Fixing A Broken Heart DEPARTMENT OF INTERNAL MEDICINE

Fixing A Broken Heart!

DEPARTMENT OF INTERNAL MEDICINE MEDICAL GRANDROUNDS RANIER T. TANALGO M. D. PRESENTER RUTH DIVINAGRACIA M. D. MODERATOR 9 TH FLOOR-LEDESMA HALL MARCH 17, 2011

OBJECTIVES: 1. To present a case of 71 yo patient who had difficulty of breathing after diving. 2. To present a case of a patient presented with NSTEMI with normal coronary angiographic findings.
 Panicked/ anxiety")
History of Present Illness: 1 Day PTA Deep sea diving (70 feet) Panicked/ anxiety attack Difficulty of breathing (+) chest tightness, (+) nausea, (+) dizziness, (-) epigastric pain, (-) nausea, (-) vomiting ADMISSION

Review of Systems: No history of headaches, dizziness No cough, fever, chest pain No weight loss, edema No abdominal pains, no urinary and bowel movement changes, no joint pains, no pruritus, no numbness No sensorial changes, behavioral changes, visual changes, seizures, focal weekness, easy fatigability, no hearing loss
 Hypothyroid and maintained on unrecalled medication (+) Depression treated since")
Past Medical history: (+) Hypothyroid and maintained on unrecalled medication (+) Depression treated since the 1980’s (+) Vaginal hysterectomy (+) Shingles in 2004 (+) Bilateral bunionectomy (+) Sclerotherapy for varicose veins of the lower extremities (+) Allergic to Penicillins- itchiness (-) Hypertension (-) Diabetes mellitus (-) Bronchial asthma.
 Hypertension (+) Coronary Artery Disease (+) Dyslipidemia (+) Thyroid disease r.")
Family History: (+) Hypertension (+) Coronary Artery Disease (+) Dyslipidemia (+) Thyroid disease r. Both parents sides

Personal/Social history: Non-smoker Occasional alcoholic beverage drinker

Physical Examination: Conscious, coherent, oriented, not in distress: BP=106/72 mm. Hg HR=82 bpm RR=20 cpm Temp=37 C O 2 Sat 93% at 4 LPM nasal cannula Ht: 167. 64 cm Wt: 68 kgs BMI: 24. 19 kg/M 2

Physical Examination: Skin: warm, good turgor, no pallor, no cyanosis, no skin color changes HEENT: anicteric sclera, pinkish palpebral conjunctivae, no naso-aural discharges, no tonsilopharyngeal congestion, Neck: no neck vein distention, JVP=5 -6 cm, no lymphadenopathy, non-palpable thyroid gland, no carotid bruit

Physical Examination: Chest and Lungs: no retractions, symmetrical chest expansion, mid to base bilateral coarse rales, no wheezing Heart: normal rate, regular rhythm, apex beat at 5 th ICS LMCL, S 1>S 2 at apex, S 2>S 1 at base, no S 3, no heave, no thrill, no murmur

Physical Examination: Abdomen: flat, normoactive bowel sounds, soft, nontender, no organomegaly, no masses Extremities: no edema, left leg noted slightly bigger than right leg (reportedly fell 3 weeks ago and injured left knee)

Salient features Subjective Findings 71/Female Difficulty of breathing after diving Elevate d Trop I Pulmonary edema on CXR Bilateral crackles from mid to base Objective findings Bilateral crackles from mid to base Normal vital signs

Differential Diagnosis Patient 71/Female Difficulty of breathing after diving Elevate d Trop I Pulmonary edema on CXR Bilateral crackles from mid to base Non ST Elevation Myocardial Infarction • Chest pain described as a pressure sensation, fullness, or squeezing in the midportion of the thorax • Radiation of chest pain into the jaw or teeth, shoulder, arm, and/or back • Associated dyspnea or shortness of breath • Associated epigastric discomfort with or without nausea and vomiting • Associated diaphoresis or sweating • Syncope or near syncope without other cause • Impairment of cognitive function without other cause

Differential Diagnosis Patient 71/Female Difficulty of breathing after diving Elevate d Trop I Pulmonary edema on CXR Bilateral crackles from mid to base ECG: Non specific ST wave chenges Decompression sickness Extreme Fatigue, Pain in Joints, Muscle Pain, Dizziness, Paralysis, Rash on Skin, Staggering, Choking. Decreased Sensation, Collapse or Unconsciousness P wave peaking and P-R depression compatible with right heart strain; S-T segment and T wave changes suggestive of myocardial ischemia; and ventricular arrhythmias ranging from unifocal premature ventricular contractions to ventricular tachycardia

Differential Diagnosis Patient Acute Pulmonary Embolism Most common symptom is 71/Female Difficulty of breathing after diving unexplained shortness of breath and/or chest pain with difficulty Elevate d Trop I breathing Pulmonary edema on CXR Chest pain, often worse when taking a Bilateral crackles from mid to base breath A feeling of apprehension Sudden collapse Coughing Sweating Non-specific ST changes Tachycardia

Admitting Impression: Acute pulmonary edema probably secondary to Acute Coronary Syndrome-Non ST elevation Myocardial Infarction Rule out Decompression Sickness Rule out Acute Pulmonary Embolism

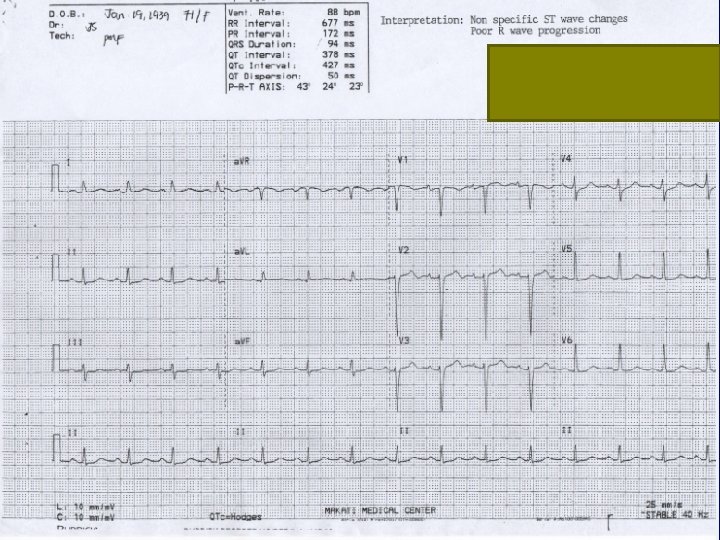
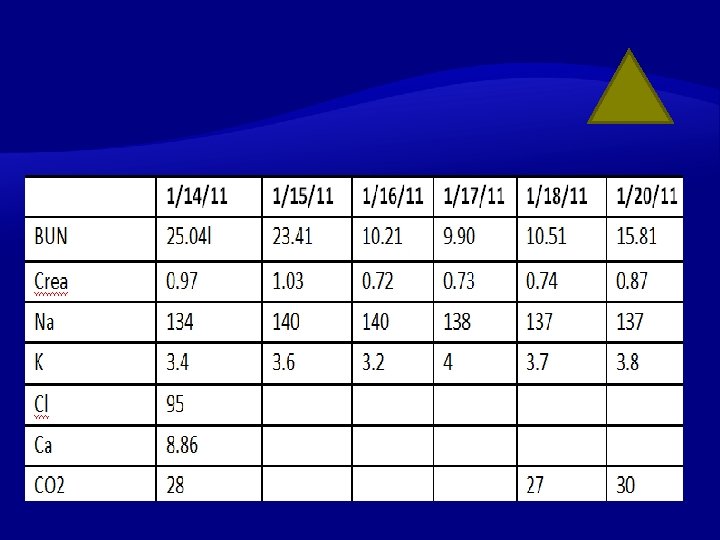
At the ER Patient started on MI protocol (Enoxaparin, ASA, Clopidogrel, Bromazepam and Lactulose, Furosemide, and Rosuvastatin ECG showed non-specific ST-T wave changes, poor R wave progression Electrolytes

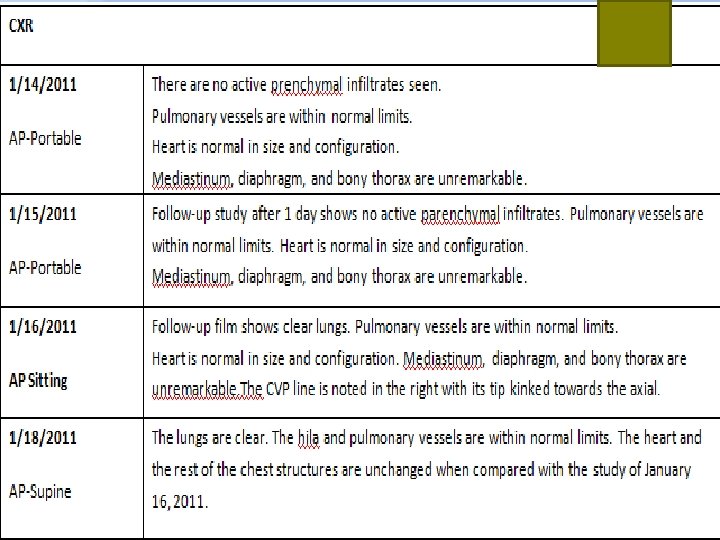
At the ER CXR: There are no active parenchymal infiltrates seen. Pulmonary vessels are within normal limits. Heart is normal in size and configuration. Mediastinum, diaphragm, and bony thorax are unremarkable. ABG: Respiratory alkalosis

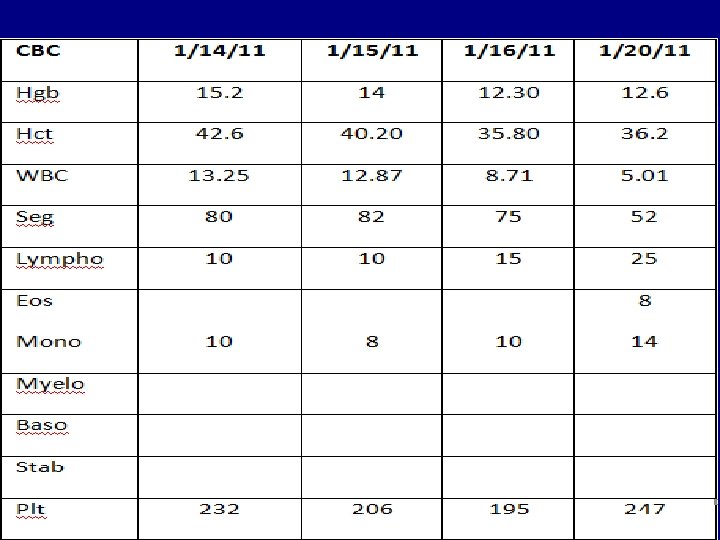
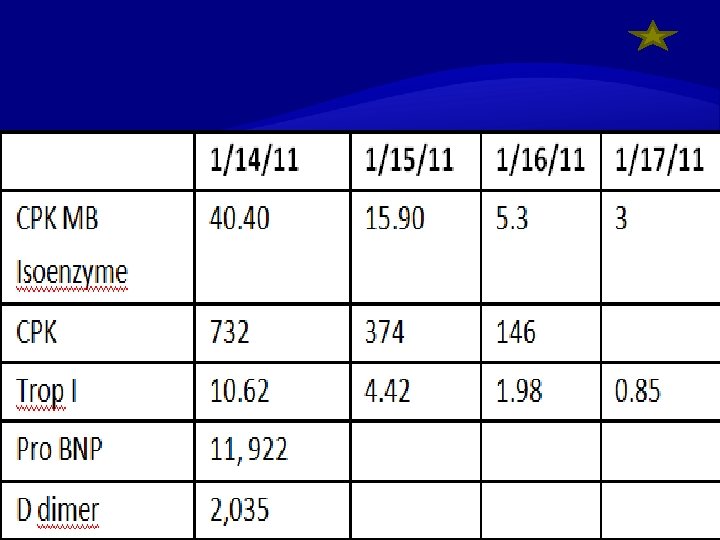
At the ER Cardiac enzymes were elevated (Trop I 10. 62 ng/ml, CPK 732 U/L and CPK MB isoenzyme 40. 40 ng/ml). Pro BNP and D dimer were elevated Protime was normal CBC showed leukocytosis (WBC 13. 25) with predominance of segmenters(80) and monocytes(10)

At the ER 2 D echo revealed dilated left ventricular dimensions with left ventricular global hypokinesia; LVEF of 36% by Teicholz and 35% by Simpson’s. MR, mild. TR, mild.

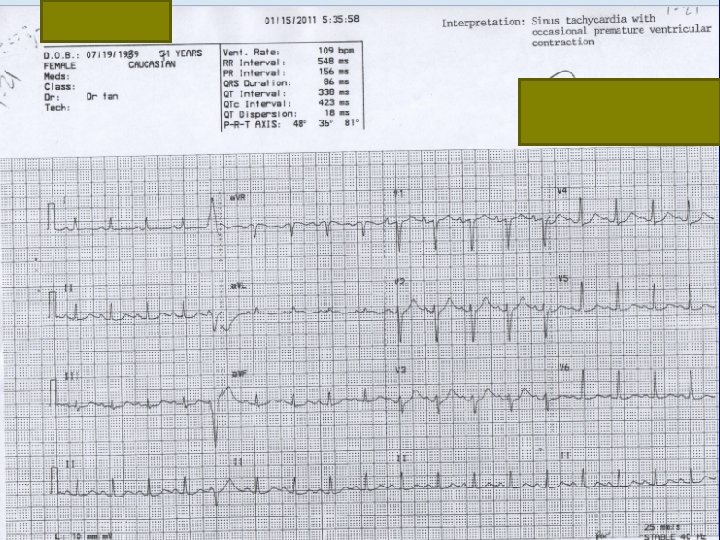
Medical Intensive Care Unit Second Hopsital Day Repet ECG: Sinus tachycardia with occasional premature ventricular contraction Patient had hypotension Inotropes started with Dopamine and Dobutamine Patient was scheduled for stat left heart catheterization with coronary angiography on double set up for possible angioplasty and CABG

Medical Intensive Care Unit Second Hopsital Day Repeat cardiac enzymes: Trop I 4. 42, CPK 374, CPK MB isoenzyme 15. 90 Electrolytes

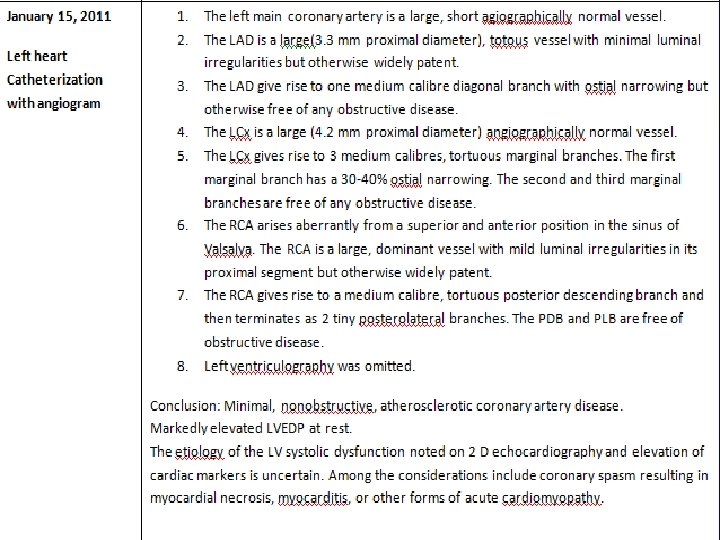
Medical Intensive Care Unit Second Hopsital Day Left heart catheterization with coronary angiography: Conclusion: Minimal, nonobstructive, atherosclerotic coronary artery disease. Markedly elevated LVEDP at rest. The etiology of the LV systolic dysfunction noted on 2 D echocardiography and elevation of cardiac markers is uncertain.

Medical Intensive Care Unit Fourth Hopsital Day Repeat 2 D echo: NLVD with hypokinesia of the anterior interventricular septum and anterior and lateral LV wall from base to apex. LVEF 54% by Teicholz and 54% by Simpson’s. Normal left and right atria. Normal right ventricle. Normal main pulmonary artery and aortic root dimensions. Calcification on aortic walls. Mitral and aortic annular calcification.

Medical Intensive Care Unit Fourth Hopsital Day Repeat 2 D echo: Color flow and Doppler study: MR, trivial. TR, trivial. Calculated pulmonary artery pressure by TR jet 40 mm. Hg. Pulmonary hypertension, mild. Compared with previous study done Jan. 15, 201103 -10 Left ventricular end diastolic diameter decrease from 5. 4 cm to 4. 7 cm. Ejection fraction has increase from 36% to 54%.

Medical Intensive Care Unit Fourth Hopsital Day Venous dupplez scan of lower extremities: Normal Carotid doppler: Normal

Medical Intensive Care Unit Fifth Hopsital Day Patient was stable Transferred out to regular room Referred to cardiac rehab Discaharged on the 8 th hospital day CXR

Follow up done at Mayo Clinic Follow after 1 month Trans esophangeal echocardiogram performed LV: normal LV chamber size. NLVSF. ELVEF, 65%. No regional wall motion abnormalities. NRVSF. No shunt at atria level by color flow imaging and agitated contrast injection

In Summary 71/F Sudden dyspnea after diving Non-specific ST changes Elevated cardiac enzymes 2 D echo with segmental wall hypokinesia with improvement after 4 days Normal Coronary angiogram

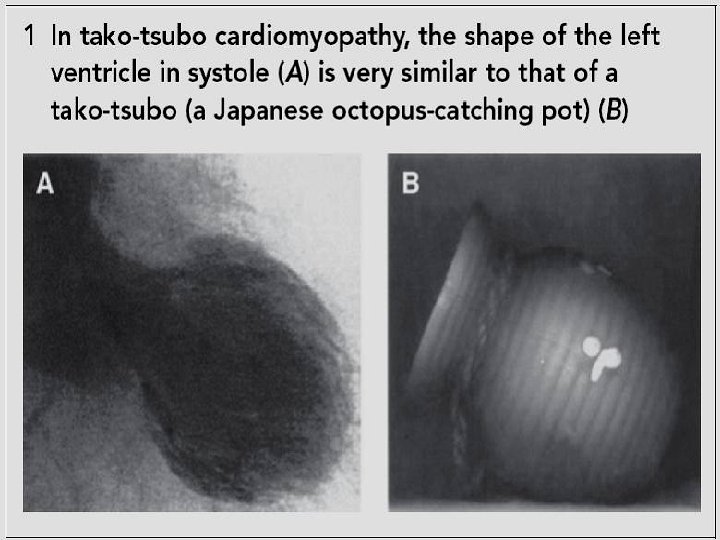
Final diagnosis Acute Cornary Syndrome- Non ST Elevation Myocardial Infarction complicated by pulmonary edema Tako-Tsubo cardiomyopathy
 Tako-Tsubo – Japanese name for octopus trap fisherman uses to catch")
Tako-Tsubo Cardiomyopathy (TTC) Tako-Tsubo – Japanese name for octopus trap fisherman uses to catch octopus. TTC – Heart (LV) Like the shape of an octopus trap

Broken Heart Syndrome Other names: Stress induced cardiomyopathy Transient LV apical balooning Apical balooning syndrome Tako-Tsubo Cardiomyopathy

An antique tako-tsubo.

Epidemiology Early 1990’s – 1 st reported in Japan by Sato et al Early 2000 – recognized in western white population, Africans, Americans, Asians High prevalence in Japan Women : men ratio (7: 1) Age 68. 6 + 12. 2 women 65. 9 + 9. 1 men Kinji Ishikawa, M. D.

Epidemiology TTC accounts for 2% of all patients presenting with CP and ST elevation. Gianni et al European Heart Journal 2006 27: 1523 -1529

Mayo Clinic criteria for tako-tsubo cardiomyopathy • Transient, reversible akinesis or dyskinesis of the left ventricular apical and mid-ventricular segments with regional wall motion abnormalities extending beyond a single vascular territory on left ventriculography. • Absence of obstructive coronary artery stenosis > 50% of the luminal diameter or angiographic evidence of acute plaque rupture. MJA • Volume 187 Number 6 • 17 September 2007

Mayo Clinic criteria for tako-tsubo cardiomyopathy • New electrocardiographic abnormalities consisting of ST- segment elevation or T-wave inversion. • Absence of: recent head trauma, intracranial bleeding, phaeochromocytoma, obstructive epicardial coronary artery disease, myocarditis, hypertrophic cardiomyopathy

Pathophysiology Exact mechanism unknown Evidences point to: Catecholamine mediated mechanism via cardiac sympathetic neurons which can be triggered by emotional or physical stress. Myocardial stunning form multiple site microvascular spasm
 More")
Pathophysiology Wall motion localized at the distal half of the LV (apical balooning) More dense adrenoreceptors at the apex.

Pathophysiology Stressors 65 – 80% - with identifiable stressors 50% - emotion 50% - physical 20 – 35% – non identified Irfran Abdulla, MD Clinical Update MJA vol 187 No. 6 – 17 Sept 07

Common physical, psychological and emotional stressors precipitating tako-tsubo cardiomyopathy • Unexpected death in the family • Gambling and financial losses • Devastating medical diagnosis • Car accidents • Public speaking • Earthquakes • Acute physical trauma • Robbery • Major surgical procedures MJA • Volume 187 Number 6 • 17 September
 silhouettes published in different articles under")
FIGURE 1. Different end-systolic left ventricular (LV) silhouettes published in different articles under the term “Takotsubo syndrome” (transient LV apical ballooning or broken heart syndrome). The tracing was done exactly over the shape of the angiograms from the articles (A, Abe et al 8; B, San Roman Sanchez et al 9; C, Wittstein et al 10; D, Rivera et al 3; E, Desmet et al 11; and F, Reyburn and Vaglio 4). As can be clearly seen, there is wide heterogeneity among the different patterns, varying from a relatively small akinetic apical area in C to a wide global akinesia in D and E. Mayo Clin Proc. • June 2006; 81(6): 732 -735 • www. mayoclinicproceedings. com

Usual Presentation Post menopausal – female Chest pain, dyspnea, hypotension 1 -5% hemodynamically unstable ECG – ST elevation in V 3 – V 6 or diffuse ST – T changes Troponin & CK-MB – no rise or min

Usual Presentation LV wall motion – apical balooning or dyskinesia and basal hyperkinesia during systole Coronary Angio – no significant CAD Precipitating factors – severe emotional or physical stress Serum nor epinephrine – significantly

Treatment Self – limiting disorder – Blocker ACE I Caution on patients With LVOT obstruction Avoid Inotropes Volume depletion Vasodilators

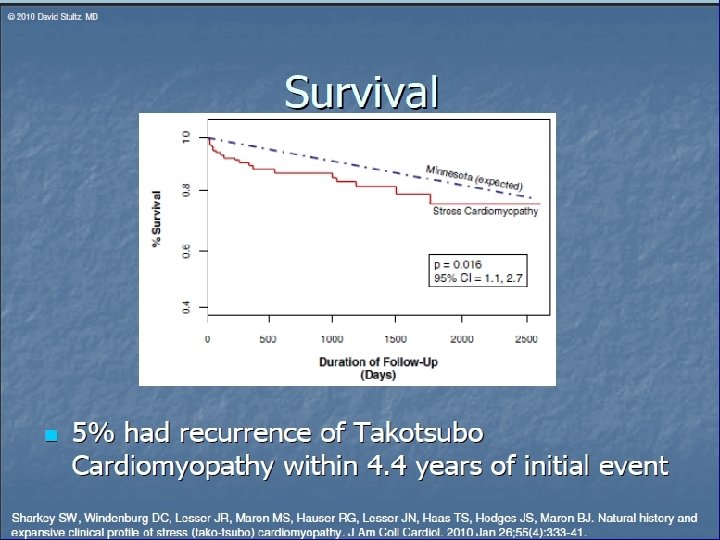
Prognosis Excellent despite Hemodynamic compromise in some patients Hospital mortality 0 – 8% LV systolic function (N) in 1 – 4 weeks Recurrent rate low 1 – 5% Long term Rx – unclear

Conclusions 1. Is a reversible cardiomyopathy triggered by psychologically stressful events. 2. Occurs in older women and may mimic evolving acute myocardial infarction or coronary syndrome.

Conclusions 3. Must be taken into consideration regardless the geographical area. 4. The complete explorations (echocardiography, angiography, MRI and myocardial scintigraphy) contribute to a better and more complete diagnosis and are important for evolution, consequences and ppropriate medical therapy.

Thank you very much

Jan. 18, 2011

ABG

ECG 1/14/2 Non specific ST wave changes. Poor R wave progression. 011 1154 H 1/15/2 Sinus tachycardia with occasional 011 premature ventricular 0535 H contraction
- Slides: 63