FIBROMYOMAS OF THE UTERUS Dr Madhavi Karki Benign

FIBROMYOMAS OF THE UTERUS Dr. Madhavi Karki

Benign Neoplasm Synonyms : Leiomyomas, fibroids or simply myomas Commonly encountered in gynecological practice in the reproductive age group females

Etiology Age : 3545 years Parity : Nulliparo us Race: Blacks Hyperestrogenic states : pregnancy pill users

Pathology Microscopic features: -It is composed of muscle tissue although there is a variable amount of fibrous connective tissue. Naked eye examination: Myomas are frequently multiple and as many as 200 may be found in one uterus. More often the number is between 5 -10.

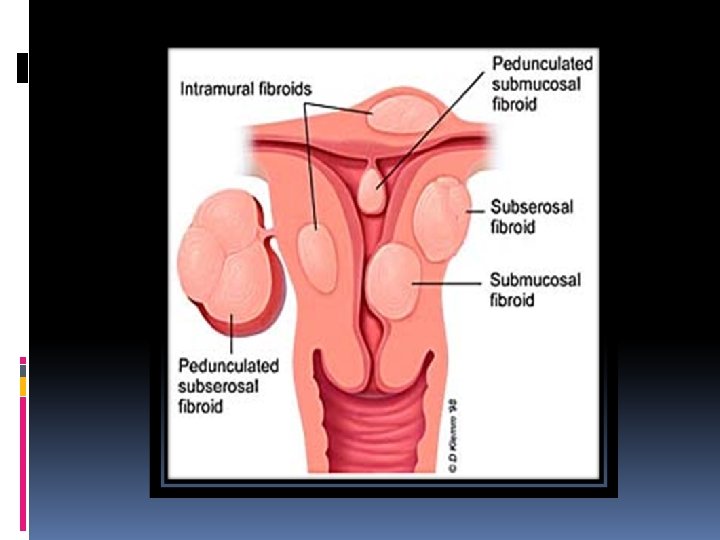
TYPES OF FIBROID Intramural Fibroid • The tumor remains within the myometrial wall Subserous Submucous • If the tumor grows outwards into the peritoneal cavity • Uterine contractions can force the myoma towards the cavity where it is covered by a thin endometrium

Secondary Changes Atrophy Degenerations Sarcomatous changes

Other complications of myomas Torsion Inversion Infection Endometrial carcinoma
 Pain Pressure symptoms")
Symptoms Menstrual disorders Infertility Asymptomatic (50%) Pain Pressure symptoms

Signs Abdominal examination: If the tumor is larger than 14 wks, it can be felt per abdomen Percussion: -The swelling is dull on percussion. Pelvic examination. Bimanual examination reveals, uterus is irregularly enlarged. Fornices will be felt free. The cervix moves with the movement of the tumor felt per abdomen.

INVESTIGATIONS Hemoglobin, blood grouping USG Hysterosalpin gography Hysteroscopy Uterine curettage Laparoscopy MRI

Treatment Small and asymptomatic cases do not require removal. They can be observed every 6 months. Indications of treatment are : - Infertility and habitual abortion - Symptomatic fibroids : menorrhagia and pressure symptoms - Rapid growth in a menopausal women - When the nature of the tumor cannot be ascertained clinically then laparotomy is required.

TREATMENT MEDICAL MINIMALLY INVASIVE SURGERY
- Slides: 13