FLUID THERAPY Body Fluid Compartments 23 X 5070

FLUID THERAPY

Body Fluid Compartments: 2/3 X 50~70% lean body weight ICF: 55%~75% TBW 3/4 • • • Male (55%) > female (45%) Most concentrated in skeletal muscle TBW=0. 6 x. BW ICF=0. 4 x. BW ECF=0. 2 x. BW 1/3 ECF 1/4 Extravascular Interstitial fluid Intravascular plasma
 • TBW varies with age , gender and body habitus")
Total body water (TBW) • TBW varies with age , gender and body habitus • In adult males= 55% of body weight • In adult female=45% of body weight • In infant = 80% of body weight • Obese patients have less TBW per Kg than lean body adult.
=55% TBW or 30%-40% BW 2= Extracellular fluid")
Body compartment fluid 1= Intracellular fluid (ICF)=55% TBW or 30%-40% BW 2= Extracellular fluid (ECF) =45%TBW or 20% BW • Interstitial fluid =15% of body weight • Intravascular fluid or plasma volume = 5% of body weight

Fluid compartments ICF

Fluid compartments ICF Plasma Interstitial ECF

Fluid compartments ICF Plasma Interstitial ECF

Fluid compartments Capillary Membrane ICF Plasma Interstitial ECF

Fluid compartments Capillary Membrane ICF Plasma Interstitial ECF

Fluid compartments Capillary Membrane Cell Membrane ICF Plasma Interstitial ECF

Colloid osmotic pressure Capillary Membrane Plasma Interstitial ECF Capillary membrane freely permeable to water and electrolytes but not to large molecules such as proteins (albumin).

Colloid osmotic pressure Capillary Membrane Plasma Interstitial ECF Capillary membrane freely permeable to water and electrolytes but not to large molecules such as proteins (albumin).

Colloid osmotic pressure Capillary Membrane Capillary membrane freely permeable to water and electrolytes but not to large molecules such as proteins (albumin). H 2 O Plasma Interstitial H 2 O ECF The albumin on the plasma side gives rise to a colloid osmotic pressure gradient favouring movement of water into the plasma

Colloid osmotic pressure Capillary Membrane Capillary membrane freely permeable to water and electrolytes but not to large molecules such as proteins (albumin). H 2 O 120/80 Plasma Interstitial H 2 O ECF The albumin on the plasma side gives rise to a colloid osmotic pressure gradient favouring movement of water into the plasma This is balanced out by the hydrostatic pressure difference

Starling equation Q=Pc-Posm

Cell Membrane H 2 O ICF Interstitial Cell membrane is freely permeable to H 20 but

Cell Membrane H 2 O Interstitial ICF Na+ K+ Cell membrane is freely permeable to H 20 but Na and K are pumped across this membrane to maintain a gradient!
![Cell Membrane H 2 O Interstitial ICF Na. K+ [K+] =4 Cell membrane is](http://slidetodoc.com/presentation_image_h/eae2949dafe4acb02b3f826409644d14/image-18.jpg "Cell Membrane H 2 O Interstitial ICF Na. K+ [K+] =4 Cell membrane is")
Cell Membrane H 2 O Interstitial ICF Na. K+ [K+] =4 Cell membrane is freely permeable to H 20 but Na and K are pumped across this membrane to maintain a gradient!
![Cell Membrane H 2 O Interstitial ICF Na. K+ [K+] =4 [K+] =150 Cell](http://slidetodoc.com/presentation_image_h/eae2949dafe4acb02b3f826409644d14/image-19.jpg "Cell Membrane H 2 O Interstitial ICF Na. K+ [K+] =4 [K+] =150 Cell")
Cell Membrane H 2 O Interstitial ICF Na. K+ [K+] =4 [K+] =150 Cell membrane is freely permeable to H 20 but Na and K are pumped across this membrane to maintain a gradient!
![Cell Membrane Na+= 144 H 2 O Interstitial ICF Na. K+ [K+] =4 [K+]](http://slidetodoc.com/presentation_image_h/eae2949dafe4acb02b3f826409644d14/image-20.jpg "Cell Membrane Na+= 144 H 2 O Interstitial ICF Na. K+ [K+] =4 [K+]")
Cell Membrane Na+= 144 H 2 O Interstitial ICF Na. K+ [K+] =4 [K+] =150 Cell membrane is freely permeable to H 20 but Na and K are pumped across this membrane to maintain a gradient!

Cell Membrane Na+= 144 H 2 O Na+= 10 H 2 O Interstitial ICF Na. K+ [K+] =4 [K+] =150 Cell membrane is freely permeable to H 20 but Na and K are pumped across this membrane to maintain a gradient!

Composition of Body Fluids: Cations 150 Anions 100 50 0 ECF Na+ Cl. HCO 3 Ca 2+ Mg 2+ Protein K+ Organic anion ICF 50 PO 43 - 100 150 Osmolarity = solute/(solute+solvent) Osmolality = solute/solvent (290~310 m. Osm/L) Tonicity = effective osmolality Plasma osmolility = 2 x (Na) + (Glucose/18) + (Urea/2. 8) Plasma tonicity = 2 x (Na) + (Glucose/18)
 ICF (mmol/L) Na+ 143 9 K+ 5")
Composition body fluid compartments Ion Plasma (mmol/L) ICF (mmol/L) Na+ 143 9 K+ 5 135 Ca 2+ 1, 3 <0, 8 Mg 2+ 0. 9 25 Cl- 9 HCO 3 - 103 24 HPO 42 - 0, 4 74 Sulphate- 0, 4 19 - 9
 Na+* K+ Cl- HCO 3 -")
Composition of GI Secretions Source Volume (ml/24 h) Na+* K+ Cl- HCO 3 - Salivary 1500 (500~2000) 10 (2~10) 26 (20~30) 10 (8~18) 30 Stomach 1500 (100~4000) 60 (9~116) 10 (0~32) 130 (8~154) 0 100~2000 140 5 80 0 Ileum 3000 140 (80~150) 5 (2~8) 104 (43~137) 30 Colon 100 -9000 60 30 40 0 Pancreas 100 -800 140 (113~185) 5 (3~7) 75 (54~95) 115 Duodenum * Average concentration: mmol/L

Sweat: Na 10 -70 m. Eq/L Cl 5 -60 m. Eq/L K 1 -15 m. Eq/L Mg 0. 2 -5 m. Eq/L Urine: Na 50 -250 m. Eq/24 h K 30 -120 m. Eq/24 h Cl 100 -250 m. Eq/24 h

Questions to ask before prescribing fluid • Does my patient need intravenous fluid? • Why does my patient need intravenous fluid? • How much and which fluid does he need?

Does he need fluid? • May be drinking • May be on NG feed/TPN – both of these contain fluid which counts as maintenance • May be receiving many drug infusions e. g. antibiotics/paracetamol – can amount to 1+ litre/day • He may only need a bit of maintenance fluid • This calculation should be done for each patient

Why does he need fluid? • Maintenance –water and electrolytes • To supply the daily needs – (e. g. 4% dextrose/0. 18%saline/KCl) • Replacement To replace ongoing losses • know the content of the fluid! (usually crystalloid) • Resuscitation - e. g. colloid/blood • To correct an intravascular or extracellular volume deficit

Fluid balance charts Always calculate the balance between inputs and outputs
 • Sweat")
Sources of daily water loss • Urine 1200 -1500 ml/d (30 ml/hr) • Sweat 200 -400 ml/d • Lungs 500 ml/d • Feces 100 -200 ml/d

Daily Electrolyte loss Na+ Na 100 m. Eq K+ 100 m. Eq Cl- 150 m. Eq
 Sodium approx 1 mmol/kg Potassium approx 1")
Daily Requirements Water 25 -35 ml/kg (30) Sodium approx 1 mmol/kg Potassium approx 1 mmol/kg Calories minimum 400 Calories (i. e. 100 g dextrose) (calories help to deal with electrolytes normally)

Average Daily Requirements • 70 kg man needs: 2100 ml H 2 O 70 mmol Na+ 70 mmol K+ 70 mmol Cl • 50 kg man needs 1500 ml H 2 O 50 mmol Na+ 50 mmol K+ 50 mmol Cl-
 Osmolality (m. Osm/kg) p.")
Properties of Commonly Used Crystalloid Solutions Solution Electrolyte Content (mmol/l) Osmolality (m. Osm/kg) p. H 0. 9% Na. Cl Na+ 154 Cl- 154 308 5. 0 Dextrose (4%)Saline (0. 18%) Na+ 31 Cl- 31 286 4. 5 Nil 280 4. 0 276 6. 5 5% Dextrose Hartmann’s Na+ 131 Cl- 111

MAINTENANCE If you were on a desert island, would you drink from the sea or a stream? 0. 9% saline is not a maintenance fluid

MAINTENANCE • Prescribe maintenance if not drinking >6 hrs • 4%/0. 18% dextrose/saline with 20 mmol potassium in 500 ml, or 40 mmol in 1 litre (1 litre is cheaper). Or no potassium • Prescribe in ml/hr via a pump. • The correct volume of this by weight per day for maintenance will provide roughly the correct amount of sodium and potassium for each patient. Maximum 100 ml/hr to avoid hyponatraemia.

Potassium • A normal serum potassium is not an indication that the patient does not need potassium – it just means that their stores haven’t run out yet. • A low potassium means that losses are high and body stores very low. • A high potassium may be drug related but commonly is due to acute renal failure – monitor U&Es and do not give extra K. • Remember that TPN, NG feed and food contain K

Sodium • We all need some. However most drugs contain sodium so we don’t need to give a lot in fluids unless the patient is losing it. • Causes of a low Na – too much fluid (commonest cause in hospital!) – fluid restrict • SIADH inappropriate antidiuretic hormone secretion– pneumonia, brain pathology • High Na loss – usually upper GI losses – tend to be obvious

4 – 2 – 1 Rule • 100 – 50 – 20 Rule for daily fluid requirements • 4 m. L/kg for 1 st 10 kg • 2 m. L/kg for 2 nd 10 kg • 1 m. L/kg for each additional kg

Maintenance Fluids: Example • 60 kg female • 1 st 10 kg: 4 m. L/kg x 10 kg = 40 m. L • 2 nd 10 kg: 2 m. L/kg x 10 kg = 20 m. L • Remaining: 60 kg – 20 kg = 40 kg 1 m. L/kg x 40 kg = 40 m. L • Maintenance Rate = 120 m. L/hr

REPLACEMENT • Losses should be accounted for with replacement fluid: balanced solution( Hartmanns – Ringers Lactate) • Work out how much patient is losing and replace this with Hartmanns or RL – better to calculate retrospectively and replace. • Fluid prescriptions for losses must be reviewed regularly and updated.
 • Blood Loss")
Fluid Deficits • Fasting • Bowel Loss (Bowel Prep, vomiting, diarrhea) • Blood Loss – Trauma – Fractures • Burns • Sepsis • Pancreatitis

LOSSES • Upper GI loss: stomach, small bowel ileostomy/fistula/bile leak: high Na and Cl content – may become hypochloraemic and alkalotic – appropriate to use 0. 9%Na. Cl • Lower GI loss: diarrhoea - lose lots of water and potassium: Hartmanns or RL is appropriate to replace + extra potassium
 Fluid Sequestration (bowel, lung) Extent")
Insensible Fluid Loss Evaporative Exudative Tissue Edema (surgical manipulation) Fluid Sequestration (bowel, lung) Extent of fluid loss or redistribution (the “Third Space”) dependent on type of surgical procedure • Mobilization of Third Space Fluid POD#3 • • •

Insensible Fluid Loss • • • 4 – 6 – 8 Rule Replace with Crystalloid (NS, LR, Plasmalyte) Minor: 4 m. L/kg/hr Moderate: 6 m. L/kg/hr Major: 8 m. L/kg/h

Replacement Strategies • • • Sweat: D 5¼NS + 5 m. Eq KCl/L Gastric: D 5½NS + 20 m. Eq KCl/L Biliary/pancreatic: LR Small Bowel: LR Colon: LR 3 rd space losses: LR

Example 68 kg female for laparoscopic cholecystectomy Fasted since midnight, OR start at 8 am Maintenance = 40 + 20 + 48 = 108 m. L/hr Deficit = 108 m. L/hr x 8 hr = 864 m. L • 3 rd Space (4 m. L/kg/hr) = 272 m. L/hr • •

Example • Intra-operative Fluid Replacement of: – Fluid Deficit 864 m. L – Maintenance Fluid 108 m. L/hr – 3 rd Space Loss 272 m. L/hr – Ongoing blood loss (crystalloid vs. colloid)

How much fluid does he need? • Weight for maintenance 30 -35 ml/kg/24 hrs • History, fasting, losses, sepsis, fluid balance charts • Clinical status, current losses, fluid intake, urine output • Electrolytes, Hb (may be raised in dehydration)

Shock • Circulatory failure leading to inadequate perfusion and delivery of oxygen to vital organs • Blood Pressure is often used as an indirect estimator of tissue perfusion • Oxygen delivery is an interaction of Cardiac Output, Blood Volume, Systemic Vascular Resistance

Preload Contractility Afterload HR CO SV DO 2 Hgb Pa. O 2 Sat % Ca. O 2

Types of Shock • Hypovolemic – most common • Hemorrhagic, occult fluid loss • Cardiogenic • Ischemia, arrhythmia, valvular, myocardial depression • Distributive • Anaphylaxis, sepsis, neurogenic • Obstructive • Tension pneumo, pericardial tamponade, PE

Types of Shock • Hypovolemic – most common • Hemorrhagic, occult fluid loss • Cardiogenic • Ischemia, arrhythmia, valvular, myocardial depression • Distributive • Anaphylaxis, sepsis, neurogenic • Obstructive • Tension pneumo, pericardial tamponade, PE

Shock States BP Hypovolemia Cardiogenic LV - RV Distributive Obstructive CVP PCWP CO SVR
 Burns")
Hypovolemic Shock • • Most common Trauma Blood Loss Occult fluid loss (GI) Burns Pancreatitis Sepsis (distributive, relative hypovolemia)

Assessment of Stages of Shock % Blood Volume loss < 15% 15 – 30% 30 – 40% >40% HR <100 >120 >140 SBP N N, DBP, postural drop Pulse Pressure N or Cap Refill < 3 sec >3 sec or absent Resp 14 - 20 20 - 30 30 - 40 >35 CNS anxious v. anxious confused lethargic

Fluid Resuscitation of Shock • Crystalloid Solutions – Normal saline – Ringers Lactate solution – Plasmalyte • Colloid Solutions – Voluven – Emagel – Blood products (albumin, RBC, plasma)

Crystalloids • Na+ main osmotically active particle • Useful for volume expansion (mainly interstitial space) • For maintenance infusion • Correction of electrolyte abnormality

Crystalloids • Isotonic crystalloids - Lactated Ringer’s, 0. 9% Na. Cl - 25% remain intravascularly • Hypertonic saline solutions - 3% Na. Cl • Hypotonic solutions - D 5 W, 0. 45% Na. Cl - < 10% remain intravascularly, inadequate for fluid resuscitation

Colloids vs Crystalloids

Crystalloid Solutions • • • Normal Saline Lactated Ringers Solution Plasmalyte Require 3: 1 replacement of volume loss e. g. estimate 1 L blood loss, require 3 L of crystalloid to replace volume

Colloid Solutions • • Contain high molecular weight substances do not readily migrate across capillary walls Preparations - Albumin: 5%, 25% - Hydoxyethyl starches ie Voluven - Dextrans - Gelatins - Fresh Frozen Plasma

The colloids are mainly in the intravascular compartment for a period lasting more than crystalloids

Fluids and Cardiac Index
 pressure ∆plasma volume infused Duration Albumina 25%")
What colloid? Fluids Average molecular Oncotic weight(kilodaltons) pressure ∆plasma volume infused Duration Albumina 25% 69 70 4. 0 -5. 0 16 hr Destrano 40 10% 26 40 1. 0 -1. 5 6 hr Hetastarch 6% 450 30 1. 0 -1. 3 10 hr Voluven 130 36 1. 0 6 hr Emagel 35 30 0. 7 -0. 8 1 -3 hr

Albumin MW 69, 000 Da Main protein "transport" in the blood Responsible for 75% of the COP Can act as a "buffer" Can inhibit the aggregation PTLs and factor Xa by ATIII • Solutions at 5% and 25% • • •

Disputes on the use of albumin • Cochrane Injuries Group Albumin Reviewers. Human albumin administration in critically ill patients: systematic review of randomized, controlled trials. Br. Med. J. 1998; 317: 235 -240. • Choi PT, Yip G, Quinonez LG et al. Cristalloids vs. Colloids in fluid resuscitation: a systematic review. Crit Care Med. 1999; 27: 200 -210. • Wilkes MN, Navickis RJ. Patient survival after human albumin administration: a meta-analysis of randomized, controlled trials. Ann Intern Med. 2001; 135: 149 -164. • SAFE Study Investigators. A comparison of albumin and saline for fluid resuscitation in the intensive care unit. N Engl J Med 2004; 350: 2247 -2256. • Vincent JL, Navickis RJ, Wilkes MM. Morbidity in hospedalized patients receiving human serum albumin: a meta-analysis of randomized, controlled trials. Crit Care Med. 2004; 32: 2029 -2038.
 •")
Dextrans • Polydisperse polymers of glucose (10% dextran 40 and 6% dextran 70) • High power oncotic (directly proportional to the size) • Remain in the vascular compartment in a variable depending on the size • Elimination almost exclusively via the kidneys • Also used to reduce blood viscosity
 • Renal dysfunction")
Adverse effects of Dextrans • Anaphylactic reactions (> Gelatin and HES) • Renal dysfunction or IRA • Interference with Coagulation

Gelatins • MW 5000 -50000 • Are polydisperse polypeptides derived from the degradation of bovine collagen • Increase in the volume less than the amount infused because they go into the interstitial space and are rapidly eliminated by the kidney • Not accumulate in the blood • Can alter the haemostasis • Do not affect renal function
 • Urea-cross-linked gelatin (Haemacel) • Modified fluid gelatins")
Gelatins • Cross-linked or ossipoligelatin (Gelofundiol) • Urea-cross-linked gelatin (Haemacel) • Modified fluid gelatins or succinilate(Gelofusin)
 • Colloids synthesis of derivatives from amylopectin (Corn or potato) •")
Hydroxyethyl starch (HES) • Colloids synthesis of derivatives from amylopectin (Corn or potato) • The natural starches are unstable and rapidly hydrolyzed; the replacement of the hydroxyl group with a hydroxyethyl group in position C 2 C 3 -C 6 increases its solubility and retards the hydrolysis • Good ability to expand the plasma volume • High capacity to bind water (20 -30 ml / g)
 EFFECTS ON THE CIRCLE • Increases the intravascular volume • Improves")
Hydroxyethyl starch (HES) EFFECTS ON THE CIRCLE • Increases the intravascular volume • Improves the flow in the microcirculation • Reduces blood viscosity and therefore the Vascular resistances • Appears to reduce capillary permeability due to inflammation (Seal the leakage) EFFECTS ON RENAL FUNCTION • Recent studies show that patients treated with HES may have renal dysfunction • Some histological studies of transplanted kidneys showed tubular alterations but do not give any symptoms to the recipient (urinary hyperviscosity) • Adequate hydration with crystalloid prevent these adverse effects on renal function
 EFFECTS ON STORAGE COAGULATION • Possible negative effects • Itching for")
Hydroxyethyl starch (HES) EFFECTS ON STORAGE COAGULATION • Possible negative effects • Itching for accumulation in that vary with the type of the peripheral nerves even HES: those of "first after a month generation" have effects • Predominantly affects the more severe hydroxyethyl starch "first • Mechanism of action is not generation" entirely clear: possible inhibition of factor VIIIc and v. WF and platelet function

Is hydroxyethyl starch safe for the kidney? • Association of hydroxyethyl starch administration with mortality and acute kidney injury in critically ill patients requiring volume resuscitation: a systematic review and meta-analysis. Zarychanski R, Abou-Setta AM, Turgeon AF, Houston BL, Mc. Intyre L, Marshall JC, Fergusson DA. JAMA. 2013 Feb 20; 309(7): 678 -88 • Hydroxyethyl starch or saline for fluid resuscitation in intensive care. Myburgh JA, Finfer S, Bellomo R, Billot L, Cass A, Gattas D, Glass P, Lipman J, Liu B, Mc. Arthur C, Mc. Guinness S, Rajbhandari D, Taylor CB, Webb SA; CHEST Investigators; Australian and New Zealand Intensive Care Society Clinical Trials Group. N Engl J Med. 2012 Nov 15; 367(20): 1901 -11.

All colloids exert a negative effect on haemostasis! • Dilution effect • Specific action on coagulation factors and platelets De Jonge E. , Levi M. Effects of different plasma substitutes on blood coagulation: a comparative review. Crit. Care Med. 2001; 29: 1261 -7.

Colloid Solutions • • • Voluven Emagel Albumin 5% Fresh Frozen Plasma Replacement of lost volume in 1: 1 ratio

Eternal war between Colloids and Crystalloids!!

There is no ideal Fluid resuscitation! • Colloids versus crystalloids for fluid resuscitation in critically ill patients. Perel P, Roberts I, Ker K. Cochrane Database Syst Rev. 2013 Feb 28; 2: CD 000567.

Preload Contractility Afterload HR CO SV DO 2 Hgb Pa. O 2 Sat % Ca. O 2
 • Replacement")
Oxygen Carrying Capacity • Only RBC contribute to oxygen carrying capacity (hemoglobin) • Replacement with all other solutions will – support volume – Improve end organ perfusion – Will NOT provide additional oxygen carrying capacity

RBC Transfusion • BC Red Cell Transfusion Guidelines recommend transfusion only to keep Hgb >70 g/d. L unless – Comorbid disease necessitating higher transfusion trigger (CAD, pulmonary disease, sepsis) – Hemodynamic instability despite adequate fluid resuscitation

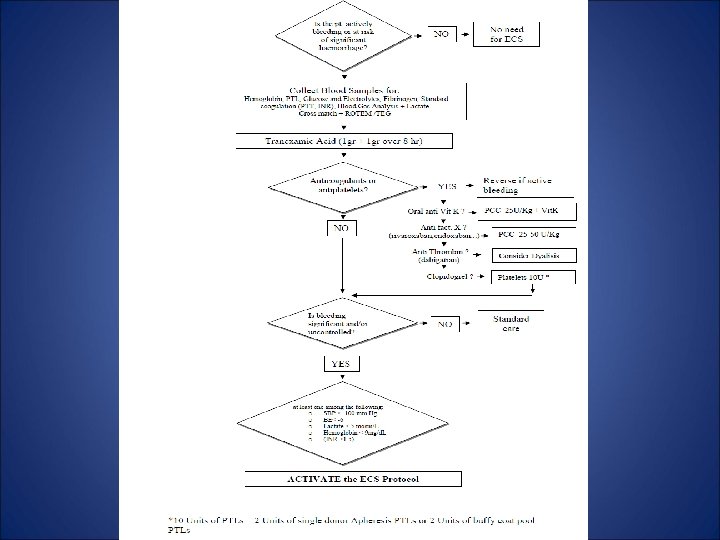
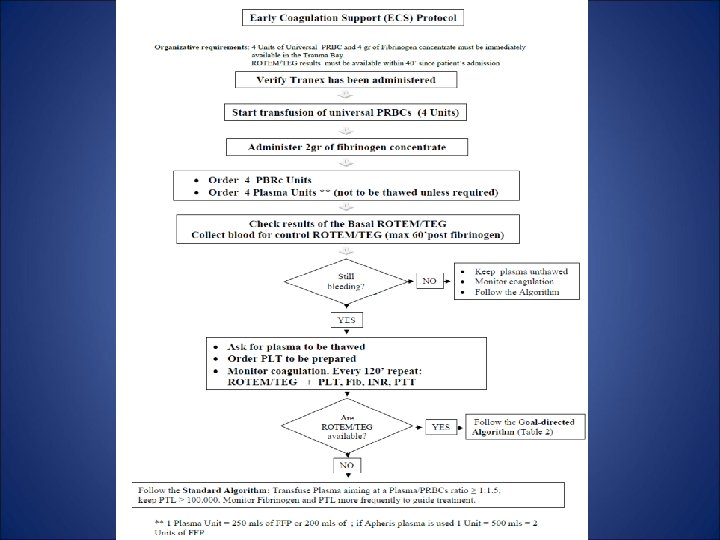
Fluid therapy and haemostasis Centro per lo Shock e il Trauma, Azienda Ospedaliera S. Camillo-Forlanini; Roma - Italy

Goals of Fluid Resuscitation • Easily measured – Mentation – Blood Pressure – Heart Rate – Jugular Venous Pressure – Urine Output

Goals of Fluid Resuscitation • A little less easily measured – Central Venous Pressure (CVP) – Left Atrial Pressure – Central Venous Oxygen Saturation SCVO 2

Mixed Venous Oxygenation • Used as a surrogate marker of end organ perfusion and oxygen delivery • Should be interpreted in context of other clinical information • True mixed venous is drawn from the pulmonary artery (mixing of venous blood from upper and lower body) • Often sample will be drawn from central venous catheter (superior vena cava, R atrium)

Mixed Venous Oxygenation • Normal oxygen saturation of venous blood 68% – 77% • Low SCVO 2 – Tissues are extracting far more oxygen than usual, reflecting sub-optimal tissue perfusion (and oxygenation) • Following trends of SCVO 2 to guide resuscitation (fluids, RBC, inotropes, vasopressors)

Goals of Fluid Resuscitation • A bit more of a pain to measure – Pulmonary Capillary Wedge Pressure (PCWP) – Systemic Vascular Resistance (SVR) – Cardiac Output / Cardiac Index

Pinsky MR, Payen D. Functional hemodynamic monitoring. Crit Care 2005; 9: 566 -572

The End GRAZIE PER L’ATTENZIONE !!!
- Slides: 92