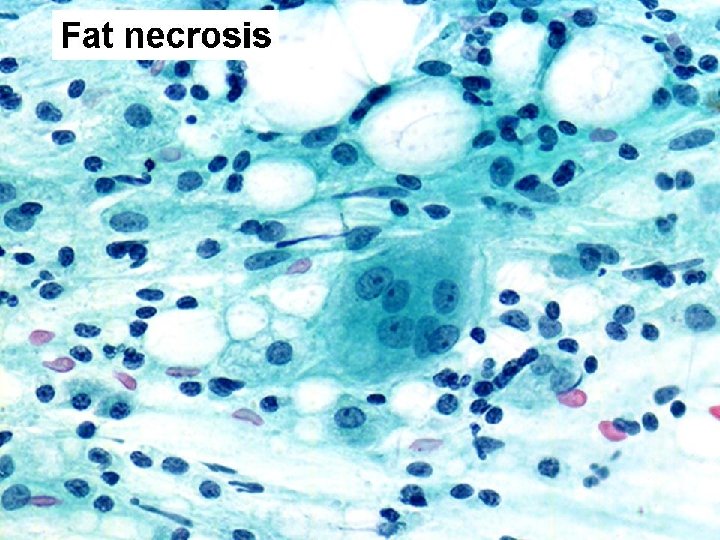
C 2 Benign

C 2 benign • FNA: Adequate and representative material of benign disease – FCC (cysts) – Abscess – Fat necrosis – Fibroadenoma – Other

FNA/Pathology correlation, AUBMC, 2003 -2007 PATHOLOGY FNA Negative Positive Total C 1 4 5 9 C 2 56 1 57 C 3 9 0 9 C 4 0 13 13 C 5 1 92 93 Total 70 111 181 FN: 1

FNA/pathology correlation of palpable masses FNA p PATHOLOGY Negative Positive FCC FA Other Total neg IDC ILC DCIS Other Total pos Total C 1 2 1 0 3 2 0 0 0 2 5 C 2 16 18 1 PT 35 0 0 1 crib pap 0 1 36 C 3 4 2 0 6 0 0 0 6 C 4 0 0 7 2 2 1 tubular 12 12 C 5 0 0 69 3 (2 Pleo) 1 comedo 0 73 73 Total 22 21 1 44 78 5 4 1 88 132 44 88

FNA/pathology correlation of non palpable masses PATHOLOGY FA Other Total neg IDC ILC DCIS Other Total pos Total C 1 0 1 2 0 1 0 3 4 C 2 15 5 1 LN 21 0 0 0 21 C 3 1 2 0 3 0 0 0 3 C 4 0 0 1 0 0 0 1 1 C 5 0 0 1 (ame) 1 16 1 2 0 19 20 Total 16 8 2 26 19 1 3 0 23 49 Positive FCC 26 FNA n p Negative 23
 • 1 False negative: (1%) DCIS Cribriform and micropapillary. Misinterpreted on")
C 2 (benign) • 1 False negative: (1%) DCIS Cribriform and micropapillary. Misinterpreted on FNA as FCC

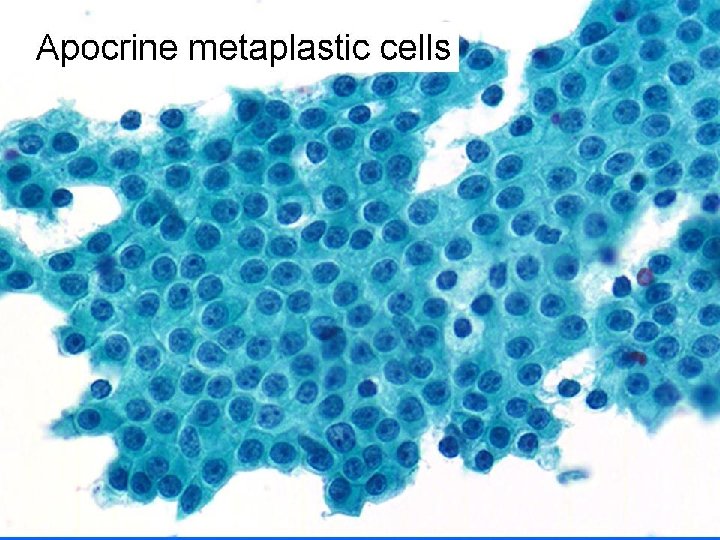
FCC • Cyst content: Clear, few macrophages • Hypocellular – Benign duct epithelial cells – Naked nuclei – Apocrine metaplastic cells
 – Very cellular –")
Fibroadenoma • Pigeon egg, rubbery feel • Smears (pattern recognition) – Very cellular – 3 components • Staghorn epithelial cohesive honeycombed duct cells • Stromal fragments • Numerous myoepithelial cells (naked bipolar nuclei)
 • Negative triplet: Follow up – FNA: Benign – Clinical: Benign")
C 2 (Benign) • Negative triplet: Follow up – FNA: Benign – Clinical: Benign – Radiologic: Benign

C 5 Malignant

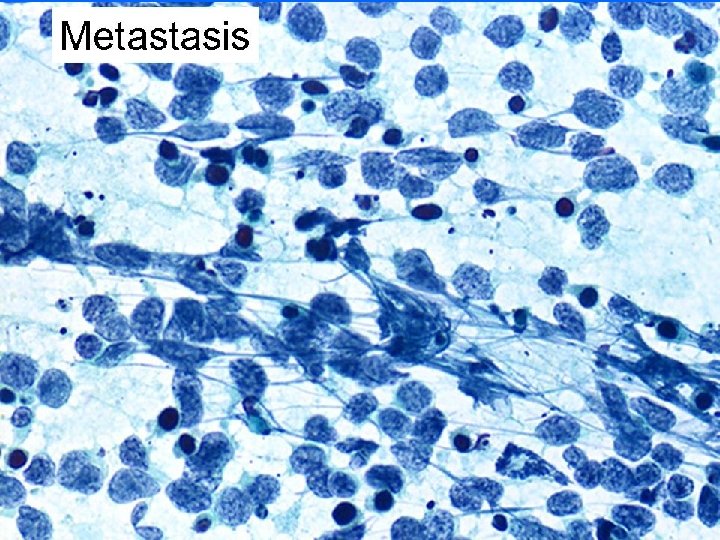
C 5 Malignant • Primary – – – IDC nos ILC Mucinous Tubular Papillary Other • Metastatic • Hematopoetic

FNA/Pathology correlation, AUBMC, 2003 -2007 PATHOLOGY FNA Negative Positive Total C 1 4 5 9 C 2 56 1 57 C 3 9 0 9 C 4 0 13 13 C 5 1 92 93 Total 70 111 181 False positive: Adenomyoepithelioma

FNA/pathology correlation of palpable masses FNA p PATHOLOGY Negative Positive FCC FA Other Total neg IDC ILC DCIS Other Total pos Total C 1 2 1 0 3 2 0 0 0 2 5 C 2 16 18 1 PT 35 0 0 1 crib pap 0 1 36 C 3 4 2 0 6 0 0 0 6 C 4 0 0 7 2 2 1 tubular 12 12 C 5 0 0 69 3 (2 Pleo) 1 comedo 0 73 73 Total 22 21 1 44 78 5 4 1 88 132 44 88

FNA/pathology correlation of non palpable masses PATHOLOGY FA Other Total neg IDC ILC DCIS Other Total pos Total C 1 0 1 2 0 1 0 3 4 C 2 15 5 1 LN 21 0 0 0 21 C 3 1 2 0 3 0 0 0 3 C 4 0 0 1 0 0 0 1 1 C 5 0 0 1 (ame) 1 16 1 2 0 19 20 Total 16 8 2 26 19 1 3 0 23 49 Positive FCC 26 FNA n p Negative 23

Adenomyoepithelioma • Rare benign tumor, epithelial and ME cells • FNA. – Scant. Scattered highly atypical epithelial cells. – Numerous foamy ME cells (histiocytes) • CNB: Interpreted as IDC, Grade 2/3 • Single false positive FNA since we started doing FNAs of breast (>3000 cases) • AME has been reported as a cause of false + in literature

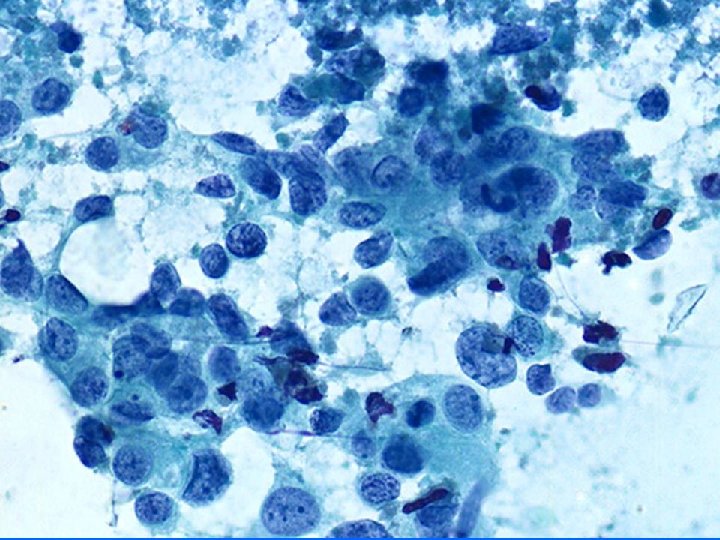
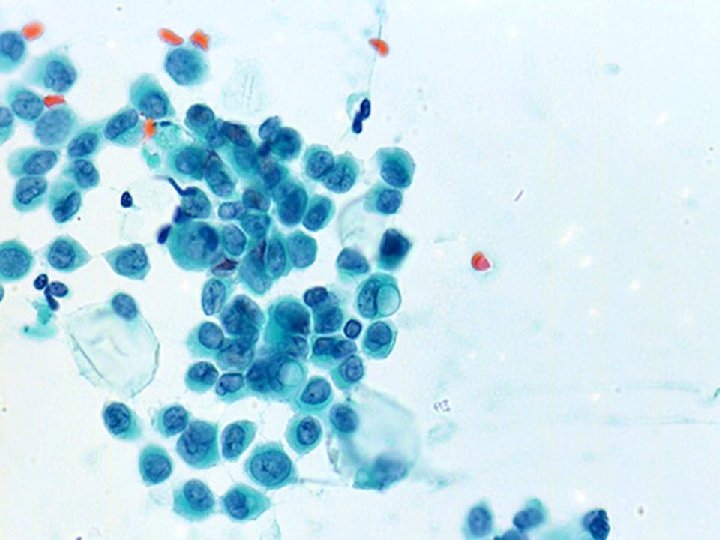
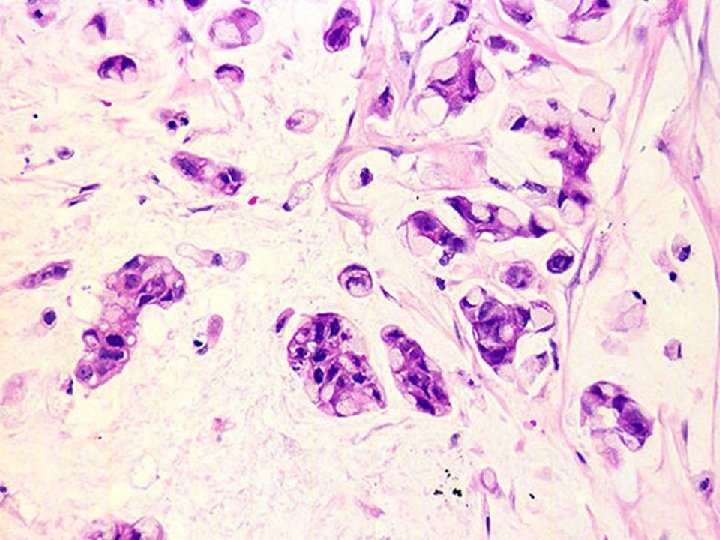
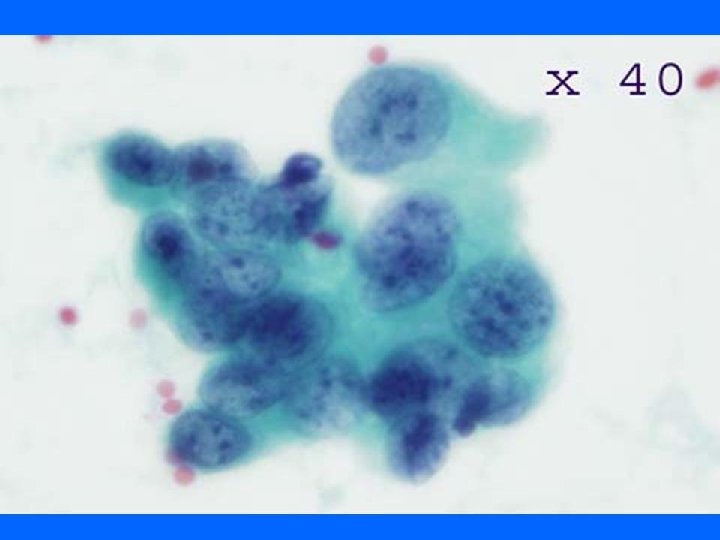
Diagnostic criteria for malignancy 1. Tumor cellularity 2. Discohesion 3. Cytologic features of malignancy. • Compare neoplastic cells to benign duct cells • • ↑ N/C ratio Irregular nuclear contour Hyperchromasia Presence of nucleoli

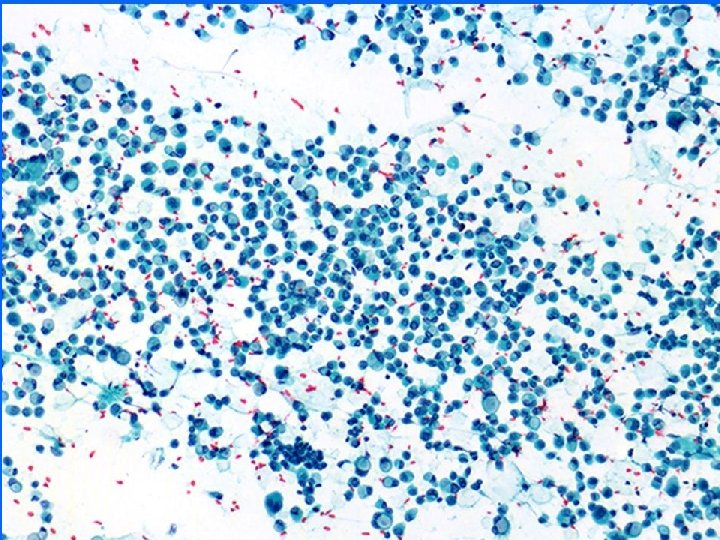
Ductal adenocarcinoma nos • • Cellular Necrotic background Monomorphic cell population Loss of cell cohesion Numerous isolated singe cells Anisonucleosis Lack of ME cells
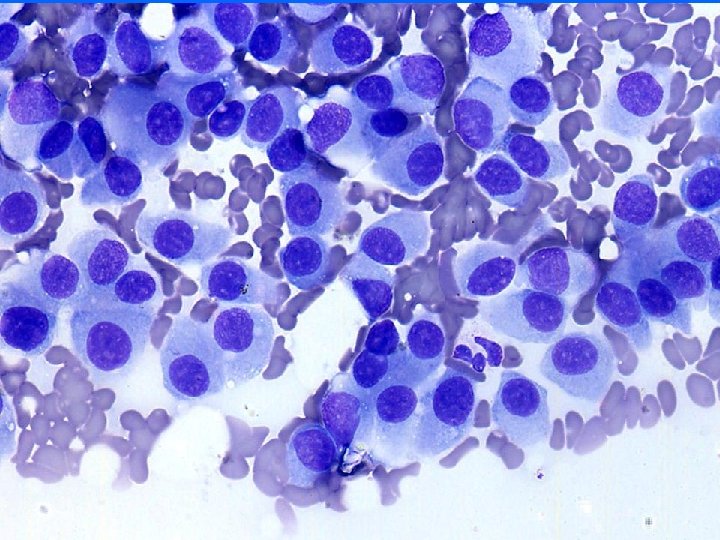

Tumor grade • HISTOLOGY – Glands – Nuclei – Mitosis • CYTOLOGY – Nuclei • • Size Membrane Chromatin Nucleoli Nuclear grade 1 -3 Good correlation with histologic grade

Special type carcinomas

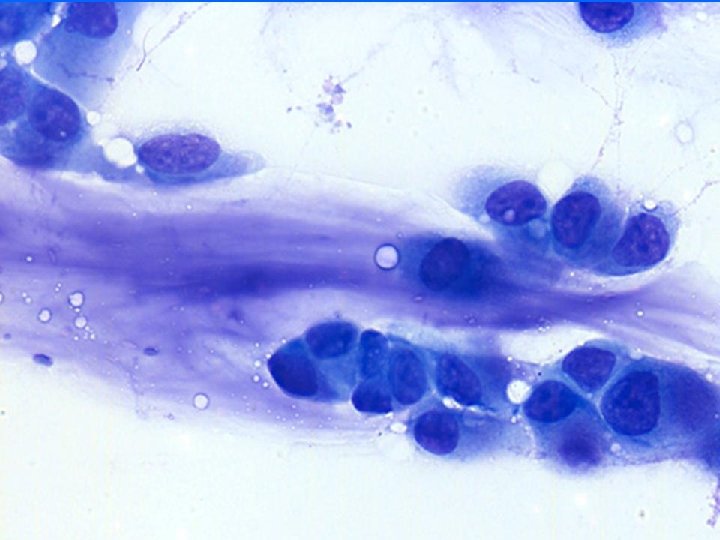
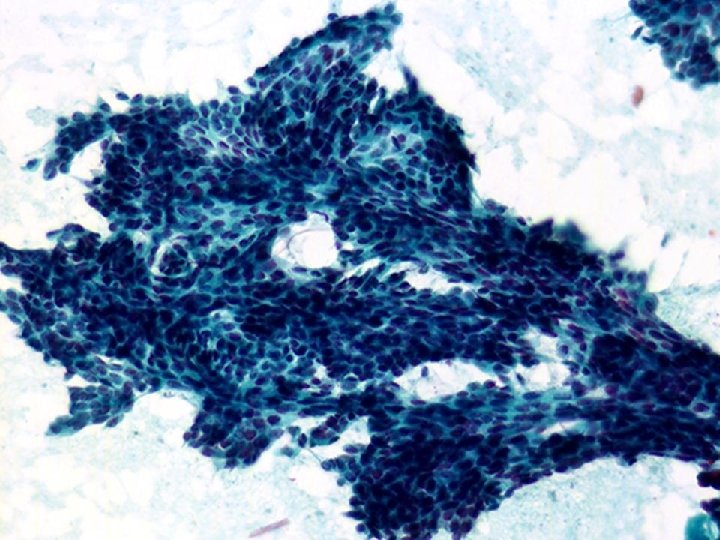
Lobular carcinoma • • Low to moderate cellularity Small chains or groups of cells, single cells Uniform population, small to medium sized cells Mild atypia, inconspicuous nucleoli Occasional signet ring cells Source of false negative Feel of the needle in the mass while doing FNA is most helpful
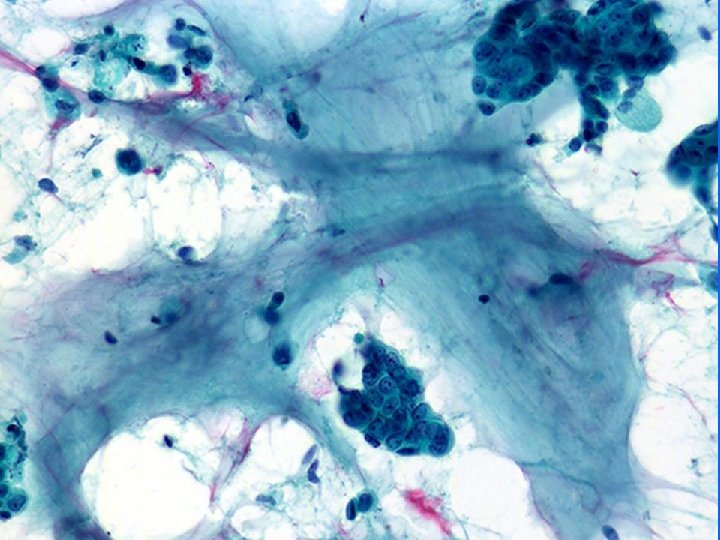

Mucinous carcinoma • • Well circumscribed, soft Thick mucinous material Cell balls, minimal atypia, few signet rings Cannot diagnose absolutely on FNA

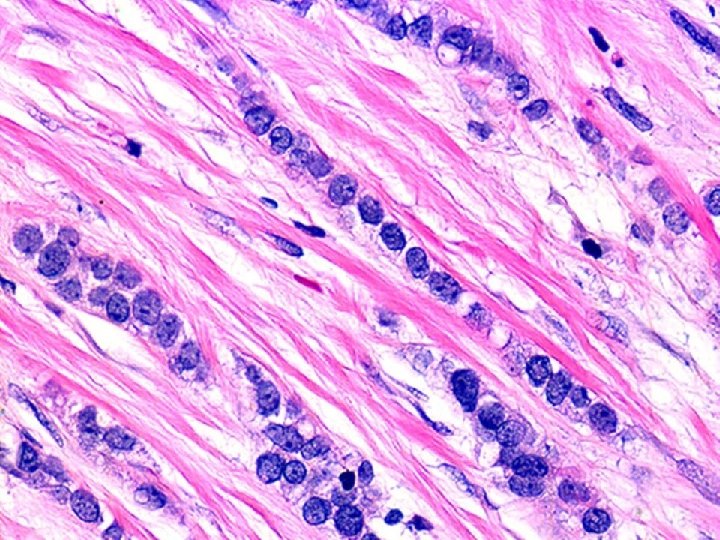
Tubular ca • Angular, rigid, bent tubular clusters, sharp borders • Crowded nuclei • Minimal tumor discohesion • Dispersed single cells, minimal atypia • Absence/paucity of ME cells • Peripheral perpendicular cells

Other carcinomas • Not very good • No clinical need • Carcinoma and nuclear grade

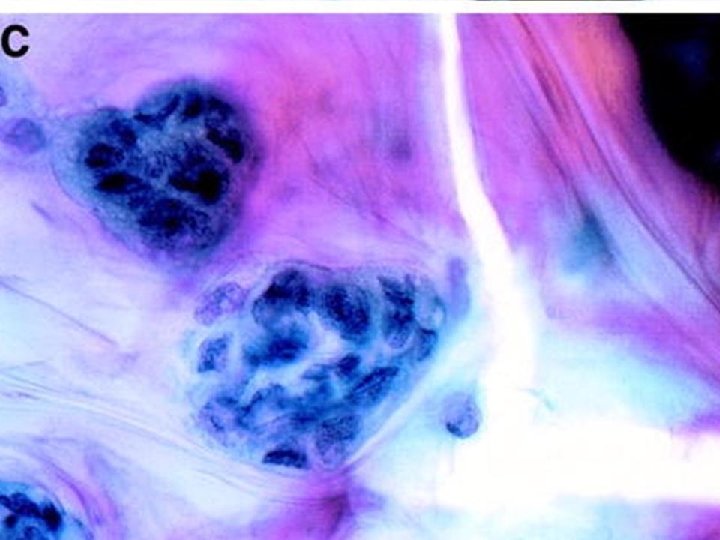
DCIS • FNA cannot distinguish in situ from invasive carcinoma – Cancer cells infiltrating fibrofatty tissue, tubular structures, cytoplasmic lumina, absence of ME cells) • Incidence of DCIS in FNA material ranges 1 -18% (palpable vs non palpable) • CNB is more accurate but not infallible (false negative 19 -66% )
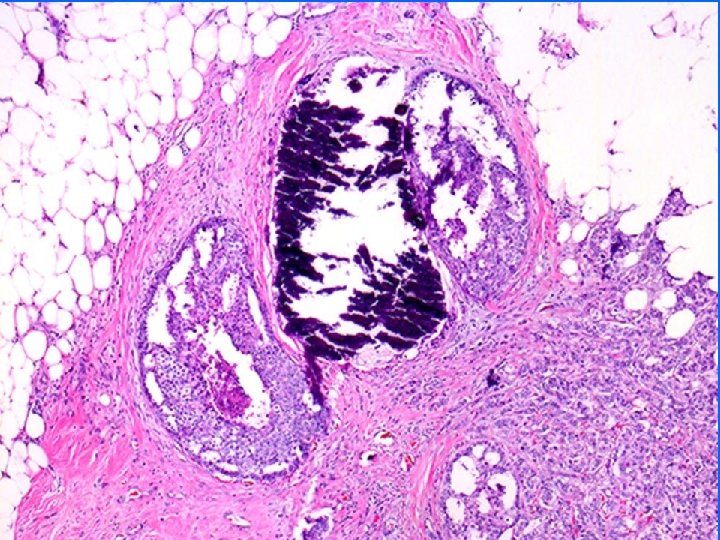

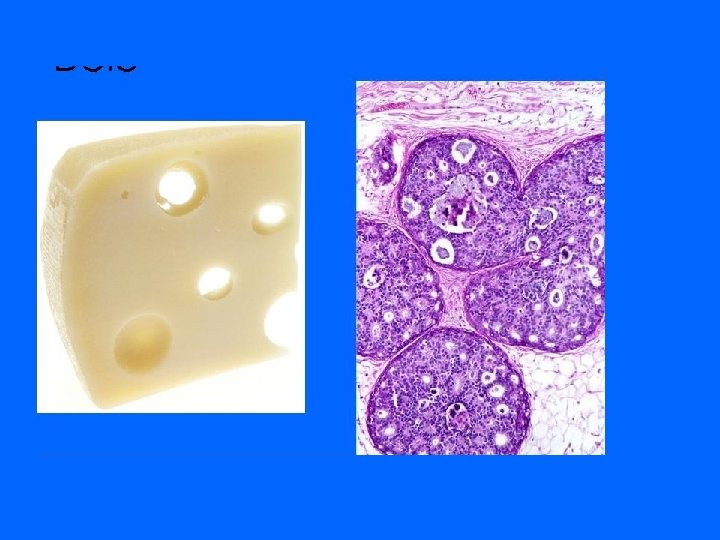
FNA of DCIS • DCIS Grade 3: – Pleomorphic carcinoma cells, calcium, necrosis, macrophages – casting Calcification on mammogram • DCIS cribriform – Low grade carcinoma – punched out holes in cell clusters • DCIS grades 1 and 2: – No distinguishing features

C 5 • Management • If the TT is positive then definitive treatment is undertaken

C 3 & C 4 C 3: Atypical favor benign C 4: Suspicious for malignancy
 • Atypical/indeterminate/favor benign • Lesion is probably benign •")
C 3 (atypical favor benign) • Atypical/indeterminate/favor benign • Lesion is probably benign • Malignancy cannot be excluded entirely • TT
 • Very high probability of malignancy but confirmation is")
C 4 (Suspicious probably malignant) • Very high probability of malignancy but confirmation is needed prior to definitive therapy • Others are complex lesions • Additional material

FNA/Pathology correlation, AUBMC, 2003 -2007 PATHOLOGY FNA Negative Positive Total C 1 4 5 9 C 2 56 1 57 C 3 9 0 9 C 4 0 13 13 C 5 1 92 93 Total 70 111 181 C 3+C 4: 11. 6%

FNA/pathology correlation of palpable masses FNA p PATHOLOGY Negative Positive FCC FA Other Total neg IDC ILC DCIS Other Total pos Total C 1 2 1 0 3 2 0 0 0 2 5 C 2 16 18 1 PT 35 0 0 1 crib pap 0 1 36 C 3 4 2 0 6 0 0 0 6 C 4 0 0 7 2 2 1 tubular 12 12 C 5 0 0 69 3 (2 Pleo) 1 comedo 0 73 73 Total 22 21 1 44 78 5 4 1 88 132 44 88

FNA/pathology correlation of non palpable masses PATHOLOGY FA Other Total neg IDC ILC DCIS Other Total pos Total C 1 0 1 2 0 1 0 3 4 C 2 15 5 1 LN 21 0 0 0 21 C 3 1 2 0 3 0 0 0 3 C 4 0 0 1 0 0 0 1 1 C 5 0 0 1 (ame) 1 16 1 2 0 19 20 Total 16 8 2 26 19 1 3 0 23 49 Positive FCC 26 FNA n p Negative 23

C 3 and C 4 lesions • Nature of lesion – – – Proliferative breast disease with atypia Low grade carcinoma (in–situ & invasive) Tubular ca Papillary lesions Phyllodes tumor • Technical reasons – Limited cellularity – Poor preservation of cellular features

C 3 and C 4 • Number of dx in this category shouldn’t exceed 12% (11. 6%) • C 3 in literature: 28 -52% Malignant (0%) • C 4 in literature: 81 -97% malignant (100%)

Inconclusive FNAs of breast with adequate and representative material: A cytologic/histologic study of 18 cases. AUBMC experience N Shabb F Boulous Z Chakhachiro

Inconclusive/erroneous cellular and representative FNAs/histology Patient Age Clinical presentation FNA performed by Dx 1 Cytologic cancer category Dx 2 Cytologic cancer category Final diagnosis 1 58 Hypoechoic mass Radiologist C 5 C 4 Adenomyoepithelioma 2 43 6. 5 cm lump Clinician C 3 -4 C 4 DCIS (crib) 3 67 lump Pathologist C 2 C 3 DCIS (crib, pap) 4 65 lump Clinician C 4 C 5 Inv crib 5 40 lump Pathologist C 4 Inv crib 6 46 4 mm U/S Radiologist C 4 Tubular 7 53 3 cm, gritty Pathologist C 3 -4 Tubular 8 43 f NA Clinician C 2 C 4 Tubular 9 44 f lump Clinician C 4 C 5 Lobular 10 71 f lump Clinician C 4 C 3 -4 Inv adeno (nos) 1/3 11 50 f NA Clinician C 4 Inv adeno (nos) 1/3 12 38 f lump, preg Pathologist C 4 C 5 Inv adeno (nos) 2/3 13 36 f 1 cm Pathologist C 4 C 5 Inv adeno (nos) 2/3 14 50 f Non palpable Radiologist C 4 C 5 Inv adeno (nos) 2/3 15 73 f 3 cm Pathologist C 4 Inv adeno (nos) 2/3 16 66 f 15 cm hem cyst Clinician C 4 ICPC 17 29 f lump Radiologist C 3 -4 FA 18 60 f 2 cm gritty Pathologist C 4 PT malignant

Papillary lesions • FNA not reliable in distinguishing benign from malignant. Defer to histology


False negative FNAs • Lesions responsible for false – – Low grade ca/lobular/mucinous/tubular/DCIS – Scirrhous tumors – Hemorrhagic/cystic – Small size • Usually sampling error (5/6) • Can be interpretative error (1/6) • TT

False positive FNAs • Lesions responsible for False + – – – Fibroadenomas Epithelial hyperplasia Pregnancy Papillary lesions Reactive atypias Adenomyoepithelioma • Usually interpretative errors • Poor specimen preparation • TT

Post triple test recommendations • Benign triplets – FU • Malignant triplets – Definitive therapy • Mixed triplets – Histologic evaluation

Benefits of the triple test • False negatives: ↓ 10 to 1% • False positives: ↓ 1 to < 0. 2%

FNA diagnostic accuracy • Literature – – Sensitivity: 75 -98% Specificity: 60 -100% False positive: 0 -2. 5% False negative: 2. 517% – Insufficient: 4 -13% (P), 36% (NP) • AUBMC – – Sensitivity: 94. 6% Specificity: 98. 6% False positive: *1% False negative: 1% – Insufficient: 3. 5% (P), 8% (NP)

CNB vs FNA preoperative evaluation of breast masses CNB FNA Special expertise (Performing + interpretation) No Yes Feel effect No Yes Safety (chest wall) No Yes Time consuming (pathologist) No Yes In situ/invasive +/- - Definitive dx Better Good Cost/TAT/pain/invasiveness Good Better Tumor grade Better Good Yes No Insufficient rate Better ↓ experience False +/- Better Inevitable Palpable Good Non palpable Good No Good Prognistic markers

Current issues with FNA of breast • False negative FNAs – High rate in inexperienced hands – Adeverse effect on patient. Delay in proper management – Medico legal problems (10% of MLP in US) • In situ vs invasive – Preoperative chemotherapy – LN dissection (small lesions)

Conclusions • Compared to CNB, FNA may not provide all the necessary information in modern management of some cases of breast ca. – Small lesions to determine management of the axilla – Some larger lesions where preoperative chemotherapy is a consideration.

Conclusions • CNB has replaced FNA in non palpable mammographically detected lesions • FNA is highly reliable in palpable masses particularly in the hands of properly trained aspirators and interpreters • FNA needs to be incorporated in the TT

")
Advantages of FNA • • • Easy “painless” office procedure Quick (dx in minutes) Inexpensive Decreases hospital costs Helps patient plan treatment in case of carcinoma • Helps alleviate anxiety in benign disease

Advantages of FNA • Definitive dx in inoperable ca, chest wall recurrence and LN metastases • Useful in pregnant patients • Diagnostic and therapeutic in benign cysts • Helpful in triaging patients for surgery • Decreases time in OR (eliminates need for FS)

Disadvantages of FNA • False negatives • False positives • Special training needed to perform and interpret FNA • In situ vs invasive carcinoma • Complications

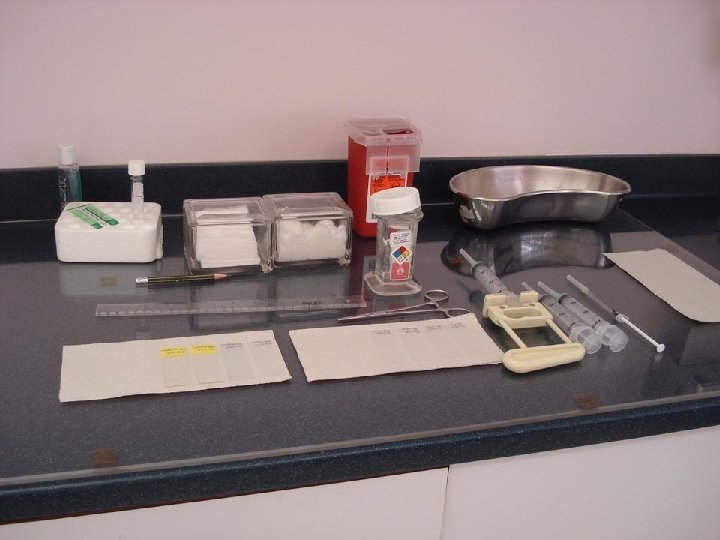
FNA technique • Ljung BM: Techniques of aspiration and smear preparation • Ljung BM: Thin needle aspiration biopsy video. Dept of Pathology UC San Francisco Ca • Koss LG et al: Aspiration biopsy: Cytologic interpretation and Histologic Basis, 2 nd ed, NY Igaku-Shoin, 1992.
 Quick transfer of material on")
FNA technique • • Quick aspiration (avoid blood clot) Quick transfer of material on slides Proper smearing (avoid crush) Immediate fixation (avoid air dry) – Papanicoulau stain (fully frosted alcohol fixed) – Romanowsky type stain (frosted tip, air dry) – Cell block (Optional)
")
Pointers while performing FNA • Clinical setting (age, skin and nipple changes, axillary LN) • Gross feel of tumor • Size of tumor. How to direct needle • FNA feel: Gritty or rubbery? • How many passes? • Rapid stain after every pass? • Naked eye inspection of cellularity

FNA/pathology correlation of palpable masses PATHOLOGY Negative Positive FNA p FCC FA Other Total neg IDC ILC DCIS Other Total pos Total C 1 2 1 0 3 2 0 0 0 2 5 C 2 16 18 1 PT 35 0 0 1 crib pap 0 1 36 C 3 4 2 0 6 0 0 0 6 C 4 0 0 7 2 2 1 tubular 12 12 C 5 0 0 69 3 (2 Pleo) 1 comedo 0 73 73 Total 22 21 1 44 78 5 4 1 88 132 44 88 Sensitivity: TP/TP+FN = 88/88+1 = 98. 8% Specificity: TN/TN+FP = 44/44+0 = 100% False negative: 1 False positive: 0

FNA/pathology correlation of non palpable masses PATHOLOGY Negative Positive FNA np FCC FA Other Total neg IDC ILC DCIS Other Total pos Total C 1 0 1 2 0 1 0 3 4 C 2 15 5 1 LN 21 0 0 0 21 C 3 1 2 0 3 0 0 0 3 C 4 0 0 1 0 0 0 1 1 C 5 0 0 1 (ame) 1 16 1 2 0 19 20 Total 16 8 2 26 19 1 3 0 23 49 26 23 Sensitivity: TP/TP+FN = 23/23+0 +100% Specificity: TN/TN+FP = 26/26+1 =96% False negative: 0 False positive: 1
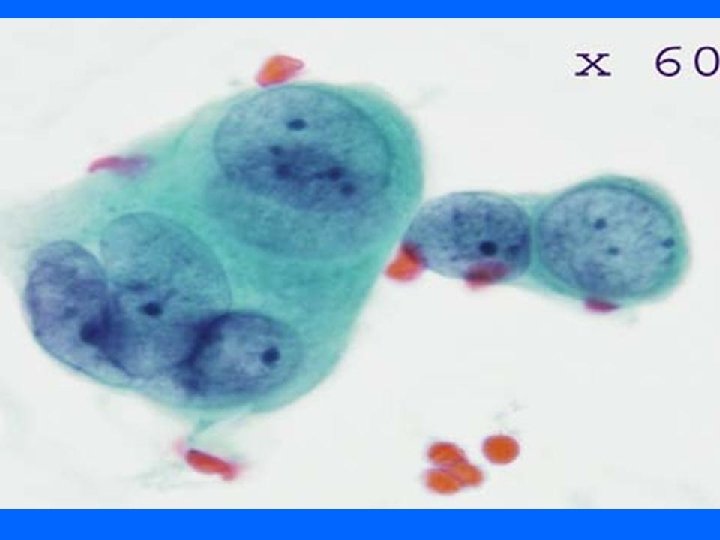
 • Apocrine metaplasia and")
Pitfalls • Low grade carcinomas (lobular, tubular, low grade ductal) • Apocrine metaplasia and lactational change Have large nuclei and prominent nucleoli
. • Placement of")
Breast FNA report • Precise location (laterality, O’clock, distance from nipple). • Placement of cytologic specimen in one of 5 categories (C 1 -C 5) • Specimen type • Localization technique • Comment of specimen findings • Adequacy • Recommendation of correlation with clinical and radiologic findings

Acknowledgments • • Dr Fuad Boulous Dr Zaher Chakhachiro Dr Alexis Bousamra Ms. Nisrine Hashem

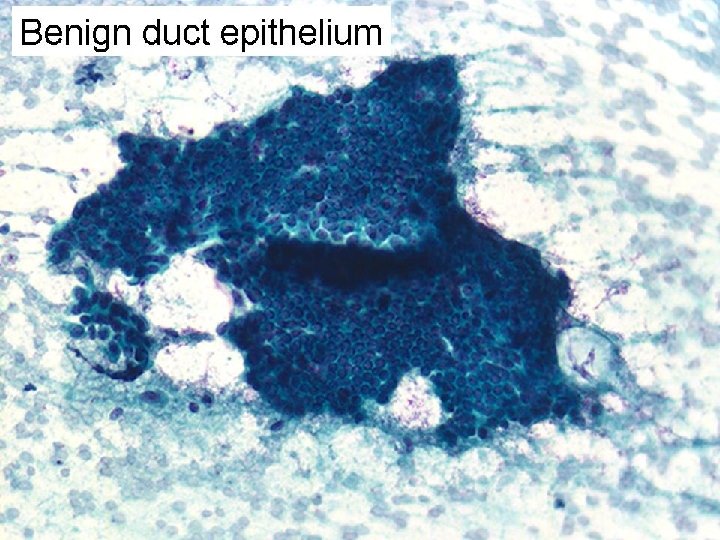
Benign duct epithelium • • Cohesive honeycombed sheets Regular round/oval evenly spaced nuclei Evenly distributed chromatin. No nucleoli Myoepithelial cells (in ductal sheets and in background) • Apocrine cells

Papilloma • • Cellular, bloody background Macrophages 3 dimensional papillary clusters, cell balls Tall columnar cells, apocrine cells and ME cells

Papillary carcinoma • Papilloma + • Necrotic debris • Atypical cytology High N/C ratio, hyperchromasia, nucleoli • Absence of apocrine cells and ME cells

FNA palpable masses FNA P a l p a b l e PATHOLOGY Negative Positive Total C 1 3 2 5 C 2 35 1 36 C 3 6 0 6 C 4 0 12 12 C 5 0 73 73 Total 44 88 132 • • 73% FNAs 67% malignant C 1: 3. 5% C 2: FCC (16), FA(18), PT (1), – DCIS crib +micropapa (1) FN • C 4: IDC (7), ILC (2), DCIS (2), Tubular (1)

FNA of non palpable masses PATHOLOGY FNA non palpable Negative Positive Total C 1 1 3 4 C 2 21 0 21 C 3 3 0 3 C 4 0 1 1 C 5 1 19 20 Total 26 23 49 • • 27% FNAs 47% malignant C 1: 8% C 5: 1 FP. Adenomyoepithilioma • The only FP in our 17 year experience (>2500 cases)
- Slides: 116