Fig Extensor carpi radialis longus ECRL Extensor carpi

, Extensor carpi radialis brevis (ECRB), Extensor carpi ulnaris (ECU),")

. Mallet : hammer like")








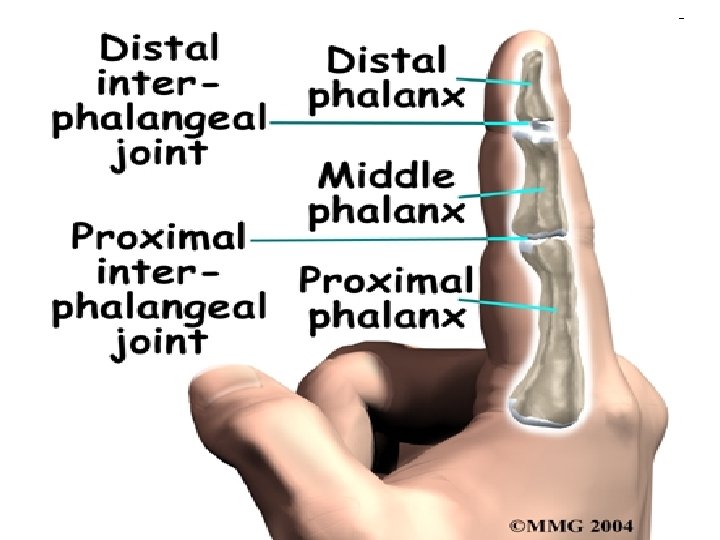
. Lateral view")












- Slides: 27
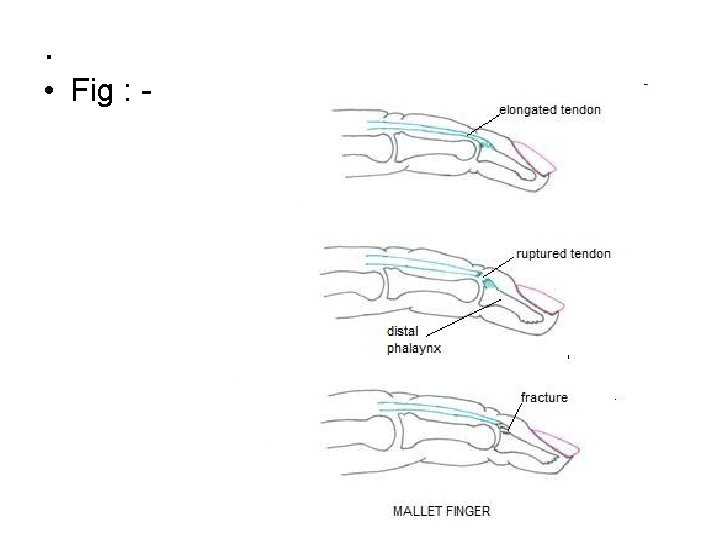
Fig : -
Extensor carpi radialis longus (ECRL), Extensor carpi radialis brevis (ECRB), Extensor carpi ulnaris (ECU), Extensor digitorum communis (EDC), Extensor digiti minimi (EDM), Extensor indicis proprius (EIP), Abductor polliis longus (APL), Extensor pollicis brevis (EPB) and. Extensor pollicis longus (EPL). • Fig :
Fig : - showing the central slip and lateral bands • Fig :
Mallet Finger (baseball finger, drop finger , cricket finger ). Mallet : hammer like Mallet finger of tendon origin Mallet finger of bony origin Mallet finger : flexion deformity of terminal phalanx due to avulsion or rupture of extensor tendon
Mallet Finger • Presentation – DIP Flexion +/- edema. • Imaging – AP, lateral, oblique 1
Mallet Finger 1
Mallet finger: Clinical presentation
Mallet finger deformity due to a closed rupture of the extensor tendon with an associated avulsion fracture of the terminal phalanx
Tendon origin • Due to loss of extensor tendon continuity at the distal finger joint Mechanism of injury : • The end of the finger is forcibly flexed , when extensor tendon is taut , e. g catching a ball , striking an object with extended finger
Extensor tendon rupture • Fig : -
Fig : • mallet deformity of the right middle finger along with the normal left finger shown for comparison.
Cont. . • Baseball finger (dropped finger, mallet finger). Lateral view
Four types of mallet finger injuries • Type I: Closed with or without avulsion fracture • Type II: Laceration at or proximal to the DIP joint with loss of tendon continuity • Type III: Deep abrasion with loss of skin, subcutaneous cover and tendon substance • Type IV: • (A) Trans-epiphyseal plate fracture • (B) Hyperextension injury with fracture of the articular surface and • (C) Hyperextension injury with fracture of the articular surface and with early or late palmar subluxation of the distal phalanx.
Fig : - mallet finger injury at the DIP joint
Treatment For type I injuries : • continuous splinting of the DIP joint in extension for six weeks, followed by two weeks of night splinting. - K – wire fixation of the DIP joint in extension, for six weeks followed by two weeks of night splinting.
Fig : showing the use of a splint in treating closed mallet injury
Type II • injuries may be repaired with a simple figure-of-eight suture through the tendon alone. • DIP joint is splinted in extension for 6 weeks, followed by 2 weeks of night splinting.
Cont. . Type III injuries with loss of tendon substance require : • immediate soft tissue coverage and primary grafting or late reconstruction using a free tendon graft.
Cont. . Type IV-A : • closed reduction followed by splinting for 3 -4 weeks. Type IV-B with no palmar subluxation: • good results with 6 weeks splinting and 2 weeks night splinting. Type IV-C with palmar subluxation of the distal phalanx : • open reduction and internal fixation using K wire. splint for 6 weeks, after which the wire is removed and motion started.
Fig : - external fixator in position. • .
Posture When relaxed, the hand lies in a characteristic posture with the thumb-tip held slightly flexed and fingers held in a cascade. Any change in the resting posture can suggest tendon or even nerve damage • Fig : -
Fig : - Examination of the extensor tendons showing normal function of the extensor communis (left) and extensor proprius (right) tendons
Flexion of the fingers demonstrates loss of active movement at the tip of the ring finger (due to a closed flexor tendon (FDP) rupture)
Mallet Finger Thumb Splint