Filarial Worms Wuchereria Bancrofti Disease Benceroftian filariasis or

Filarial Worms Wuchereria Bancrofti Disease: Benceroftian filariasis or elephantiasis. Distribution: Tropical and subtropical areas, Far East, Central Africa and the Nile delta, South and Central America. Hosts: -Definitive: Man only. -Intermediate: Female Culex pipiens mosquito. Habitat: Adult worms are found in lymphatic vessels and lymph nodes of man only, commonly of the lower limbs. Infective stage: Actively motile third-stage filariform larva is infective to man.

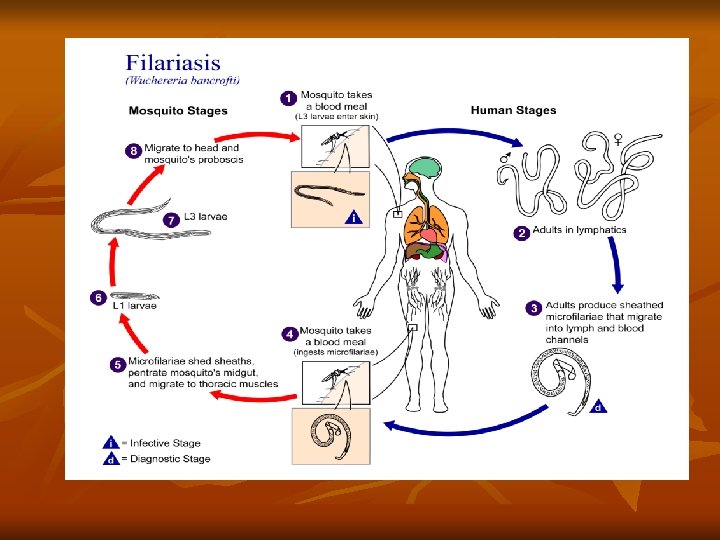
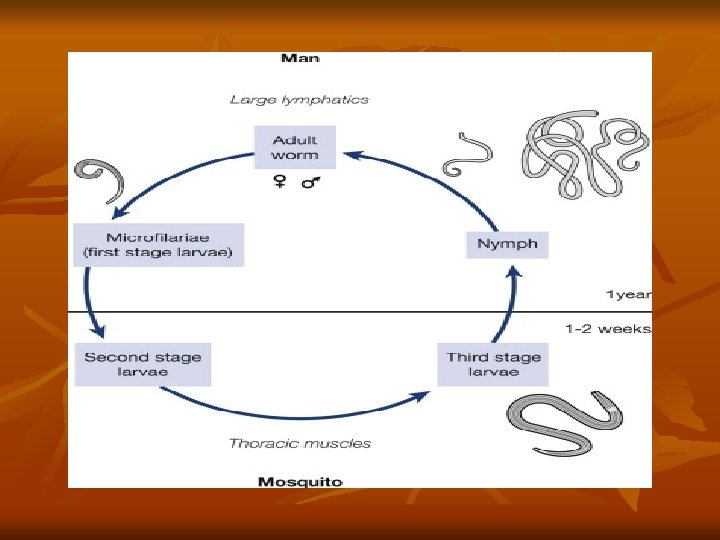
Mode of transmission: Humans get infection by bite of mosquito carrying filariform larva. Life cycle: • When Culex pipiens mosquito feeds on a carrier, the microfilariae are taken in with the blood meal and reach the stomach of the mosquito. • Within 2– 6 hours, they cast off their sheaths (exsheathing), penetrate the stomach wall and then migrate to the thoracic muscles where they undergo further development. • During the next 2 days, they develop into the first-stage larva, which is a sausage-shaped with a spiky tail. • Within a week, it molts once or twice, increases in size and becomes the second-stage larva.

Clinical incubation period: The period from the entry of the infective larvae, till the development of the earliest clinical manifestation is called the clinical incubation period. This is very variable, but is usually 8– 16 months, or longer. Pathogenesis: It occurs due to blockage of lymph vessels and lymph nodes by the adult worms. Blockage could be due to mechanical factors or allergic inflammatory reaction to worm antigens and its secretions. Affected lymph nodes and vessels are infiltrated with macrophages, eosionophils, lymphocytes, and plasma cells.

• In another week, it develops its internal structures and becomes the elongated third-stage filariform larva. It is actively motile and is the infective form. • It enters the proboscis sheath of the mosquito, awaiting opportunity for infecting humans on whom the mosquito feeds. • The larvae enter through the puncture wound or penetrate the skin by themselves. • After penetrating the skin, the third-stage larvae enter the lymphatic vessels and are carried usually to abdominal or inguinal lymph nodes, where they develop into adult forms. • The gravid female worm releases large numbers of microfilariae. They pass through the thoracic duct and pulmonary capillaries to enter the peripheral circulation.
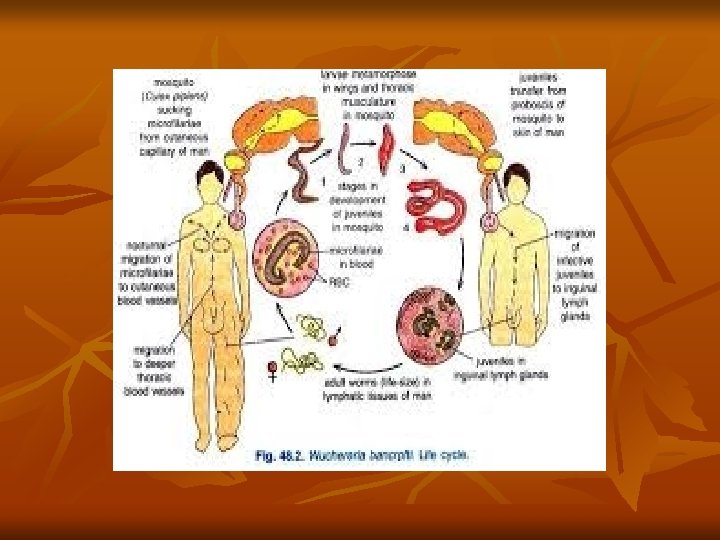

• The microfilariae are ingested with the blood meal by mosquito and the cycle is repeated. Pathogenesis: It occurs due to blockage of lymph vessels and lymph nodes by the adult worms. The blockage could be due to mechanical factors or allergic inflammatory reaction to worm antigens and secretions. Recurrent secondary bacterial infections cause further damage. Clinical manifestations: The most common presentations of lymphatic filariasis are asymptomatic (subclinical) microfilaremia, acute lymphangitis and chroniclymphatic disease.

• Most of the patients appear clinically asymptomatic but virtually all of them have subclinical disease including microscopic hematuria or proteinuria , dilated lymphatics (visualized by imaging) and in men with W. bancrofti infection, scrotal lymphangiectasia (detected by ultrasound). • Lymphangitis is inflamed lymph vessels seen as red streaks underneath the skin which may be associated with streptococcal infection also. • Lymphadenitis: Inflammation of lymph nodes. The lymph nodes become enlarged, painful, and tender. • Elephantiasis: This is a delayed sequel to repeated lympangitis, obstruction and lymphedema.

Repeated leakage of lymph into tissues first results in lymphedema, then to elephantiasis, in which there is non-pitting brawny edema with growth of new adventitious tissue and thickened skin, cracks, and fissures with secondary bacterial and fungal infections, commonly in legs. Diagnosis: • Microfilaria can be demonstrated in blood, It is best to collect ‘night blood’ samples between 10 pm and 4 am. • Radiology: Dead and calcified worms can be detected occasionally by X-ray. • Serodiagnosis: Demonstration of antigens and antibodies by several serological tests as ELISA. • Polymerase chain reaction (PCR).
 is the drug of choice. It is given orally in")
Treatment: 1. Diethylecarbamazine (DEC) is the drug of choice. It is given orally in a dose of 6 mg/kg body weight daily for a period of 12 days amounting to a total of 72 mg of DEC per kg of body weight. 2. Elastic pressure bandages to eliminate the oedema. 3. Surgical reconstruction. Prevention and control: 1 -Avoiding mosquito bites by wearing suitable clothes using mosquito nets, application of repellents. 2 -Destruction of mosquitoes. 3 -Treatment of cases and carriers. 4 -Health education about mode of infection, early diagnosis and control of filariasis.
- Slides: 12