FFR and i FR guided NSTEMI for Culprit







 Similar in angina and NSTEMI –not STEMI")







 Outcomes-Deferred pts")


- Slides: 33
FFR and i. FR guided NSTEMI for Culprit and Non –Culprit lesions Jasvindar Singh MD, FACC Associate Professor of Medicine Washington University in St. Louis Barnes-Jewish Hospital
FFR and i. FR guided NSTEMI for Culprit and Non –Culprit lesions …………. Jasvindar Singh, MD Disclosure Research /Grant support: Philips-Volcano Corp. , Abbott Vascular, Medtronic Vascular , Boston -Scientific Consulting: Philips-Volcano Corp, Boston-Scientific, Abbott Vascular, Medtronic Vascular , CSI
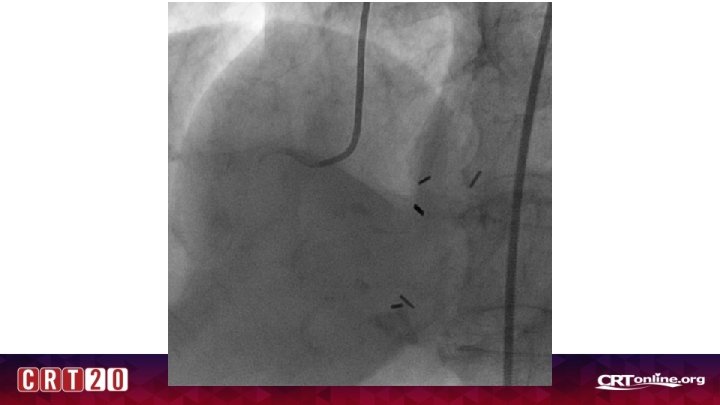
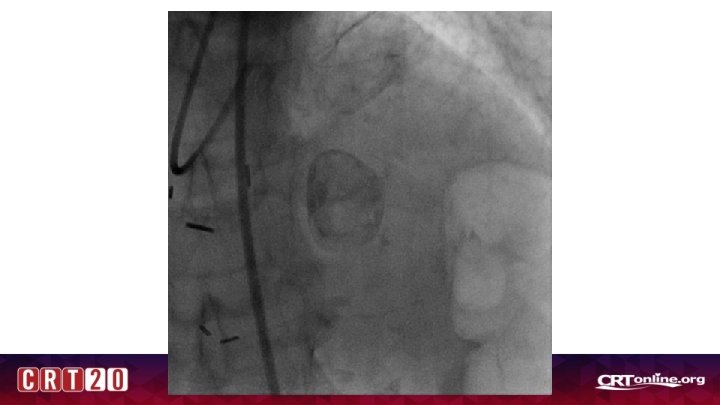
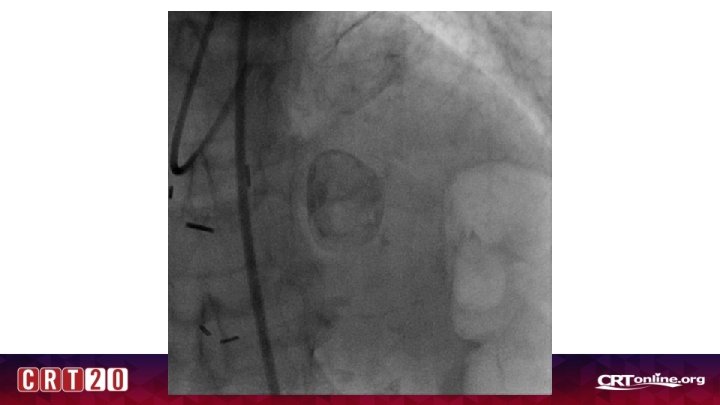
Case 1 • 77 yr old WF with PMN of osteoarthritis, osteoporosis, renal mass being monitored closely, hypothyroidism who presented with weakness, nausea, and atypical chest pain. Had several months of nonspecific periodic nausea leading up to admission. • BP 170/70, HR 75 • EKG: NSR, Normal EKG • Hgb 11. 3, Plt 195 • Cr 0. 80 • Trop 3. 00 > 3. 78 > 3. 66 • Referred for coronary angiogram for NSTEMI
Where is the culprit?
Introduction
Outline- Questions to address • Is FFR valid in ACS (do we achieve maximal hyperemia? ) • Are culprit and non –culprit vessels different in NSTEMI? • Do the stable angina cutoffs still hold up for NSTEMI patients? • What data do we have? • Is i. FR more reliable in ACS?
THREE SCENARIOS • Culprit • Non-Culprit • Unclear culprit
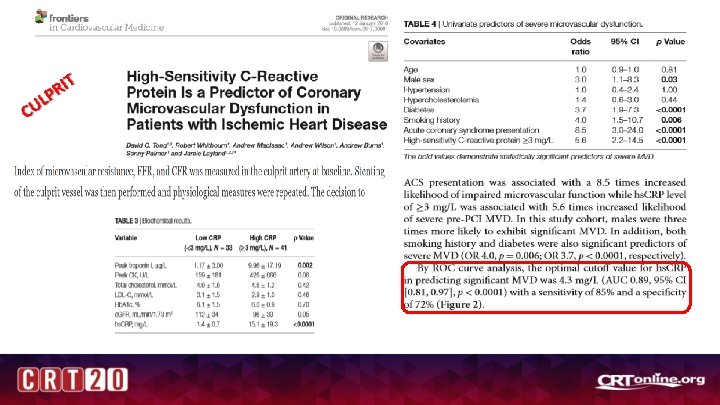
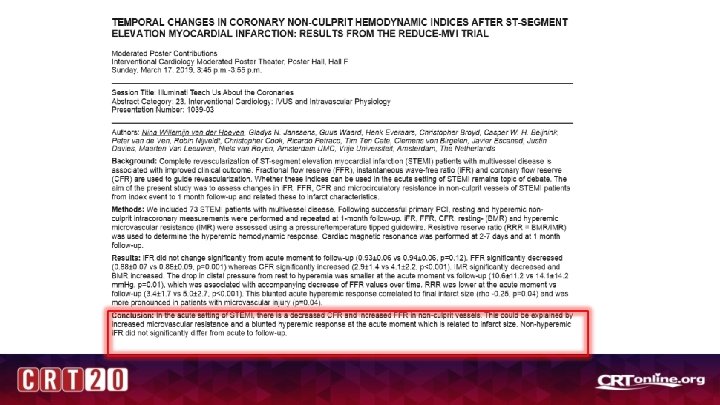
Index of Myocardial Resistance (IMR) Similar in angina and NSTEMI –not STEMI
CU LP RI T Microvascular resistance ACS /NSTEMI
Culprit lesion: FAMOUS-NSTEMI Outcome FFR Group N=176 Angio Group N=174 PValu e Total Lesions 355 351 NR Lesions FFR <0. 8 208 (58. 6) 222 (63. 6) NR Medical Management 40 (22. 7) 23 (13. 2) 0. 02 PCI 125 (71) 139 (79. 9) 0. 05 MACCE 12 months 13 (7. 4) 16 (9. 2) 0. 56 (%) and changed management in roughly 20% patients. Deferring lesions was. Nsafe Eur Heart Jrl. 2015; 36: 100 -111.
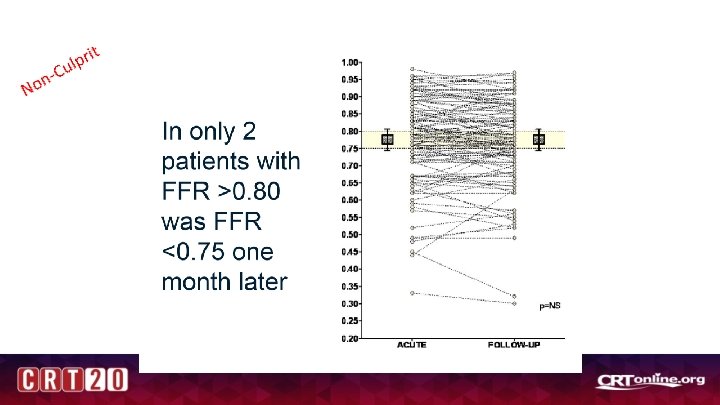
t Non pri l u C
LVEDP FFR
Unclear Culprit
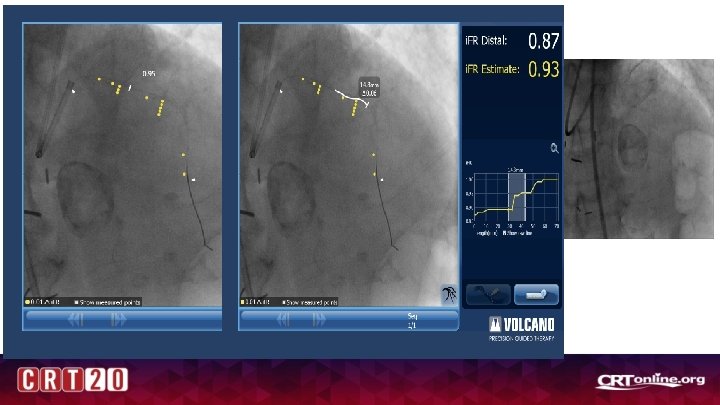
i. FR
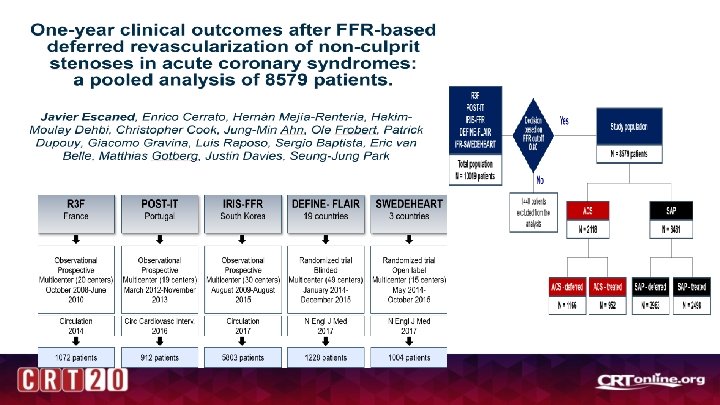
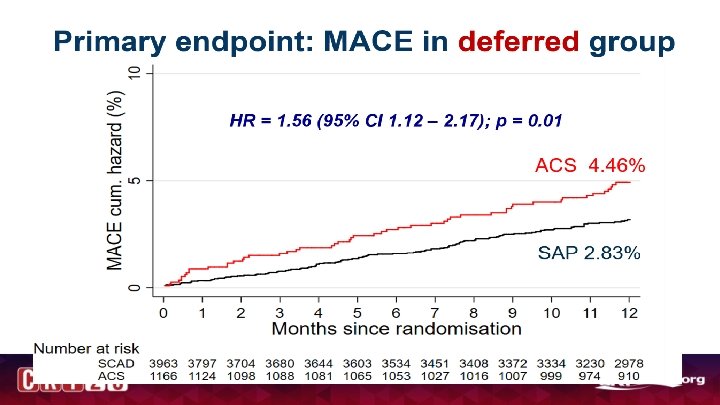
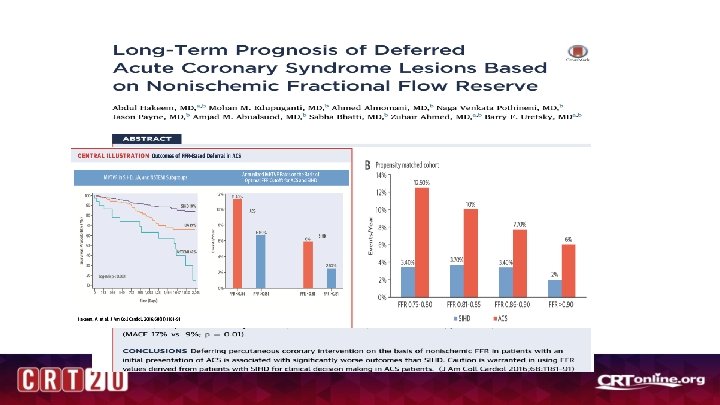
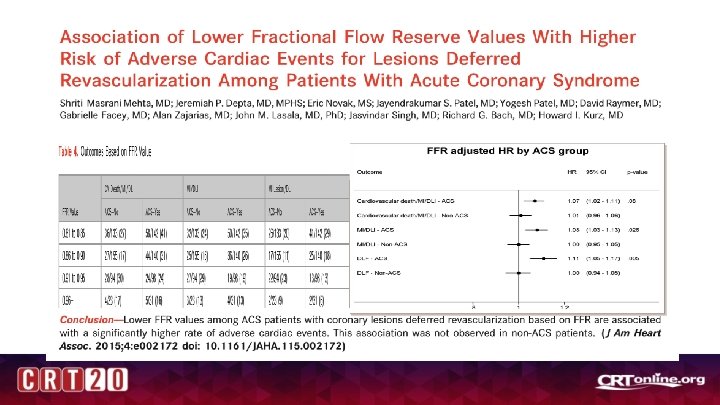
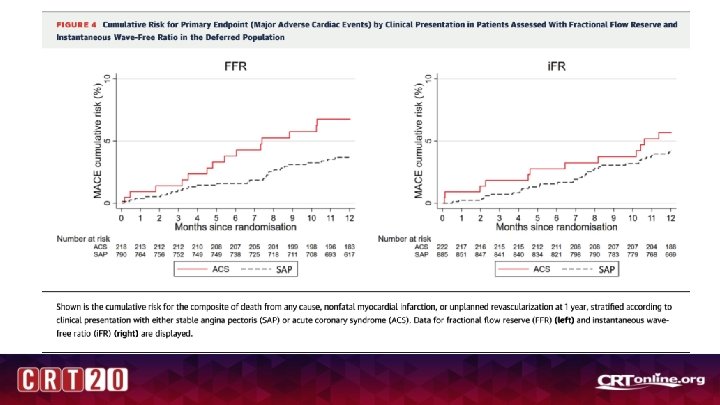
MACE (all pts) Outcomes-Deferred pts
Outcomes in Deferred pts according to clinical presentation
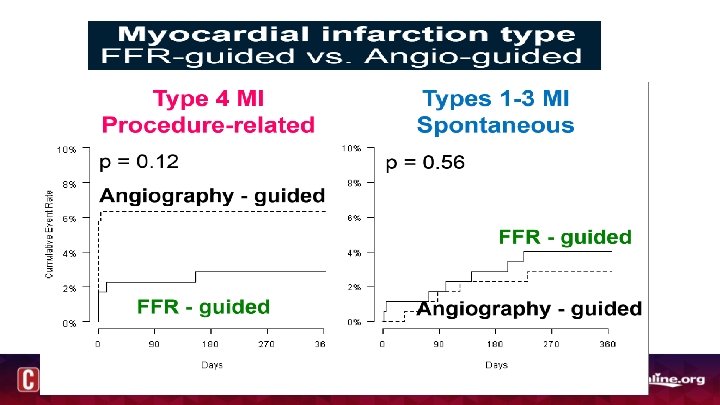
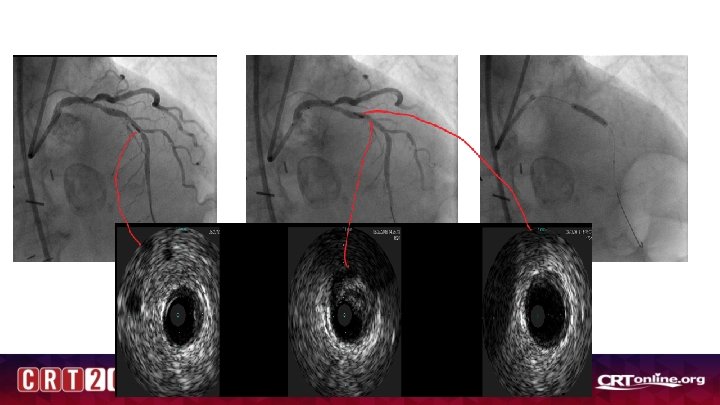
Conclusions • Event rate is higher in deferred lesions in NSTEMI /ACS patients • Non-culprit vessel FFR is reliable and did not change significantly at follow up (although only at ~1 month- 6 month may be different) • Culprit vessel –FFR reliable and better than Angio-guided, but may be falsely negative in patients with high troponins and CRP and higher LVEDP (20 -25% of patients) -Also trend towards more events , spontaneous MI at follow up • IFR vs FFR data is ACS is interesting and needs further study • Co-Registration with resting indices may have promise in unclear culprit subsets