FLUIDS AND ELECTROLYTES Body Fluid Composition Water largest

FLUIDS AND ELECTROLYTES

Body Fluid Composition • Water – largest body component – 55 -65% total body weight • Solutes –dissolved in body water
 – Potassium (K+) –")
Solutes – Electrolytes • Cations – positive – Sodium (Na+) – Potassium (K+) – Calcium (Ca+2) • Anions – negative – Chloride (Cl-) – Bicarbonate (HCO 3 -) – Phosphate (HPO 4 -) – Non-electrolytes Proteins • • Urea Glucose Oxygen (O 2) Carbon dioxide (CO 2)

Body Maintains Charge and Osmolality • Body fluids – Electrically neutral – Osmotically maintained • Specific # solute molecules per volume fluid • Homeostasis of charge, osmolality maintained by – Ion transport – Water movement between fluid compartments – Kidney function
 • MW (molecular weight) = sum of weights")
Units of Solute Measurement (A Review) • MW (molecular weight) = sum of weights of atoms • m. Eq (milliequivalents) = MW (in mg) / valence – Valence = # charges of ion • Na+ valence = 1 • Cl- valence = 1 • Ca+2 valence = 2 – Allows comparisons of charge # of solutes in fluids, without molecular wts • Important to monitor overall charge of body fluids • m. Osm (milliosms) = # particles in solution – Particles = atoms or molecules, charged or uncharged – Measures concent of overall # of solute particles in fluid • Important to monitor overall concentrations of body fluids

Fluid Compartments • ICF = Intra. Cellular Fluid – Inside cells – 65% total body weight • ECF = Extra. Cellular Fluid – Not inside cells – 35% total body weight – Further divided

ECF – cont’d – IVF = Intra. Vascular Fluid • In blood vessels • 8% total body weight – ISF = Inter. Stitial Fluid • Bathes cells + lymph • 25% of total body weight
 • Solutes may be in higher concentration")
Movement of Body Fluids (WATER FOLLOWS SALT!) • Solutes may be in higher concentration on one side of the cell membrane • Fluid (water) can move to equilibrate concentration and/or charge on both sides of the membrane
 down concentration gradient to establish")
Definitions • Diffusion = net movement of particles (solutes) down concentration gradient to establish equilibrium between two sides of membrane – Passive (no energy needed) – Assisted (energy must be added by the cell) • Osmosis = diffusion of water – Freely passes through cell membranes.

Movement of Body Fluids – cont’d • ICF to ECF – Osmolality changes in ICF not rapid • Cell strives to maintain fluid and ion concentrations • Cell very dependent on relatively constant water/solute amounts – BUT if ECF osmolality changes so water moves among compartments, both compartments affected and equilibrated over time

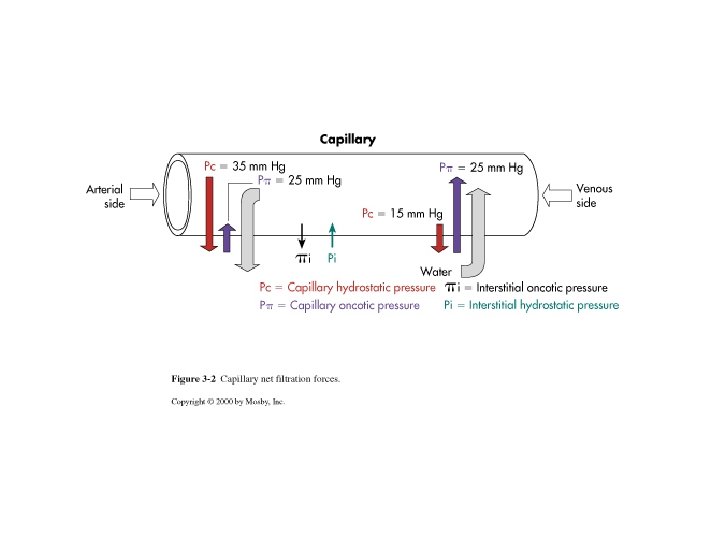
Movement of Body Fluids – cont’d • IVF to ISF to IVF – Happens constantly due to changes in fluid pressures and osmotic forces at arterial and venous ends of the capillaries – Necessary to move oxygen and nutrients toward metabolizing cells, and wastes and carbon dioxide away from metabolizing cells


Movement of Body Fluids – cont’d • Arteriolar end of the capillary: – Highest fluid pressure force -- Blood Hydrostatic Pressure (BHP) • • Pressing out against the capillary walls Direction toward cells Encourages movement out Due to fluid pressures and heart contractions – Colloid Osmotic Pressure (COP) • • Lower pressure at arteriolar end Pulls inward from capillary wall Encourages fluid to stay inside Due to large proteins, cells in capillary (too large to move through capillary walls, so remain in the capillary), can’t leave the bloodstream – Overall at arteriolar end of capillary, BHP > COP • Greater force encouraging fluid out of capillary than encouraging fluid to stay inside capillary • So fluid (from heart; oxygenated; w/ nutrients) encouraged to move toward metabolizing cells

Movement of Body Fluids – cont’d • At the venous end of the capillary: – BHP decreased • Fluid “lost” from vessel • Don’t have same high fluid pressure pushing against vessel walls – COP stays the same • Same amt large proteins, blood cells – Now rel higher pressure “pulling in” away from cells – Overall at venous end of capillary, COP > BHP • Greater force encourages fluid into capillary than encourages fluid out of capillary • Overall, fluid (from around cells; containing wastes and CO 2) encouraged to move into capillary – Now returned to lungs to excrete CO 2 and to kidneys to excrete wastes

Movement of Body Fluids – cont’d • ECF to environment – Fluid intake = fluid output • Intake is -- water, food, beverages • Output -- urine, feces, sweat and water vapor
 • If there")
Regulation of Body Water • Works through ADH (Anti. Diuretic Hormone) • If there is – Decreased amount water in the body, or – Increased amount Na+ in the body, or – Increased blood osmolality • So the blood is too concentrated, or – Decreased circulating blood volume • All of these lead to:

ADH Release – cont’d • Stim’n hypothalamic osmoreceptors, • Release ADH, and • Stimulation of thirst response – Thirst response increased drinking • Overall, water volume within the body increases

ADH – cont’d • ADH works at kidney – incr’d permeability of kidney tubules to water – incr’d reabsorption of water from kidney tubules back into blood vasculature • Water WOULD have been released to urine • So water is conserved, not excreted
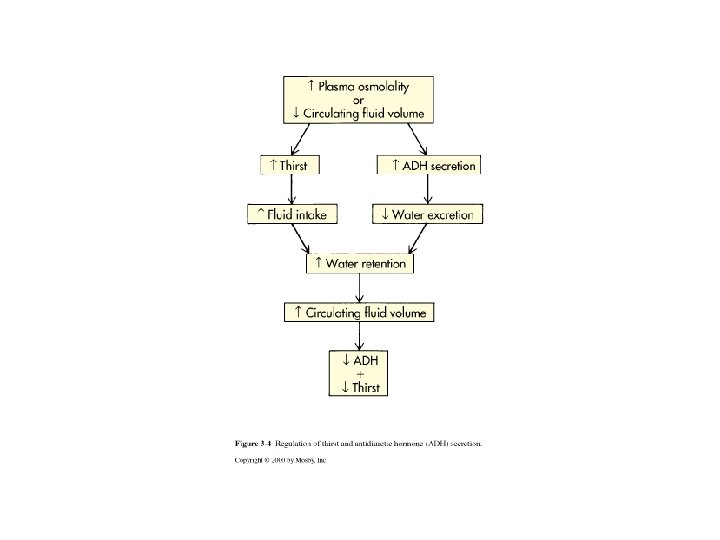

ADH – cont’d • Overall: – Incr’d water consumption, and – Incr’d water conservation, so – Incr’d amt water in body • Relieves decr’d water, decr’d circulation blood volume – Decr’d blood osmolality • Relieves increased body Na+, increased blood osmolality • Note: the various conditions leading to ADH release can all be caused by different dysfunctions or traumas, but are all related physiologically – If either hemorrhage (decr’d blood volume) or sweating (decr’d water in body) decr’d fluid available decr’d IVF decr’d blood pressure • Compensation: body tries to increase fluids in body – If endocrine disorder incr’d Na+ incr’d blood osmolality • Compensation: body tries to increase fluids to bring blood osmolality back to normal range (since body can’t n; ormalize osmolality through solute amount) • So if sodium LOAD has doubled to 290 m. Eq/L: if fluid VOLUME can double, will now have 290 m. Eq/2 L, which = 145 m. Eq/L (normal sodium CONCENTRATION is 145 mg/L)

ADH – cont’d • Note: conditions ADH release, regardless of cause, related physiologically – Hemorrhage (decr’d blood volume) or sweating (decr’d water in body) • decr’d fluid available decr’d IVF decr’d blood pressure • Compensation: body tries to increase fluids in body – Endocrine disorder incr’d Na+ incr’d blood osmolality • Compensation: body tries to increase fluids (body can’t normalize osmolality through solute amount) • Ex: Na+ LOAD doubled (290 m. Eq/L); by doubling fluid VOLUME 290 m. Eq/2 L= 145 m. Eq/L (normal sodium CONCENTRATION is 145 mg/L)
 – About 90% ECF")
Important Cations Contributing to Body Fluid Osmolality • Sodium (Na+) – About 90% ECF cations – Normal range = 136 -145 m. Eq/L in ECF – Pairs with Cl-, HCO 3 - to neutralize charge – Low in ICF (~10 m. Eq/L) – Most impt ion in regulating water balance

Sodium – cont’d – Regulation in ECF -- Renal tubule reabsorption, modulated by hormones: • Aldosterone – Rel’d from adrenal gland when body senses decr’d Na+ load – Works at renal tubule to incr renal tubule reabsorption of Na+ • Renin/angiotensin – Affects aldosterone release (also controls Na+ reabsorption) • Natriuretic hormone – Works at kidney – decr’d renal reabsorption of Na+

Potassium • Major INTRAcellular cation • ICF concentration = 150 -160 m. Eq/L • Lower in ECF (3. 5 -4. 5 m. Eq/L) – K+ concentration INSIDE cells approximates Na+ concentration OUTSIDE – Na+ concentration INSIDE cells approximates K+ concentration OUTSIDE – Body keeps electrical charge constant in ICF and ECF, but uses diff cations inside/outside cells • Cell moves two cations differently, uses each differently – Overall cells strive to maintain high K+ inside and high Na+ outside

Potassium – cont’d • Why keep K+ high inside and Na+ high outside cells? – Resting membrane potential in neurons, muscles • Na+, K+ move into/out of these cells depolarization action potential • If imbalanced, can neurological, muscle contraction problems • REMEMBER: heart is an important muscle!

Potassium – cont’d • K+ also important: – Regulates fluid, ion balance inside the cell • Sim to Na+ regulation outside the cell – p. H regulation • K+ can move across the cell membrane for H+ when H+ is in excess (body fluids are too acidic) • Regulation of body K+ is through the kidney – Aldosterone regulates K+ • If body senses decr’d K+ in plasma aldosterone release • Works at kidney tubule incr’d reabsorption of K+ from tubule back to blood (similar to Na+ mechanism) – Insulin increased K+ taken up by cells • So K+ must be monitored in diabetic patients

Isotonic Alterations • Volume of fluid changes, but numbers and types of electrolytes remain at normal levels (Table 4 -5) – Loss volume depletion (hypovolemia); occurs with • • • Hemorrhage Severe wound drainage Excess sweating Burns Third spacing

Hypovolemia – cont’d – Fluid lost from blood vessels, but remains in body – Receptors in the vessels sensitive to pressure – Interpreted as fluid loss, so decr’d ECF volume • Decr’d urine output • Weight loss (through fluid weight) • Can hypovolemic shock – Symptoms of hypovolemia • Decr’d blood pressure • Incr’d heart rate

Hypervolemia • Excess body fluid; occurs with: – Excessive IV fluids – Overproduction aldosterone • Why should this lead to hypervolemia? – Some drugs (ex: cortisol) – With incr’d ECF volume • • Weight gain (fluid weight) Diluted urine Incr’d blood pressure Can also edema

Edema -- ECF Isotonic Volume Excess • Accum’n isotonic fluid in interstitial space (incr’d ISF) • Forces that favor incr’d ISF also favor edema: – Incr’d BHP, if • Chronic hypertension • Venous obstruction • Water retention – Decr’d COP if • Not enough proteins/cells in the blood: – Protein synthesis disorders of liver – Blood cell disorders decreased # of blood cells

Edema – cont’d – Increased capillary permeability, which can occur with • Trauma • Inflammation • Decreased lymph drainage with – Blocked lymph node – Surgical removal of lymph vessels – REMEMBER: ISF drains into lymph vessels, which returns ISF to the bloodstream
 – Neck")
Edema – cont’d • Clinical – Pitting – Weight gain (water weight) – Neck vein distension – Incr’d blood pressure • Treatment – Treat underlying conditions (tumor, blood cell disorder, etc. ) – Relieve symptoms
: Sodium • Hypernatremia (a hypertonic imbalance) – Plasma Na+")
Electrolyte Imbalances (Table 4 -6): Sodium • Hypernatremia (a hypertonic imbalance) – Plasma Na+ > 145 m. Eq/L – Too much Na+ or too little water – “Tonicity”: # of solute particles in solution • Hypertonic -- high amt solute • Hypotonic = dilute – Characteristics of hypernatremia: • movement of water from ICF to ECF, so – Cells dehydrate – Overall incr’d ECF vol (at expense of the cell vol)

Sodium Imbalances – cont’d • Hypernatremia – cont’d – Due to • • Admin hypertonic IV sol’ns Oversecretion aldosterone Loss of pure water Long term sweating w/ chronic fever Respiratory infection water vapor loss Diabetes polyuria Insufficient water ingested

Sodium Imbalances – cont’d • Hypernatremia – cont’d – Clinical • Thirst • Lethargy • Neurological dysfunction (dehydration of brain cells) – Treatment • Lower serum Na+ • Use isotonic salt-free IV fluid (5% glucose) to replace body water; returns Na+ concentration to normal levels

Sodium Imbalances – cont’d • Hyponatremia – Overall Na+ decr ECF – Two types • Depletional: Too little Na+ • Dilutional: Too much water – Causes of each type • Depletional (Na+ lost out of body or insufficient) – Diuretics – Chronic vomiting – Chronic diarrhea » Though electrolytes loss – Decr’d aldosterone – Decr’d Na+ intake

Sodium Imbalances – cont’d • Hyponatremia – cont’d • Dilutional – Renal dysfunction w/ incr’d hypotonic fluid intake – Excessive sweating increased thirst intake excessive pure water • Syndrome of Inappropriate ADH (SIADH) impaired renal excretion of water • Excessive beer drinking (? ? ? ) – Clinical • Neurological symptoms – Now improper Na+ concentration outside cell improper depolarization/action potential/neuron conduction – Seizures possible – Treatment • Restrict water, or • Administer Na+

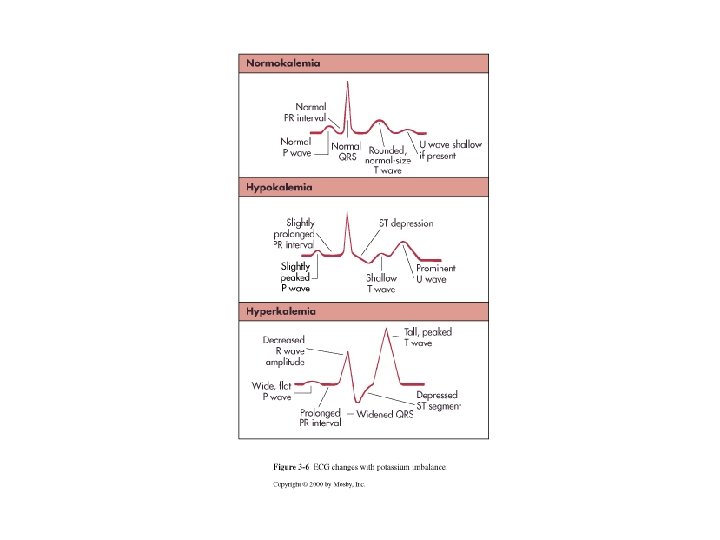
Electrolyte Imbalances: Potassium • Hypokalemia – Characteristics • Serum K+ < 3. 5 m. Eq/L • Beware if diabetes: – Insulin plays a role in K+ into the cell – Ketoacidosis incr’d H+ in ECF (so ECF too highly + charged) » H+ enters cells » Body tries to equilibrate + charges by moving K+ out of cells » Now ECF high in K+ (lost through urine) » Overall whole body K+ deficit

Potassium Imbalances – cont’d • Hypokalemia – cont’d – Causes • Decr’d K+ intake (rare) • Incr’d K+ loss – With chronic diuretics, g. i. disturbance – Acid/base imbalance K+ out of cells into ECF, then lost through urine • Clinical – Neuromuscular disorders – Cardiac arrest • REMEMBER: Na+/K+ gradient for proper action potentials in neurons/muscles – Treatment • Increase K+ intake • BUT slowly to avoid abrupt Na+/K+ gradient change

Potassium Imbalances – cont’d • Hypokalemia – cont’d • Clinical – Neuromuscular disorders – Cardiac arrest – REMEMBER: body maintains Na+/K+ gradient for proper action potentials in neurons/muscles so proper neuron/muscle function – Treatment • Increase K+ intake • BUT must be increased slowly to avoid abrupt Na+/K+ gradient change

Potassium Imbalances – cont’d • Hyperkalemia – Serum K+ > 5. 5 m. Eq/L – Importance/causes/when to check • Renal disease (kidney regulates K+) • Massive cellular trauma – High intracellular K+ is released into ECF • Insulin deficiency – Insulin plays a role in K+ uptake into cells • Addison’s disease altered aldosterone secretion • Decr’d blood p. H (high blood acidity) – – H+ into cells K+ out of cells ECF High K+ in ECF BUT over time K+ will be lost to urine overall decrease in body K+

Potassium Imbalances – cont’d • Hyperkalemia – cont’d – Clinical • Muscle weakness, paralysis • Change in ECG pattern – Treatment • Insulin + glucose K+ taken into the cells (out of ECF) • Bicarbonate – buffers H+ ions if hyperkalemia due to acidosis • Ca+2 counteracts K+ effects on heart
- Slides: 44