Fibrous Dysplasia craniofacial fibrous dysplasia skull and facial

骨纤维异常增殖症 Fibrous Dysplasia


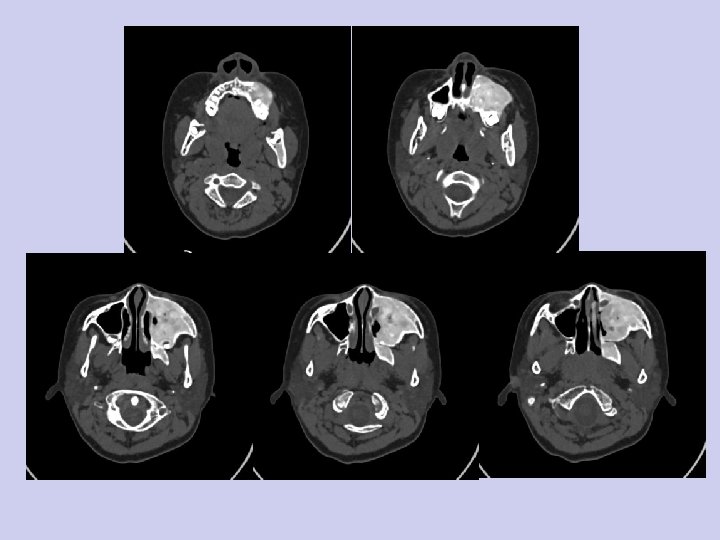
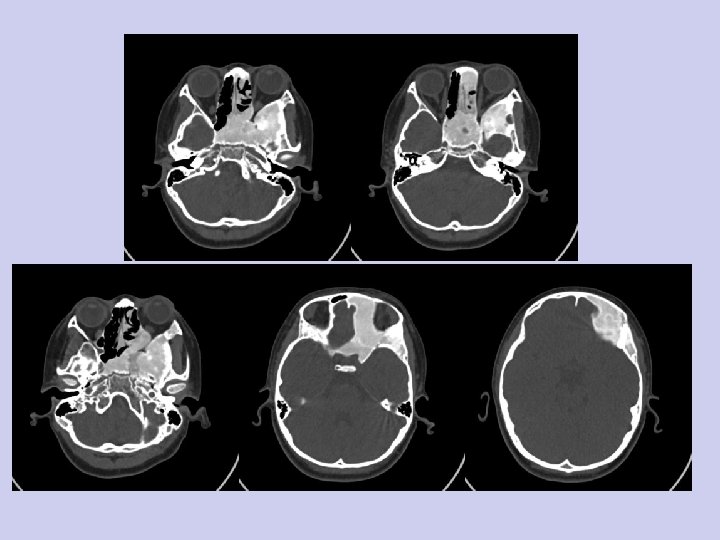
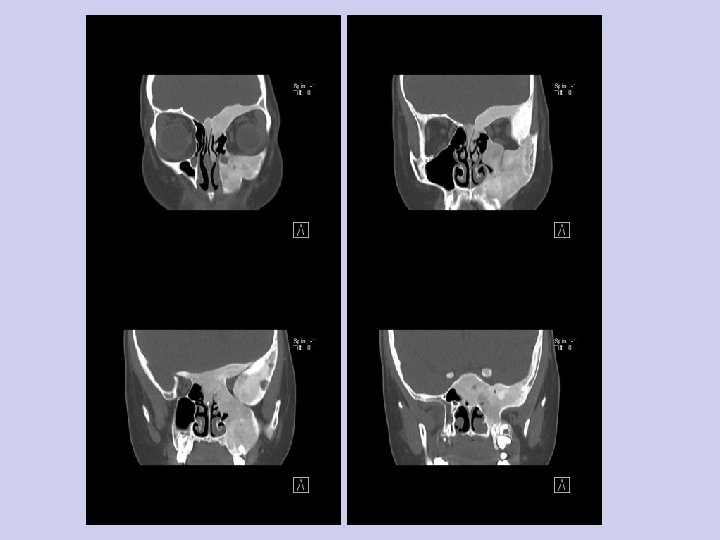
其他分类 • 颅面骨纤维异常增殖症 • craniofacial fibrous dysplasia - skull and facial bones alone • 家族性巨颌症 • cherubism - mandible and maxilla alone (not true fibrous dysplasia)







骨扫描 Ø Bone scanning can be helpful in conjunction with radiography to detect polyostotic involvement. Intense uptake of gallium is seen in the dysplastic bone. Ø 在一些囊性及“磨玻璃” 型病变中,放射性摄取 可等同于正常骨组织。

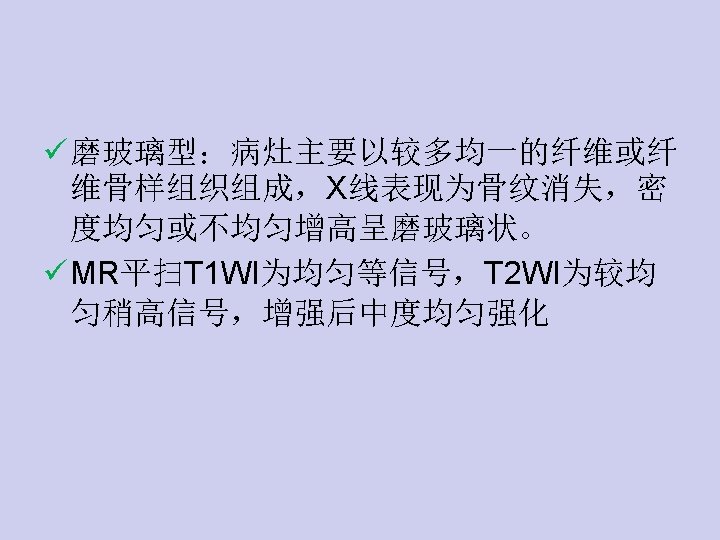
THANKS





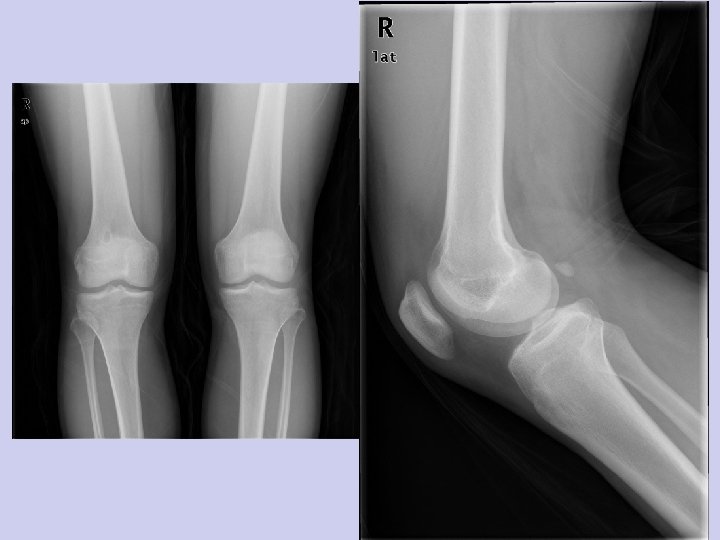


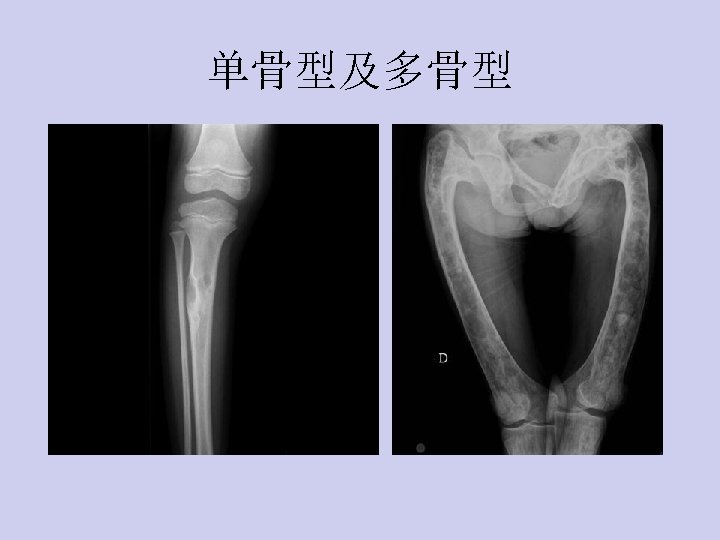
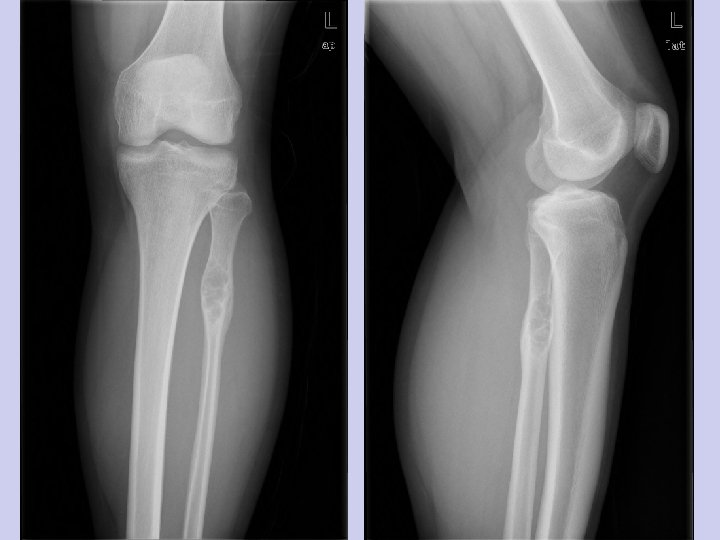
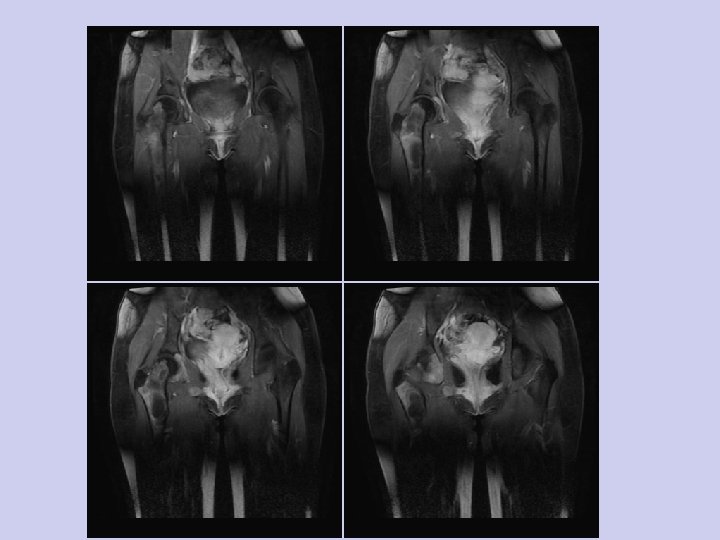
• Radiographs of the right knee and femur revealed foci of increased density in the proximal, lateral tibial plateau without evidence of a fracture. Foci of increased density leading to a ground glass appearance throughout the femur with expansion of the femoral neck consistent with fibrous dysplasia.

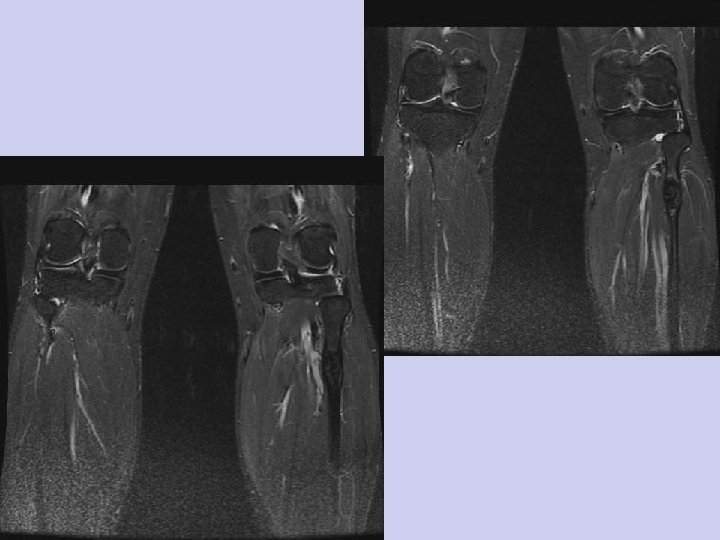
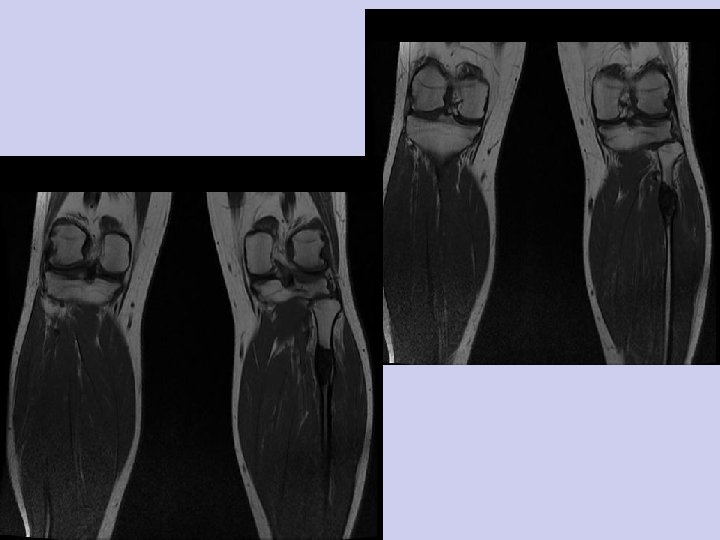
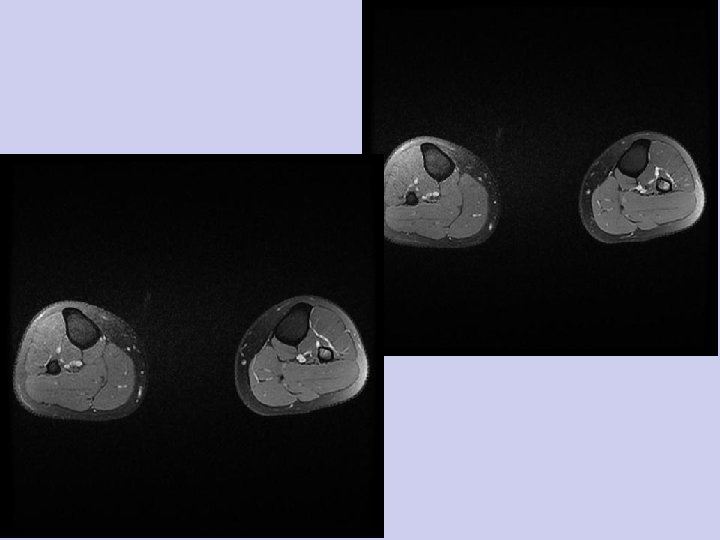
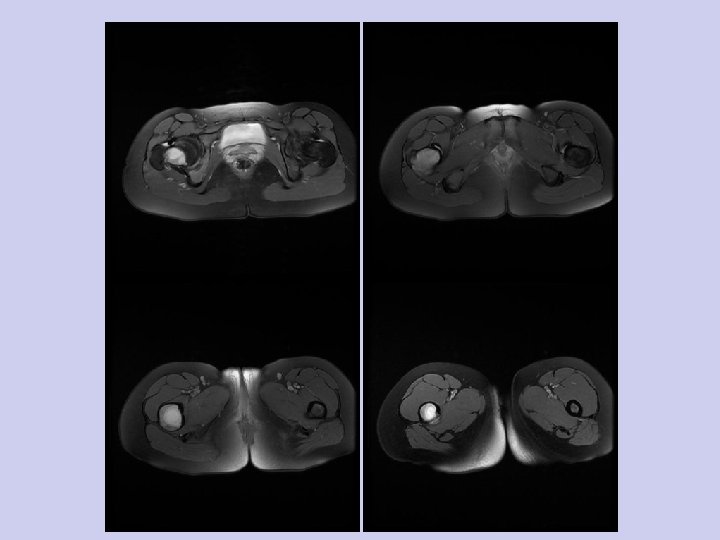
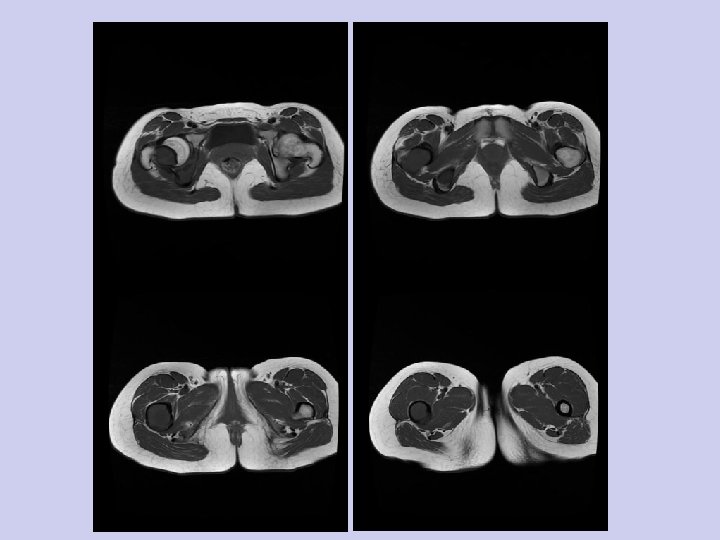
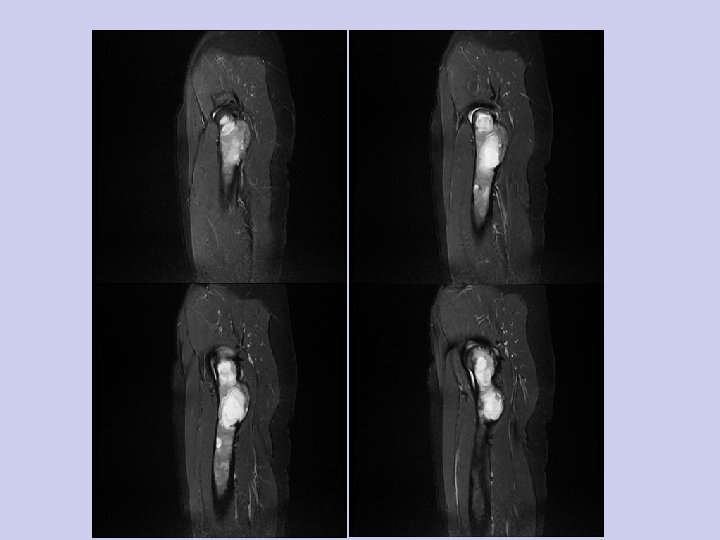
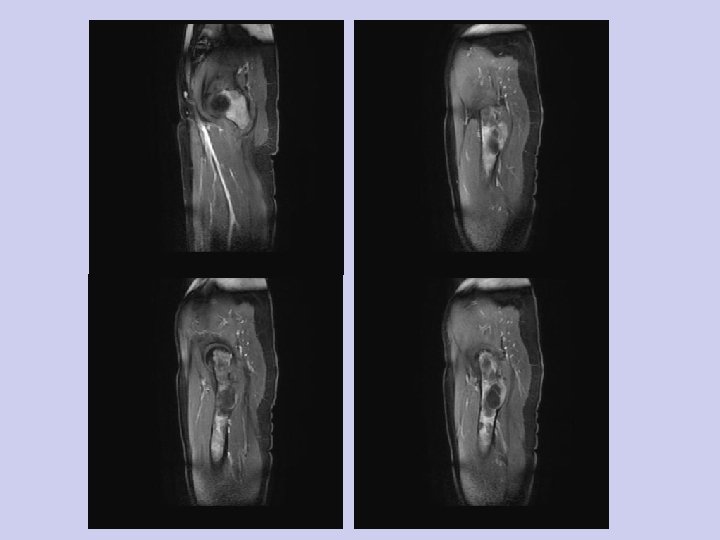
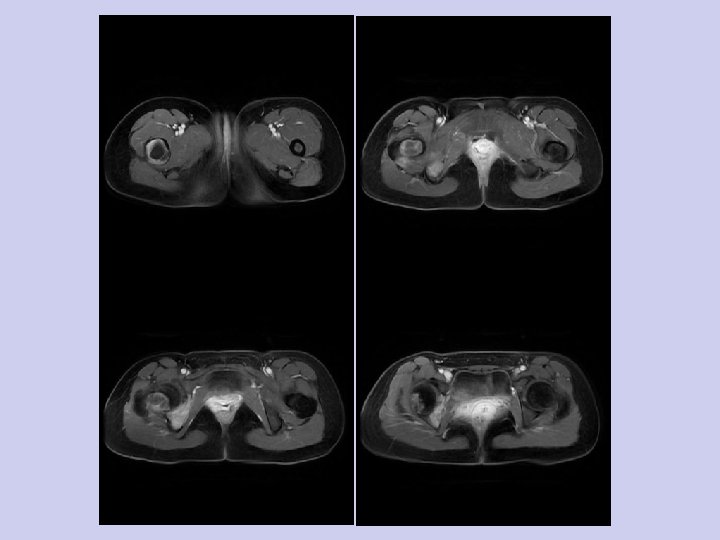
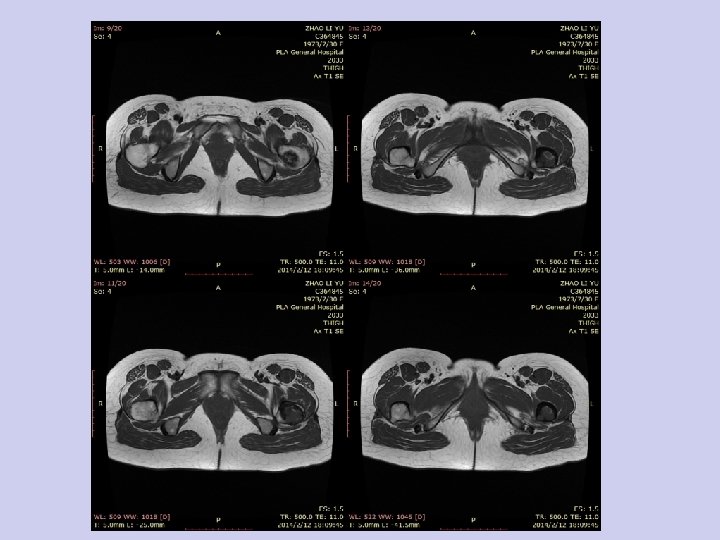
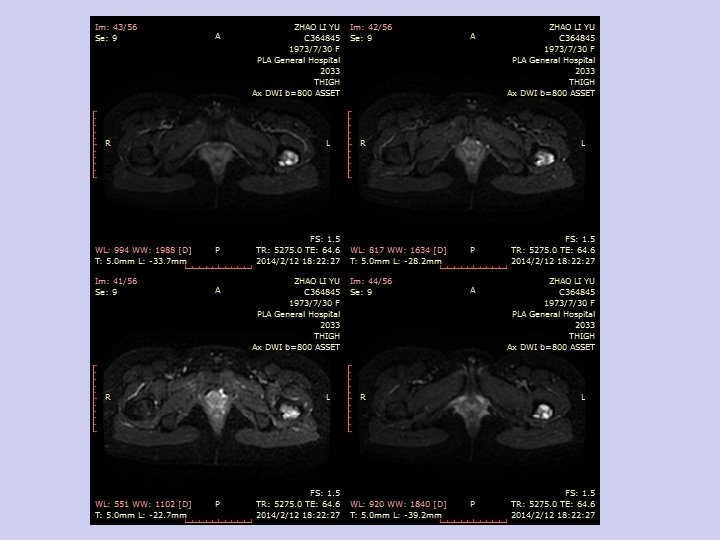
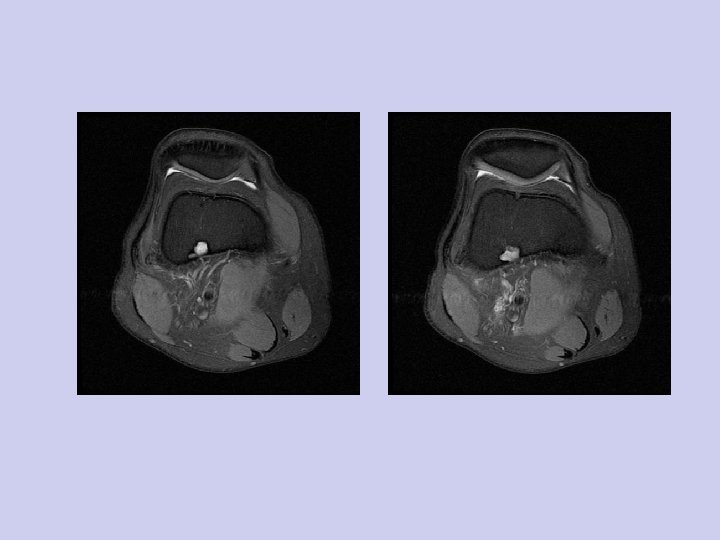
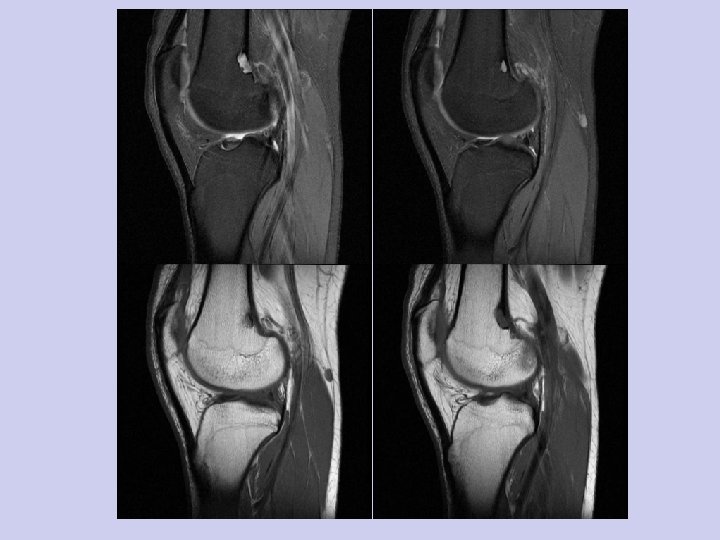
• MRI of the right knee showed a mass in the lateral aspect of the proximal tibia that breeches the osseous cortex and extends into the muscles of the anterior compartment. A narrow zone of transition is seen between the mass and surrounding tissues. Marginal enhancement of the lesion is seen. There is no surrounding edema or evidence of vascular invasion.

Scintigraphy • The majority of lesions in fibrous dysplasia are tracer avid on Tc-99 m MDP bone scans. Machida et al(3) analyzed 59 lesions in 26 patients with fibrous dysplasia. Four (14%) of 29 cystic lesion and two (7%) of 30 "ground glass" lesions had radiotracer uptake equivalent to normal bone. The remainder showed supra-normal tracer uptake. Bone scanning can be helpful in conjunction with radiography to detect polyostotic involvement. Intense uptake of gallium is seen in the dysplastic bone.

Natural History • A variable clinical course is seen. Patients are often asymptomatic. Others experience pain, pathologic fractures and bone deformity. Craniofacial fibrous dysplasias can result in impingement of the cranial nerves. An increased incidence of sarcomas is seen in dysplastic lesions, unattributable to prior radiation therapy. Ruggieri et al (4) in a review of 1122 cases of fibrous dysplasia and found 28 cases of sarcoma. Prior radiation of the dysplastic bone occurred in 13 of the 28 cases (46%). The histologic subtypes seen in descending order of frequency were:
, fibrosarcoma (5/28 cases), chondrosarcoma (3/28 cases), and malignant")
• • osteosarcoma (19/28 cases), fibrosarcoma (5/28 cases), chondrosarcoma (3/28 cases), and malignant fibrohistiocytoma (1/28 case).

• The incidence of sarcomatous degeneration is approximately 1%. Associated symptoms include pain and swelling. Clinical mimics of sarcomatous degeneration are the coexistence of a secondary aneurysmal bone cyst and cystic degeneration of fibrous dysplasia. The most constant radiographic feature of malignant degeneration is extension of the lesion through the bone cortex into the surrounding soft tissues. The prognosis for these secondary sarcomas is poor and similar to that for their primary counterparts.


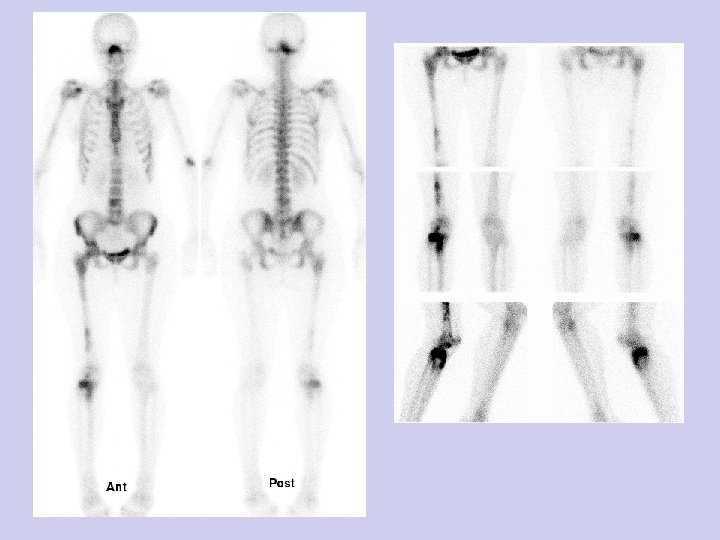
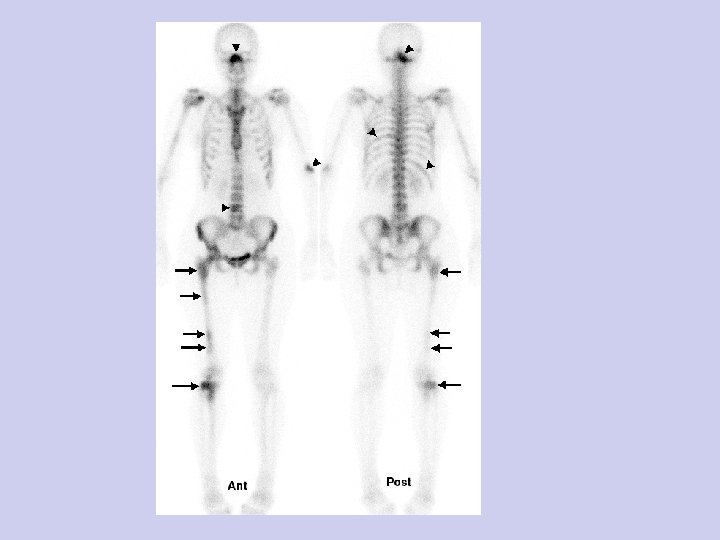
• Bone Scan • Whole body bone scan and spot views of the legs show focal very avid uptake in the proximal right tibia and fibula (shown by arrows). There are foci of abnormal uptake throughout the right femoral diaphysis, metaphysis and head with expansion of the intertrochanteric region. Abnormal increased uptake in the L 4 vertebra, left 8 th rib, right 11 th rib, distal right humerus

• Mc. Cune-Albright syndrome - in 2 -3 % of cases with the polyostotic form • isolated endocrinopathy without the full Mc. Cune-Albright syndrome precocious puberty in girls – hyperthyroidism – hyperparathyroidism : renal stones, calcinosis – acromegaly – diabetes mellitus – Cushing syndrome : osteoporosis, acne – growth retardation • Mazabraud syndrome - soft-tissue myxomas (rare) ; typically multiple intramuscular lesions in vicinity of most severely affected bone
- Slides: 110