Fluids and Electrolytes Balance Josierina Y Sarmiento M

Fluids and Electrolytes Balance Josierina Y. Sarmiento, M. D. Nephrologists Asian Hospital and Medical Center

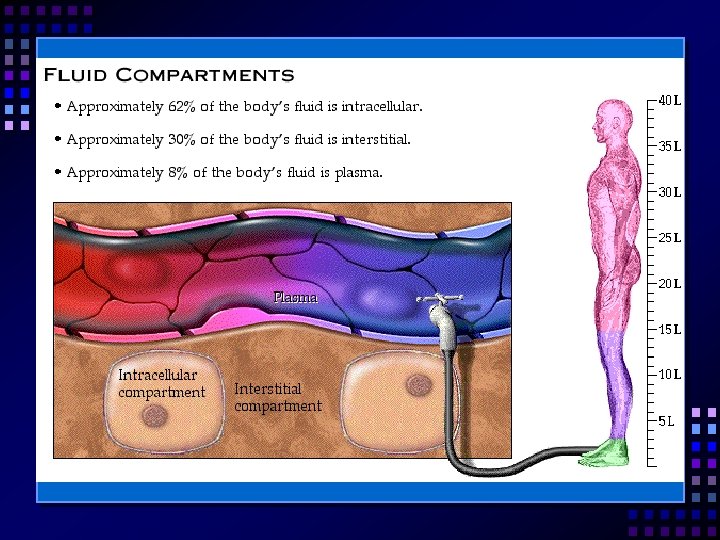
Body Fluids Man have 60% Woman have 50% Fat contains little water % of body weight that is water decreases with age
 Extracellular Fluids (ECF) ¾ ¼")
Body Fluid Compartment Intracellular Fluids (ICF) Extracellular Fluids (ECF) ¾ ¼
 Supplies the food, oxygen, water, vitamins and electrolytes and takes away")
Extracellular Fluids (ECF) Supplies the food, oxygen, water, vitamins and electrolytes and takes away body waste.

Fluid Spacing First spacing – normal amount of fluids in both the extracellular and intracellular compartments. Second spacing – an excess accumulation of intestinal fluid (edema). Third spacing – fluid accumulation in areas that normal have no fluids or minimal amount of fluids. (Ascites)

Electrolytes A. B. Solutes and substances that are dissolved in body fluids. Electrolytes Non – electrolytes Compounds that do not separate into charged particles when dissolved in water……GLUCOSE

Electrolytes are compounds that do not separate into charged particles called ions. Cations – positively charged ions such as Na+. Anions – negatively charged ions such as Cl-.
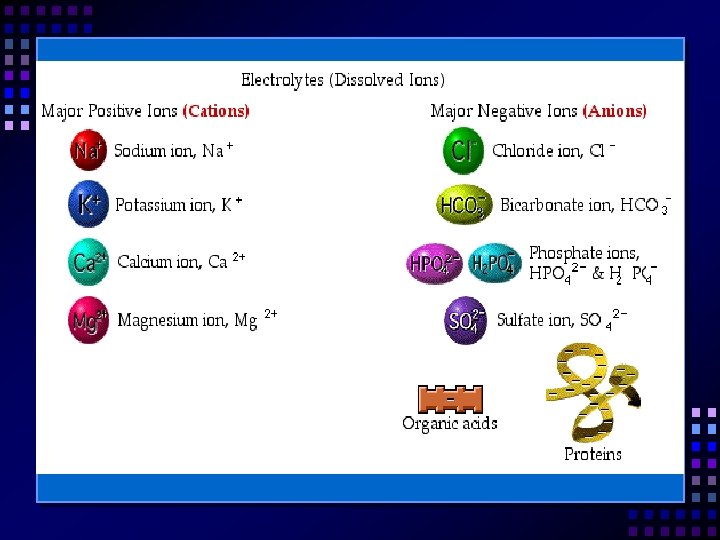

Electrolytes are found inside and outside of the cell. ECF ICF Na+ Cl– HCO 3– K+ SO 4+ PO 4+

Normal Fluid Intake and Losses in Adults Intake Water in food = 1000 ml Output Skin = 500 ml Lungs 350 cc Insensible losses Water for oxidation = 300 Feces = 150 cc Water as liquid = 1200 ml Kidneys = 1500 cc 2500

Fluid and Electrolyte Exchange

Diffusion Molecules and ions flow through a semi permeable membrane from an area of higher concentration to an area of lower concentration.

Osmosis Movement of water through a semi permeable membrane from a weaker solution to the more concentrated solution The in intent is to equalize the strength of solution.

Osmotic Pressure Osmotic pressure – is the pulling of water in the process of osmosis. Osmolarity – an indication of whether a person is adequately hydrated, over by drated or dehydrated. Normal: 275 – 295 m. Osm/kg

Osmotic Movement of Fluids Isotonic – fluids that have the same osmolarity as the fluid inside the cell. Example: Plain LR and plain NSS Has the same concentration as inside the cells

Hypotonic / Hypoosmolar Hypotonic – fluids that contain more water than the intercellular fluids. Example: ½ NSS Hypotonic fluid surrounds the cells and causes the water to move inside the cell until it burns.
 than")
Hypertonic Solution Hypertonic solutions – are fluids that contain less water (more concentrated) than intracellular fluids. Hypertonic solution around the cells draws water from the cell until it shrinks.

Hypotonic Solution Water ½ NSS Burst

Hypertonic Solution 3% Na. Cl Shrinks

Hydrostatic Pressure – is the force exerted by fluids against the wall of it containers. Hydrostatic Pressure – is the major force in the movement of water out of the capillaries.

Oncotic Pressure Oncotic pressure – is also known as colloidal osmotic pressure that is the presence caused by colloids in the solution. Colloids – are particles that are too large to pair through a semi permeable membrane. Example: protein

Capillary Fluid Movement The amount and direction of fluid movement is based on the hydrostatic pressure and oncotic pressure.

Capillaries Hydrostatic Venous Pressure End Oncotic Pressure Arterial End

Fluid Shift Edema – imbalance between hydrostatic and oncotic pressure. Hydrostatic pressure • CHF, tourniquet Oncotic pressure • Malnutrition • Nephrotic syndrome

Regulation of Fluids and Electrolytes Hypothalamus – the thirst mechanism that stimulates us to drive. It is stimulated by increased in serum osmolality. Hormones: ADH (antidiuretic hormone) – acts on the renal tubules to retain water and decrease urinal outputs Aldosterone – increases sodium and water reabsorption.

Fluids and Electrolytes Imbalances Hypovolemia – decreased in intravascular fluid volume. Occurs when water and electrolytes are lost or unavailable to circulation. Diarrhea, massive bleeding, excessive sweating (marathon, runners), vomiting.

Assessment of Hypovolemia Decreased body temperature Low blood pressure Tachycardia Weak pulse Increased respiration Weakness Weight loss Decreased urine output Increased Hab/Hct

Treatment of Hypovolemia Fluids

Hypervolemia is the excess of water and electrolytes in the ECF. Renal failure Congestive heart failure

Assessment of Hypervolemia Acute weight gain Cardiac enlargement, cyanosis Decreased Hct, Hab, RBC’s Skin warm and moise Pitting edema Puffy eyelids Bounding pulse Dyspnea, increased respiratory rate Distended neck vein

Treatment for Hypervolemia Sodium restriction Limit fluid intake Diuretics

Electrolyte Balance Each electrolyte has its very own function. Too much or too little may alter the function. Electrolytes concentration may be altered by changing the quantity of the electrolyte or by altering the quantity of water in the ECF in which electrolytes is found.

Sodium is the chief cat ion in the ECF. NV = 135 – 145 m. Eq/L Sodium function include transmission of nerve impulses, maintain acid-base balance, regulate water reabsorption and excretion in kidney tubules.

Sodium Normal Na intakes is 2 to 4 grams Hypernatremia – too much Na in the intravascular space; cause cell to shrink Hyponatremia – too little Na in the intravascular space, cause the cell to swell. Aldosterone – reabsorbs Na in the kidney tubules

Defining Characteristics of Hyponatremia Serum Na < 135 m. Eq/L Serum osmolality Anorexia and nausea Lethargy Confusion, seizures, coma Muscle twitching

Nursing Intervention for Hyponatremia Encourage diet high sodium Weigh daily Monitor neurological status Monitor serum Na levels Maintain free water intake

Food High in Sodium Potato chips Bacon / catsup Table salt Crackers Cheese Pretzels, etc. Luncheon meat

Hypernatremia Serum Na greater than 145 m. Eq/L Due to water deficit Serum osmolality > 295 m. Osm/kg.

Defining Characteristic of Hypernatremia Dry tongue Thirst Fever Oliguria CNS symptoms including focal or grand mal seizures

Nursing Intervention for Hypernatremia Encourage low Na diet Accurate I; O Hypotonic fluids Observe for seizure

Chloride is the major extracellular anion Part of hydrochloric acid in the stomach When Na is reabsorbed so is Cl

Potassium is the major intracellular cat ion. Function: 1. ICF balance 2. Maintain regular heart rhythm 3. Conducts neuromuscular impulses 4. Regulation of acid-base balance Normal potassium range: 3. 5 – 5. 0 m. Eq/L

Reasons for Hypokalemia Diarrhea Ostomies Loop diuretics Poor intake of K rich foods Stress

Defining Characteristics Hypokalemia Serum K+ level less than 3. 5 m. Eq/L Muscle weakness Cardiac arrhythmias Increased sensitivity to digitalis toxicity Muscle weakness Fatigue ECG changes: ST depression / U wave

Nursing Intervention for Hypokalemia Encourage high K foods Monitor EKG results IV/oral Potassium replacement

Foods high in Potassium All dried fruits/banana Spinach Beef Chocolate Potato’s Tomato’s

Hyperkalemia Renal insufficiency. High potassium intake. Shift of potassium out of the cell as in acidosis.

Defining Characteristics of Hyperkalemia Potassium levels greater than 5. 0 m. Eq/L Neuromuscular weakness EKG changes – peaked T waves widened QRS complex Flaccid muscles paralysis Heart block

Nursing Intervention for Hyperkalemia Monitor EKG changes Administer calcium solutions to neutralize the potassium Monitor muscle tone Give kayexalate Glucose + insulin solution Diuretics

Calcium For transmission for nerve impulses For muscle contraction Blood clotting Bone and tooth formation Normal level: 8. 6 – 10. 6 mg/dl 2 hormones: 1. Parathormone 2. Calcitonin

Reasons for Hypocalcemia Vitamin D deficiency Malabsorption Excessive GI loss hypoparathyroidism

Defining Characteristic of Hypocalcemia Membranes, tingling of fingers Tetany and cramps Trosseau’s sign – carpal spasms Chvostek’s sign – cheek twitching Seizures, mental changes EKG shows prolonged QT intervals Treatment: Calcium carbonate / calcium gluconate

Hypercalcemia Hyperparathyroidism Thiazide diuretics Malignancy Renal failure Antacids Serum calcium: > 10. 5 mg/dl EKG: shorted QT intervals Treatment: calcium from the diet

Acid Base Balance Acids – substance that can release hydrogen ions Bases – substance that can accept hydrogen ions Hydrogen ions determine whether a solution is acidic, basic or neutral Normal p. H: 7. 35 – 7. 45 Buffer system: carbonic acid / bicarbonate

Metabolic Acidosis a base bicarbonate deficit Normal HCO 3; 22 – 26 m. Eq/L Comes from too much acid and loss of bicarbonate S/s: p. H < 7. 35, increased K+ levels DKA (Kussmaul’s, breathing) Shock, stupor, coma Nursing intervention – give HCO 3

Metabolic Alkaloses A base bicarbonate excess A result of a loss of acid and a accumulation of base. S/s: serum p. H > 7. 45, increased serum HCO 3, serum K levels > 5. 0 tetany, convulsions, seizures Nursing intervention – watch for S/s of hypokalemia

Respiratory Alkalosis A deficit of carbonic acid caused by hyperventilation Normal p. CO 2: 35 – 45 Decreased levels of p. CO 2, increased levels of p. H, HCO 3 = normal. Nursing intervention – monitor for anxiety (breath in brown paper bag).

Respiratory Acidosis A carbonic acid excess Caused by condition that interferes with the release of CO 2 from the lungs (sedatives, COPD, narcotics) S/s: serum p. H < 7. 35, p. CO 2 levels, cyanosis Nursing intervention: provide O 2

Interpretation of Arterial Blood Gases Pyramid points: If acidosis the p. H is down If alkolosis the p. H is up The reparatory function indicator is the p. CO 2 The metabolic function indicator is the HCO 3

Step I Look at the p. H Is it up or down? If it is up: it reflects alkalosis If it is down: it reflects acidosis

Step II Look at the p. CO 2. Is it up or down. If it reflects an opposite response as the p. H, then you know that the condition is a respiratory imbalance. If it does not reflect as opposite response as the p. H – move to step III.

Step III Look at the HCO 3 Does the HCO 3 reflect a corresponding response with the p. H? If it does then the condition is a metabolic imbalance

Example # 1 PO 2 p. H p. CO 2 HCO 3 BE RR O 2 99. 5 7. 29 41 meq/L 19 - 17 22 2 L/NC

Answer Metabolic Acidosis

Example # 2 PO 2 p. H p. CO 2 HCO 3 BE RR Room air 98 7. 50 30 meq/L 29 meq/L + 20 28

Answer Respiratory Alkalosis
 Hyperalimentation Provide life sustaining therapy for patients who cannot take")
Total Parental Nutrition (TPN) Hyperalimentation Provide life sustaining therapy for patients who cannot take adequate food by mouth and who consequently are at risk for malnutrition and its effects.

Indications for TPN Perioperative nutrition Critical illness Cancer cachexia Liver failure Renal failure Inflammatory bowel disease Short bowel syndrome Pulmonary disease HIV Pregnancy

Energy Requirement Hypometabolic state 20 Kcal/kg x e. g. 70 kg man 1, 400 Kcal Hypermetabolic state (sepsis trauma) 40 Kcal/kg x e. g. 70 kg man 1, 800 Kcal

Conditionally Essential Nutrients Glutamine – immunocyte fuel for enterocyte and Nucleotides – mediators for many metabolic process Branched chain – regulates muscle amino acid, protein breakdown
 – normalizes cell wall fluidity Short chain fatty")
Conditionally Essential Nutrients SAM (S-adenosyl methionine) – normalizes cell wall fluidity Short chain fatty acid – fuel for colonocyses Omega 3 fatty acids – promotes production of prostaglandin

Commercially Available TPN Nutripack 1, 200 Kcal, 1, 900 Kcal Nutroflex 1, 200 Kcal, 1, 900 Kcal Kabiven 1, 400 Kcal Vitrimix Intralipids Vamin glucose Vamin 14 Nephrosteril

Infusion Technique and Patient Monitoring 1. Peripheral line: isotonic fat solution, shortterm 2. Central venous line: long-term, using glucose as the chief energy source
 a. Saline (Plain NSS) 154 meq Na 0. 9% Hypovolemic")
Fluids Isotonic Fluids (Crystalloids) a. Saline (Plain NSS) 154 meq Na 0. 9% Hypovolemic shock

Fluids Hypotonic Fluids a. ½ NSS = 77 meq Na = 0. 45% b. Dextrose in water D 5 water = 5 grams glucose D 10 water = 10 grams glucose For hypernatremic patients

Fluids Hypertonic solution 3% Na. Cl Use in hyponatremic patients Na. HCO 3 For acidotic patients
 Lactated ringers KCl Use for")
Fluids Polyionic solutions 1. 2. 3. Ringers (Plain LR) Lactated ringers KCl Use for diarrhea
 a. Haeteril (10% or 5%) b. Haemacel c. Gelafurdin")
Fluids Colloids Starch (Hydroxyethyc Starch) a. Haeteril (10% or 5%) b. Haemacel c. Gelafurdin Hypovolemic shock

Thank you!
- Slides: 80