First National Conference on Patient Safety Patient safety








 “An unintended injury or complication that results in disability at the")

")






 Between 1998 and 2011, in the US, more than 500")









")













- Slides: 44
First National Conference on Patient Safety Patient safety as a new paradigm of clinical work WHO CO Ukraine Dnipro, 6 June 2017
Content • First and second victims • The dimension of adverse events • Origins of errors at individual, group and organization level • Strategies to reduce adverse events
First, second and third victims Lewis Kimberly “If physicians, nurses, pharmacists, and administrators are to succeed in reducing errors in hospital care, they will need to fundamentally change the way they think about errors and why they occur” (Leape, 1994)
Pectum excavatum: the condition and its surgical treatment
Plausible causes behind Lewis’ tragedy Postoperative care plan: • Wrong drug and pediatric dosing of NSAID (Toradol) • Ignoring low urine flow Anticipating problems: • A relatively new procedure that lasted almost 3 hours instead of expected 30’ = surgical stress • Handoffs to a oncology unit unfamiliar with surgical patients • Failure to consider the possibility of medication side effects (acute haemorrhagic gastritis, ulcer, perforation)
Monitoring of postoperative conditions: • Inability to make sense of signs/symptoms of acute abdomen, perforated gastric ulcer and shock • Missed key lab, imaging tests + endoscopy Response to changing conditions: • Unwillingness to change the plan • Prolonged inaction in the face of alarming symptoms • Undue deference to hierarchy • Unwillingness to intervene with someone else’s patient • Code called too late Inadequate training and backup, Overconfidence, Fixation error
Upright abdominal and chest X-rays and CT showing free air under the diaphragm and anterior to the liver (Parswa Ansari, Acute Abdominal Pain, Merck Manual )
Haemorrhagic Gastritis www. gastrolab. net
Adverse Event (AE) “An unintended injury or complication that results in disability at the time of discharge, death or prolonged hospital stay and that is caused by health care management rather than by the patient’s underlying disease process. ” (Baker GR, Norton PG, Flintoft V, Blais R, Brown A, Cox J et al. 2004).
Dimension of the problem: first victims Unsafe care is a major cause of morbidity and mortality: tens of millions of patients worldwide suffer disabling injuries or death every year due to unsafe medical practices and care. (WASP/WHO, 2008) Nearly one in ten patients is harmed while receiving health care in well-funded and technologically advanced hospital settings. Financial costs : 2% of global health spending.
(Jha & Bates, 2002)
Diagnostic errors 5 -15% in a variety of settings and across several clinical conditions (Pulmonary Embolism, Drug reactions, Lung and Colon ca, Infections, Fractures, Acute Myocardial Infarctions, Aneurisms). (WHO/WAPS, 2008)
Second and third victims When clinicians make a mistake, they are more likely to suffer depression or burnout. And depressed or burnedout physicians are more likely to make mistakes.
Paradox The great majority of professionals dedicate decades to education, are motivated and skilled to confront and solve complex clinical problems, however patients • often do not get services from which they could benefit, and • as a consequence of involontary and evitabile errors, suffer of adverse events much more frequently of what believed until recently.
Determinants of errors at individual level
Human fallibility “Human fallibility is like gravity, weather, and terrain-Just another foreseeable hazard. ” (Wildavsky, 1991) “. . the universal constant is that human infallibility is impossible and those who build a system that depends on an absence of serious human mistakes will fail utterly. ” (John Nance, 2008)
Remembering Man boards T train at North Quincy, leaving infant in car (Boston Globe, May 13, 2015) Vicenza – Italy, a 17 months old little girl dies because she is forgotten inside a car for three hours under the sun (La Repubblica, June 1, 2015)
Forgotten baby syndrome (FBS) Between 1998 and 2011, in the US, more than 500 children died from being left in the interior of hot cars, one every nine days (Barth, 2011) Far-fetched behaviors leading to FBS are frequent and widespread: • Nearly 1 in 4 parents of a child under 3 has forgotten the child in a car; • Dads are nearly three times more likely than moms to leave a child in a parked car. (Safe Kids Worldwide, 2014)
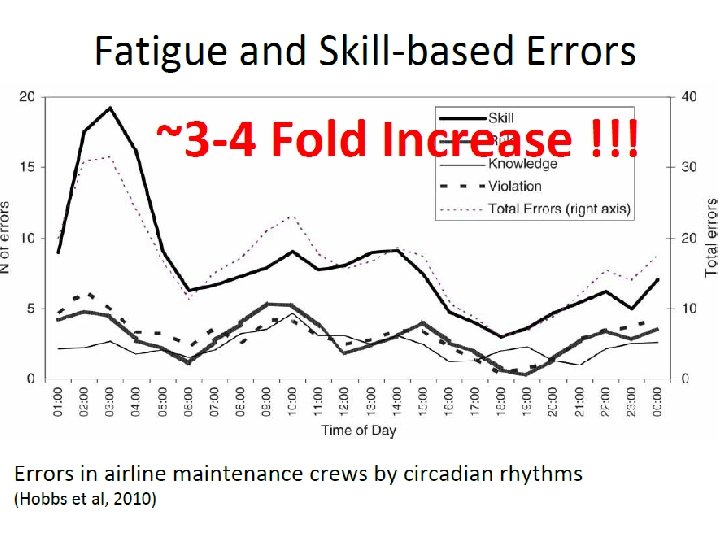
Sleep-deprivation
Multi-tasking
First Stories of Failure Saying what people should have done is a satisfying way to describe failure and assign responsibility. Telling people to be more careful will not make the problem go away. .
Always present when the outcome is known
Denial, blame, shame and retrain “…there is no place for mistakes in modern medicine. …an expectation of perfection. Hospitals react to every error as an anomaly, for which the solution is to ferret out and blame an individual, with a promise that “it will never happen again. ” (Wu, 2001)
The single greatest impediment to error prevention in the medical industry is “that we punish people for making mistakes. ” (Leape, Testimony, United States Congress, House Committee on Veterans' Affairs; 1997 Oct 12. )
Error reduction strategy: Checklists Reduce intent, vigilance and hard work, i. e. 10 -1 Performance
Error reduction strategy: Simulation. Practice tasks with immediate feedback by an expert in a low risk context
Determinants of errors at group level
Authority gradient Believe that decisions of the “leader” should not be questioned (Sexton, 2000)
Since human error is inevitable the only way to keep error from hurting patients is by creating heedful interactive teams whose members can catch and neutralize one another’s mistakes. ”
Error reduction strategy: Debriefing
Error reduction strategy: Respect “Disrespect is the heart of the slow progress in reducing medical errors. It is time for medical schools to teach respect and teamwork, and for leaders in medicine and the chief executives of hospitals to enforce codes of conduct to ensure that all parties treat one another with respect”. (Leape, 2011)
Determinants of errors at system level
“Our systems are too complex to expect merely extraordinary people to perform perfectly 100% of the time. We as leaders have a responsibility to put in place systems to support safe practice. ” (James Conway VP and COO Dana-Farber Cancer Institute, 1995)
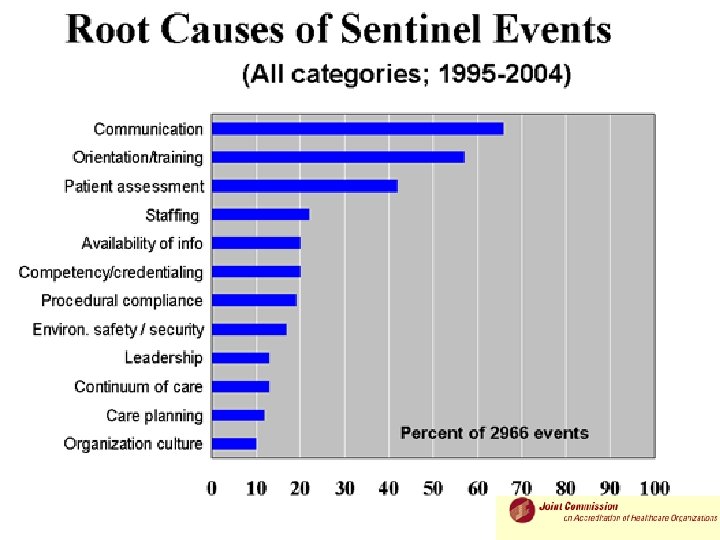
Compared with most other sectors, healthcare is • far more complex (e. g. many handoffs) • far less standardized • within a far more safety-critical environment • carried out with far less training • characterized by poor communication
Error reduction strategy: Systemic and Proactive Approach “…though we cannot change the human condition, we can change the conditions under which humans work. ” (Reason, 2000) “There is no way to change outcome except through changing process, since outcome ‘tells on’ process. ” (Slee, Slee & Schmidt. 1996)
Error reduction strategy: Culture of Safety • Acknowledgment of the high-risk nature of an hospital’s activities and the determination to achieve consistently safe operations • A blame-free environment where individuals are able to report errors or near misses without fear of reprimand or punishment • Encouragement of collaboration across ranks and disciplines to seek solutions to patient safety problems • Organizational commitment and resources to address safety concerns (AHRQ, 2014) 39
Error reduction strategy: Share stories of incidents and recovery Human beings, by their nature, learn from the experience of others. We must be willing to share our mistakes as well as our successes. Ask staff for suggestions to prevent the incident from reoccurring.
Move from Person to Systems view Person • Errors are the result of human failures Systems • Begin with the premise that anything can and will go wrong • Humans generally perform • Don’t expect humans to perform flawlessly perfectly • Perfect performance is the • Design systems accordingly in a expectation proactive way • Use retraining and • Collective preoccupation with punishment to root out possibility of failure “bad apples”
Conclusion While being concerned with quality for many years, healthcare did not, in general, think systematically about patient safety until the magnitude of the problem became very clear and could no longer be ignored. Now, after more than a decade of activity that has measured, tracked, and in many instances investigated adverse events in acute care, no one doubts that enhancing patient safety is an important and necessary goal
Thank You!