FILARIASIS Dr Mohit Bhatia Assistant Professor Department of

FILARIASIS Dr. Mohit Bhatia Assistant Professor Department of Microbiology AIIMS, Rishikesh

Learning objectives • Somatic nematodes • Difference between various filarial nematodes • Lymphatic Filariasis • Loiasis • Onchocerciasis

SOMATIC NEMATODES

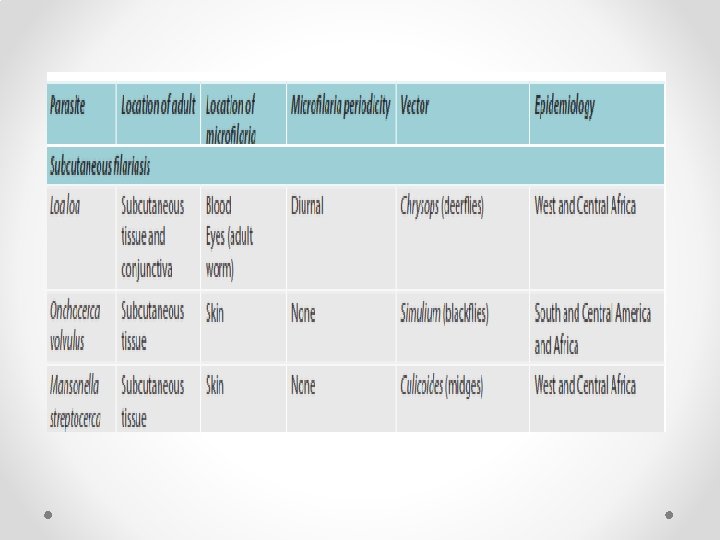
Differences between various filarial nematodes

Periodicity of Filarial nematodes

VECTORS AEDES ANOPHELES CULEX SIMULIUM CHRYSOPS

WUCHERERIA BANCROFTI Epidemiology • Southeast Asia accounts for highest burden; comprises of 50% of globally infected lymphatic Filariasis (LF) cases. • India – It is estimated that about 650 million people are at risk, residing in 256 districts of 21 states in India; accounting for 40% of global burden. • Highly endemic states are Uttar Pradesh, Jharkhand, Bihar and West Bengal, which account for two-thirds of the lymphatic Filariasis burden in India

Morphology-Adult worm • Long, slender, creamy-white thread like, filariform shaped with tapering ends. • Females are viviparous and they directly discharge larvae without any eggs.

Morphology-Larva • First stage larva is called as microfilaria. • The third stage larva is called as filariform larva; which is the infective form to humans.

Morphology-Larva • Microfilariae are the diagnostic forms, found in the blood vessels. • The nuclei are present throughout the body except near the head and the tail end. • Nuclei are also absent in few places which represent various primordial organs like nerve ring, excretory pore, anal pore and genital cells

Comparison of microfilariae of various filarial worms

Comparison of microfilariae of various filarial worms

Cultivation • Cell line: W. bancrofti and B. malayi can be cultivated in mosquito cell line (like Aedes togoi and Anopheles maculatus) grown in modified RPMI-1640 medium or medium-TC 199 supplemented with 20% newborn calf serum and LLC-MK 2 cells.

Life Cycle Host: W. bancrofti completes its life cycle in two hosts. • Definitive host: Man is the definitive host and also the only reservoir host. • Intermediate host: Mosquito named Culex quinquefasciatus is the principle vector worldwide. • Infective form: Third stage filariform larvae • Mode of transmission: Filariform larvae get deposited in skin by the mosquito bite.

Life cycle

Pathogenesis and pathology • Tissue alterations related to migration of live adult worms such as lymphatic dilatation and thickening of the vessel walls • Tissue alterations related to antigen and toxic metabolites released from dead adult worm • Secondary bacterial and fungal infections • Host’s inflammatory response to both live and dead parasite

Host Immune Response • Both cellular and humoral immune response are altered. • Antigens of both adult worms and microfilariae are processed by the antigen presenting cells (macrophages) and presented to T helper cells (TH cells). • TH cells are stimulated and differentiated into TH 1 cells and or TH 2 cells.

Clinical Features • Incubation period is about 8– 16 months. • Clinical manifestations can be categorized into: o Lymphatic Filariasis o Tropical pulmonary eosinophilia (TPE)/(Occult Filariasis) o Immune complex mediated manifestations.

Lymphatic Filariasis • Endemic normal -normal people residing in endemic area. • Asymptomatic microfilaremia – o o Microfilaremia demonstrated in their peripheral blood Microscopic hematuria and/or proteinuria Dilated and tortuous lymphatics (visualized by imaging) Filarial dance sign (ultrasound showing motile adult worm in scrotal lymphatics).
 Acute Filariasis (acute adenolymphangitis) - Recurrent episodes of: •")
Lymphatic Filariasis (cont. . ) Acute Filariasis (acute adenolymphangitis) - Recurrent episodes of: • Filarial fever (high-grade fever) • Lymphatic inflammation (lymphangitis and lymphadenitis): Lower extremities are more commonly affected than the upper limbs • Transient local edema • Dermatolymphangitis
 Chronic Filariasis: • Severe lymphatic obstruction and pedal edema")
Lymphatic Filariasis (cont. . ) Chronic Filariasis: • Severe lymphatic obstruction and pedal edema • Hydrocele • Elephantiasis • Chronic funiculitis and epididymitis Elephantiasis • Chyluria Hydrocele

Differences between classical & occult Filariasis

Laboratory Diagnosis
 (B) Thick blood smears stained with Giemsa showing microfilaria of (A)")
Laboratory Diagnosis (A) (B) Thick blood smears stained with Giemsa showing microfilaria of (A) Wuchereria bancrofti; (B) Brugia species

Treatment • DEC • DOXYCYCLINE • Albendazole • MANAGEMENT OF LYMPHEDEMA
 • Global programme to eliminate lymphatic Filariasis (LF) is")
Elimination of Lymphatic Filariasis (ELF) • Global programme to eliminate lymphatic Filariasis (LF) is launched by WHO in 2000 aiming at global elimination by the year 2020. • Strategy: WHO recommends yearly single dose of DEC + albendazole in all endemic areas except o In oncocerciasis endemic areas where ivermectin+ albendazole is given. o In Loa loa endemic area (albendazole twice per year given) o Recently in 2018, WHO recommended IDA regimen (combination of ivermectin, DEC and albendazole) under elimination program. It is yet to be implemented.

ELF in India • In India, ELF is in operation since 2004 in parallel with global strategy. • Twin Strategies employed: Comprises of (1) annual mass drug administration (MDA) of DEC + Albendazole; (2) Home based management for lymphedema cases and up scaling of hydrocele operations. • Dosage: DEC is given at dose of 100 mg for 2 -5 years, 200 mg 6 -14 years and 300 mg for ≥ 15 years age and albendazole is given 400 mg for all age group >2 years. • Indication: MDA is indicated in all high risk population of 256 endemic districts of India; except in children <2 years, pregnant women and severely ill. • Duration: MDA should be continued annually for minimum five years; with a target of >65% coverage of at risk population.

ELF • Filariasis elimination: After four years of post MDA surveillance, the area is declared as having achieved elimination status. • Elimination status: As of 2018, five states (Assam, Tamil Nadu, Goa, Puducherry, Daman & Diu) stopped MDA after achieving elimination status and observing post MDA surveillance activities.

BRUGIA MALAYI Epidemiology • There is considerable overlapping in the geographical distribution of Brugian Filariasis and Bancroftian Filariasis. • B. malayi occurs primarily in eastern India, Indonesia, Malaysia, Thailand Philippines

Morphology-Adult worm • The adult worms are essentially similar to that of W. bancrofti except they are smaller in size; males (3. 5 cm × 0. 1 mm) and females (5– 6 cm × 0. 1 mm).

Morphology-Microfilariae

Clinical Features • Both lymphatic Filariasis and tropical pulmonary eosinophilia syndrome are observed in Brugian Filariasis. • Clinical features are similar to Bancroftian Filariasis except: o o o More frequent episodes of acute adenolymphangitis, adenitis (femoral nodes), and filarial abscesses Chronic manifestations (lymphedema and elephantiasis) occur less frequently The genital involvement is not seen Elephantiasis: Swelling is limited to leg below the knee Chyluria does not occur.

Laboratory Diagnosis As in Bancroftian Filariasis, the diagnosis of Brugian Filariasis depends on: • Microscopy: Microfilaria in blood can be detected by Giemsa stained peripheral blood smear examination. • Antibody detection methods: ICT (Brugia Rapid) is available detecting parasite-specific Ig. G-4 antibodies • Molecular methods

TREATMENT AND PREVENTION • Treatment for Brugian Filariasis is same as for Bancroftian Filariasis except that frequency of adverse effects following DEC medication is more; therapy should be started with lower dose. • Prevention- Same as for Bancroftian Filariasis (i. e both chemoprophylaxis and vector control).

LOA Morphology • Adult worms (females, 50– 70 mm long and 0. 5 mm wide; males, 30 – 35 mm long and 0. 3 mm wide) • Live in subcutaneous tissues • Microfilariae circulate in the blood with a diurnal periodicity Loa loa microfilaria

Life Cycle • Life cycle is similar to that of W. bancrofti except the vector is female Chrysops species (deer flies, mango flies, red flies or tabanid flies) • Mode of transmission infective (L 3 ) larvae are transmitted by the bite of female Chrysops species during the blood meals in the daytime

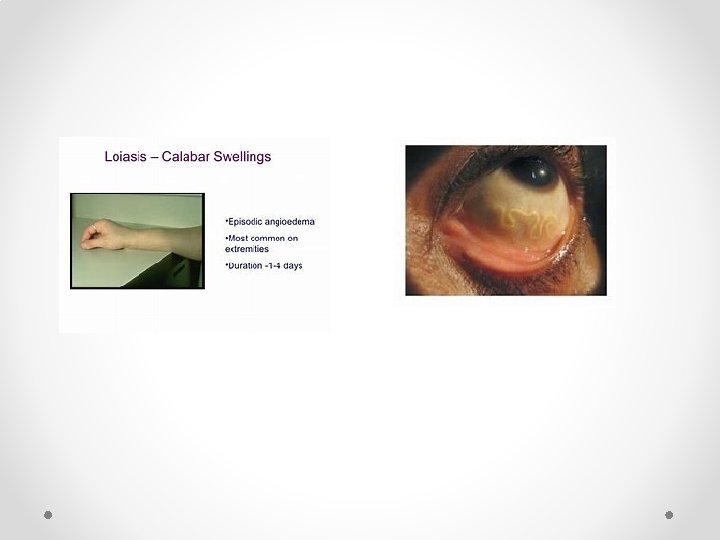
Pathogenesis and Clinical Feature • Calabar Swellings - most common form of Loiasis, also called as fugitive swelling. It is a subcutaneous swelling developing on the extremities • Ocular Manifestations - conjunctival granuloma, edema of the eye lid leading to proptosis (bulging). • Complications- Meningoencephalitis

Laboratory Diagnosis • Microscopy - Definite diagnosis of Loiasis requires Detection of microfilariae in the peripheral blood • Molecular Methods - Nested PCR-based assays for the detection of L. loa DNA in blood • Antibody Detection - Lateral flow assay (ICT)

Treatment • DEC • Albendazole • Apheresis

ONCHOCERCA VOLVULUS • Onchocerca volvulus is the causative agent of “river blindness” in man • Endemic area: The majority of individuals infected with O. volvulus live in the rural poor region of Sub-Saharan Africa, particularly West Africa.

Morphology • Adult Worm - long, thin, tapering at both the ends. They bear transverse striations on the cuticle with annular and oblique thickening. This helps in differentiating from other filarial worms • Microfilaria - skin dermis Microfilariae; Adult worms Transverse section

Life Cycle • Life cycle is similar to that of W. bancrofti, except the vector is Simulium (black flies).
 • Intense pruritus and generalized papular rashes are the most")
Clinical Features Skin (Dermatitis) • Intense pruritus and generalized papular rashes are the most common manifestations. • Leopard skin: Skin may be hypo to hyper pigmented. • Lichenoid changes and hyperkeratosis may occur in late stages • Sowda: It is a chronic hyperreactive form of dermatitis
 Onchocercoma (Subcutaneous Nodules) • Subcutaneous nodules are firm, non-tender,")
Clinical Features (cont. . ) Onchocercoma (Subcutaneous Nodules) • Subcutaneous nodules are firm, non-tender, variable in size containing the coiled adult worms and rarely microfilariae. Ocular Involvement • Bilateral blindness (river blindness) • Conjunctivitis with photophobia • Punctate keratitis: “snowflake opacities” • Sclerosing keratitis - Onchocercal blindness


Laboratory Diagnosis • Detection of the Microfilariae - Skin snips technique: Most common sites: Both iliac crests or sometimes from calves and the shoulders, scapula. • Detection of the Adult Worm - biopsy of the subcutaneous nodules, but it is less sensitive. • Serology- currently developed Ig. G 4 specific dip stick assay detecting Ov 16 antigen may indicate active infection. • Molecular Methods - PCR detecting onchocercal DNA in skin snips

SKIN SNIP BIOPSY Left: A physician takes a skin sample from a patient for a skin snip biopsy by elevating a piece of skin with a needle and shaving it off with a scalpel. Right: A physician takes a skin sample from a patient for a skin snip biopsy using a sclerocorneal biopsy punch.

Treatment • Ivermectin • Doxycycline

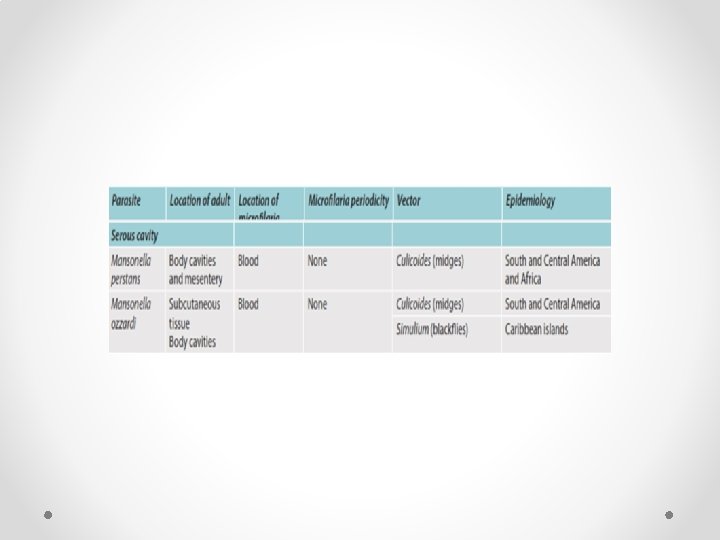
MANSONELLA SPECIES • Mansonella perstans – Causes angioedema, urticaria, pruritus and Calabar-like swelling similar to that of Loa loa. • It also produces acute periorbital inflammation; known as bung-eye or bulge-eye • Treatment - DEC or albendazole are found to be effective; lowering the level of microfilaremia.
 • Mansonella Streptocerca - Many infected individuals are asymptomatic;")
MANSONELLA SPECIES (cont. . ) • Mansonella Streptocerca - Many infected individuals are asymptomatic; few may develop inguinal lymphadenopathy, pruritus, dermatitis with hypo pigmented macule • DEC is effective for streptocerciasis.
 • Mansonella Ozzardi - Most infections are asymptomatic, but")
MANSONELLA SPECIES (cont. . ) • Mansonella Ozzardi - Most infections are asymptomatic, but occasionally cause lymphadenopathy, urticaria, pruritus, pulmonary symptoms, arthralgia and keratitis • Treatment -Ivermectin is effective in lowering the level of microfilaremia. Use of DEC is controversial.
 Microfilaria of Mansonella streptocerca (stained")
MANSONELLA SPECIES Microfilariae of Mansonella perstans (stained with Giemsa) Microfilaria of Mansonella streptocerca (stained with hematoxylin) Microfilaria of Mansonella ozzardi (Giemsa stain)

Thank you!
- Slides: 56