FIT BCSP and Colonoscopy Services S A Riley

FIT, BCSP and Colonoscopy Services S A Riley November 2019

Background • CRC one of commonest cancers – 40, 000 cases and 16, 000 deaths per year • 240, 000 referred 2 ww – only 4% CRC • Improving performance against 62 d target not improved stage at diagnosis • 20% patients presenting as emergency • Screening best means of detecting early cancer and is cost effective • Endoscopy services struggling 2 ww, STT, FIT in screening and lower risk

g. FOBt and FIT – why the switch?

Clinical Effectiveness of FIT • Systematic review of 10 European diagnostic cohort studies (no RCT) • Only one general practice study (Mowat Gut 2015) HM JACKarc n= 3 OC Sensor n= 5 • • True positive 3. 1% False positive 19. 8% True negative 76. 9% False negative 0. 2% • • True positive 2. 2% False positive 22. 9% True negative 74. 9% False negative 0% Approx 30% false positives have advanced adenomas or IBD

FIT use in different clinical settings Screening Symptomatic • 20 ug/g optimal • 10 ug/g as rule out test • 120 ug/g currently • But false negatives therefore safety net • May be reduced as endoscopic capacity increases
 FOBt to colonoscopy (uptake 62%. .")
SYB BCSP Activity (April 2018 – March 2019) FOBt to colonoscopy (uptake 62%. . . GP endorsement helpful) • Colonoscopies 1377 • 7. 5% cancers (64% early stage) • 52% adenomatous polyps ( 18% >1 cm) Bowel. Scope • Flexible sigmoidoscopy 5990 • 0. 05 % cancers • 8. 0% adenomatous polyps • 4. 0 % conversion to colonoscopy

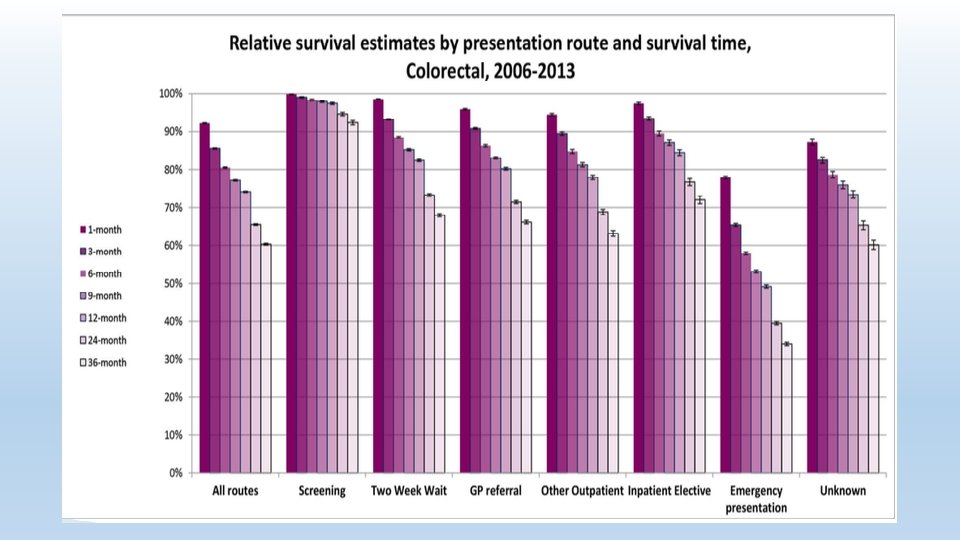
Impact of Introducing FIT in Screening

What About Colonic Polyps? • Most CRC develop from polyps and polypectomy reduces CRC • Metachronous lesions common hence surveillance with low, intermediate and high risk groups • Surveillance accounts for 15% of 1 M colonoscopies/year • But… polyps much more common that CRC • Increasingly believed that greatest benefit from initial colonoscopy • New national guidelines reduce intensity of surveillance

New Post Polypectomy Surveillance • Only one high risk group • 2 polyps including one advanced ( 10 mm, serrated with dysplasia or HGD) or • 5 polyps Recommendation • One off surveillance at 3 years

Post CRC Resection • 1 year clearance colonoscopy • Surveillance colonoscopy after 3 more years

Surveillance Exceptions No Surveillance • If life expectancy < 10 years • If age older than about 75 years If polyps and more than 10 years to lower screening age • Consider additional colonoscopy 5 -10 years

FIT : Take Home Messages Useful risk stratification tool • In screening • Increasing uptake • Potential to lower threshold • In low risk groups • Allows triage • Earlier diagnosis and stage shift for some • Fewer inappropriate invasive investigations for others • In high risk (2 ww) groups • Insufficient data yet
- Slides: 13