Five Years with the NEDSS Base System in

Five Years with the NEDSS Base System in South Carolina: Revolution, Evolution, and Future Perspectives Claire Youngblood, MA Division of Acute Disease Epidemiology South Carolina Department of Health and Environmental Control Columbia, SC

Or How We Learned to Stop Worrying and Love the NBS

Acknowledgements • • Eric Brenner, MD Jason Collins Dan Drociuck, MT Many hardworking DHEC people

• Revolution – Rollout to Regions – Rollout to Providers – Electronic Lab Reports • Evolution – A few numbers – CHESS outside the box • Future Perspectives – Upcoming projects – Where we want to go
")
Carolina’s Health Electronic Surveillance System South Carolina’s Implementation of CDC’s NEDSS Base System (NBS)

South Carolina’s CHESS Team • • • Physicians Nurses Epidemiologists Programmers Data Analysts Data Entry Trainers Healthcare Providers Laboratory Staff

Milestones • May 2003 – CHESS live in Central Office • November 2003 - CHESS Deployment Complete for All Health Districts • December 2004 – Last record entered in NETSS • July 2006 – First External Deployment • April 2007 – First Electronic Lab Report in CHESS
 • Contains lab data automatically transmitted from lab databases to")
Electronic Lab Reports (ELR) • Contains lab data automatically transmitted from lab databases to CHESS • Loaded at the end of each day • Contains no clinical information • Often received by DHEC before the ordering provider

Revolution

“This thing makes me cuss. ” -Anonymous Regional User

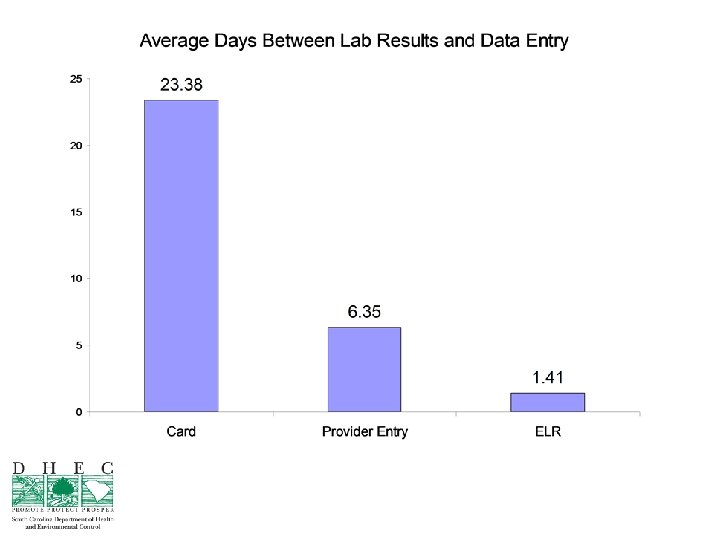
SC Disease Report Card

Why Give This Up? • • • Simple interface Portable Cheap Easy to edit No passwords Convenient in rural health departments

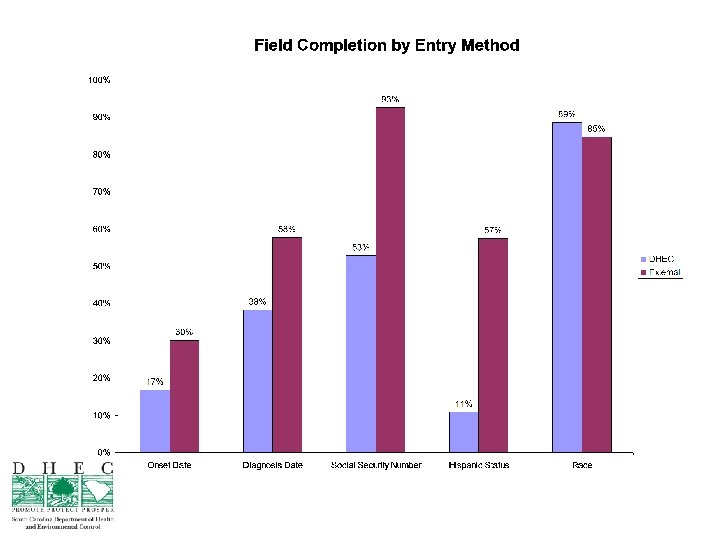
Revolution Rewards • Increased communication between regions and central office • Faster response • More complete data • Ability to follow patients over time • Closer connection to CDC case definition • Data entry from lots of sources

Revolution Costs • • • Data entry from lots of sources Changes in infrastructure Training needs Changes in interaction More hands-on computer work

Provider Deployment Challenges • • Site visits Fitting CHESS into each office Education: initial and ongoing Corporate policy Providing feedback Staff turnover “What’s in it for us? ”

ELR Challenges • Funding – Hospitals like the idea, but don’t want to spend the money • Getting vendors to meet the standard • Keeping LOINC/SNOMED codes updated • Auditing procedures to ensure that all reportable conditions are included • Complex reporting rules

Ongoing Process Challenges • • • Records without Jurisdiction Records without Program Area Disease specific process requests Legacy Data Ad-hoc reporting needs

Evolution

Users • • • 26 Users in Central Office 40 Regional Users 42 Provider Facilities 234 Provider Users 11 ELR Reporting Facilities NETSS: Data was entered by ONE user. CHESS: Data is entered by >350 users.

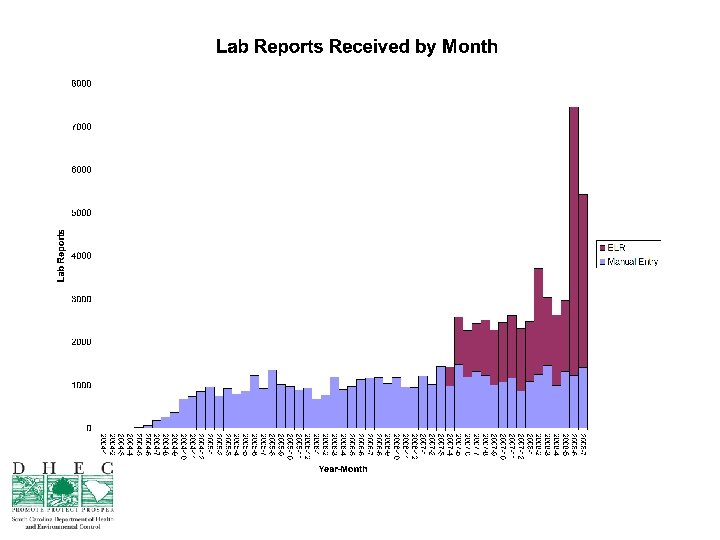
ELRs • Since April 2007, more than 33, 500 ELRs have been received • 16, 865 Total Investigations – 10, 990 (>65%) Investigations with Labs – 6, 423 (>38%) Investigations with ELR as first observation

CHESS Uses Beyond Notifications • Annual Report • Detailed Statistics for Vaccine Preventable Disease Grant • Enhanced Influenza Surveillance • Outbreak Details • Comorbidity Studies

CHESS Uses Beyond Notifications • • • Hospital Infections Disclosure Act EARS Analysis of CHESS Data Pass-through for STD/HIV Data Rabies Post Exposure Prophylaxis Tracking Email Notification Geographic analysis platform for disease tracking

Future Perspectives

2013? • Web or ELR reporting from all labs and providers. • Integration of all reportable diseases into a single system (TB, HIV/AIDS, STDs…) • Integration with outbreak management • Integration of case report forms • Integration with CDC case definitions • Contact tracing • Greater flexibility with fields. • GIS incorporated into the system
- Slides: 30