Fetal physiology and fetal circulation Prepared by Ayda

Fetal physiology and fetal circulation Prepared by : Ayda khader Feb. 2017

Fetal physiology Some aspect of the development of fetal organs and their physiology are very important to be discussed for maternity nurse.

1. Cardiovascular System It’s the first to functioning in the developing human that blood vessel formation begins in the 3 rd week after conception. Development of the heart and vessels begins in the embryonic period. The first vessels and blood cells appear in the fourth week. The heart is beating and developing four chambers at 5 th week after fertilization. Fetal heart rate is range between 120 to 160 beats /min.
 System The origin of fetal blood is from the inner cell")
2. Hematopoietic (Blood) System The origin of fetal blood is from the inner cell mass that begin their synthesis in the liver about 6 th weeks of gestation later generated from spleen and bone marrow. The fetus will inherit the genes that determine its blood group from both parents. Fetal hemoglobin is differs most from the adult hemoglobin as can carry 20 -30% more oxygen than can maternal Hb. The fetal Hb concentration is 18 -20 g/dl that considers about 50% greater than maternal hemoglobin. The RBCs and Rh factor are formed by the end of 6 th week of gestation while platelet is formed at 11 th week.

3. Renal System The fetal kidneys develop rapidly at 5 th week and begin to function and passing urine at 8 th week. The urine is very diluted as it’s not the main route of excretion since mother eliminates waste products across placenta. The urine is excreted into and mixed with amniotic fluid

4. Central Nervous System This is derived from ectoderm layer that begin to develop during 3 ed week. The neural tube complete closure at 4 th week. If it does not close, defect such as anencephaly (cephalic end of the neural tube fails to close) and spina bifida (opening in the spinal cord) result.

5. Skin The fetus is covered with a white, creamy substance at 18 th week (vernix caseosa) At 20 th week, the fetus is covered with a fine hair called lanugo that will be shed again at 36 th week and a full term infant has little left.

6. Gastrointestinal System It’s formed at 4 th week but its function as an alimentary tract not accomplished before delivery. Intrauterine nutrition and elimination occur through the placenta. The fetus receive own glucose from the mother. The maternal insulin does not pass into the fetus as the fetus secrete insulin The fetus begins swallowing amniotic fluid at 12 th weeks of gestation (2 nd trimester).

Meconium is the earliest stools of an infant. Unlike later feces, meconium is composed of materials ingested during the time the infant spends in the uterus: intestinal epithelial cells, lanugo, mucus, amniotic fluid, bile, and water. Meconium is almost sterile and has no odor. It should be completely passed by the end of the first few days of postpartum life.

7. Respiratory System The lower respiratory tract begins growth as a part from upper digestive tract at 4 th weeks after conception which is tubular at this time that gradually esophagus and trachea are separated later. Fetal lungs don’t function until after delivery.

8. Reproductive System The male and female external fetus genitalia appear to some extent as similar until the end of 9 th week. It’s well enough developed to be differentiated at 12 th week. By 30 th week of gestation the female fetus has all the ova she will ever have.

9. Endocrine System The thyroid gland is the first endocrine gland to develop in the fetus that by 4 th week. Beta cells of the fetal pancreases are starting to extract insulin by 12 th week.

10. Hepatic System Liver function begins at the 4 th week of gestation, but does not achieve their function well until after delivery. The production of fetal liver enzymes is limited especially in the fetus of less than 36 weeks gestational age.

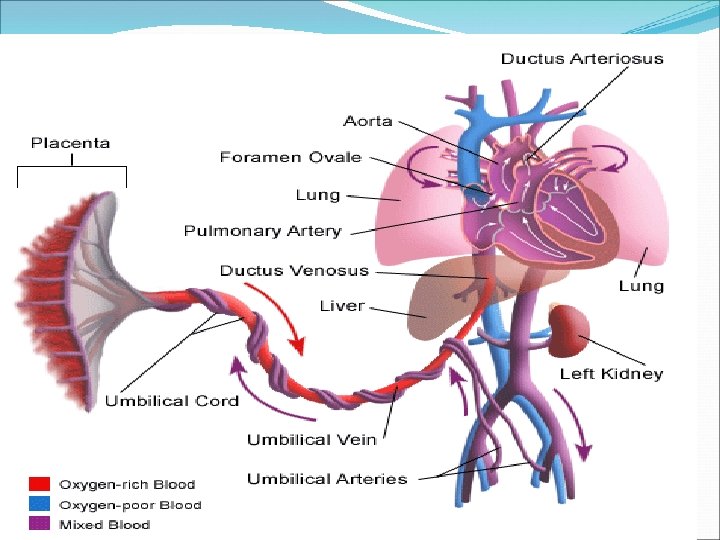
Fetal circulation The placenta is the source of oxygenation, nutrition and elimination of waste for the fetus. The circulatory system of the mother is not directly connected to that of the fetus, so the placenta functions as the respiratory center for the fetus as well as a site of filtration for plasma nutrients and wastes The single umbilical vein carries oxygen enriched blood from the placenta. The paired umbilical arteries return most of the mixed blood from the descending aorta to the

There are several temporary structures in addition to the placenta and the umbilical cord that enable the fetal circulation ( intrauterine): * Ductus venosus: connects the umbilical vein to the inferior vena cava. (vein to vein) * Ductus arteriosus: connects the main pulmonary artery to the descending aorta. (artery to artery) * Foramen ovale: anatomic opening between the right and left atrium. * The hypo gastric arteries: which branch off from the internal iliac arteries and become the umbilical arteries when they enter the umbilical cord

Adaptation to extra uterine life: These structural changes become permanent and become as follows: • The umbilical vein becomes the ligamentum teres • The ductus venosus becomes the ligamentum venosum • The ductus arteriosus becomes the ligamentum arteriosum • The foramen ovale becomes the fossa ovalis • The hypogastric arteries are known as the obliterated hypogastric arteries

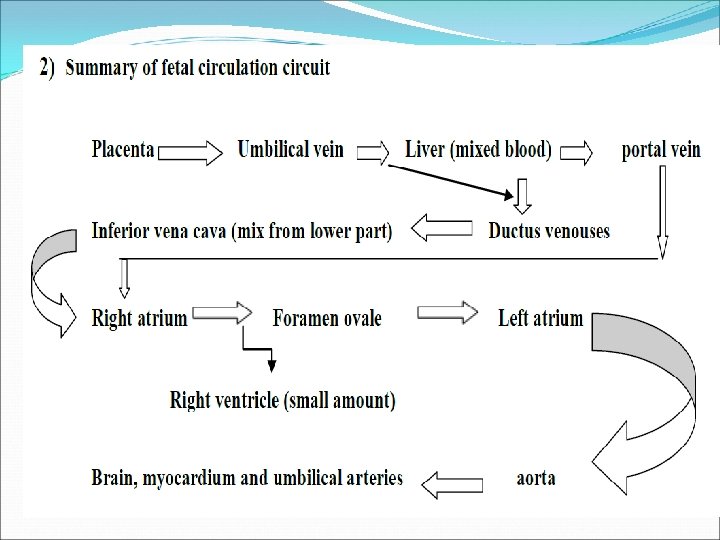
Fetal circulation circuit: The umbilical vein enters the body through the umbilical ring and travels along to the liver and joins with the portal vein. The blood then moves to the right atrium of the heart. About half of the blood passes into the liver. The other half enters a vessel through ductus venosus which bypasses the liver (the newly oxygenated blood). The ductus venosus travels a short distance and joins the inferior vena cava. There, the oxygenated blood from the placenta is mixed with the deoxygenated blood from the lower parts of the body. This mixture continues through the vena cava to the right atrium.

In the adult heart, blood flows from the right atrium to the right ventricle then through the pulmonary arteries to the lungs. While in the fetus, the lungs are non-functional and the blood largely bypasses them As the blood from the inferior vena cava enters the right atrium, a large proportion of it, is shunted directly into the left atrium through an opening called the foramen ovale because of pressure in the right atrium is higher than left atrium.

The more highly oxygenated blood that enters the left atrium through the foramen ovale is mixed with a small amount of deoxygenated blood returning from the pulmonary veins. This mixture moves into the left ventricle and is pumped into the aorta. Some of it reaches the myocardium through the coronary arteries and some reaches the brain through the carotid arteries. The rest passes into the umbilical arteries, which branch from the internal iliac arteries and lead to the placenta. There the blood is re-oxygenated

- Slides: 22