FETAL MRI an approach to practice Yarmaniani M

 (X-ray; CT) • US")










 6 4 2 0 Feb")
 DETECTED BRAIN: anencephaly, microcephaly, cephalocele, porenchepalic cyst, ventriculomegaly, intraventricular bleeding, dysgenesis")
 DETECTED ABDOMEN : esophageal atresia w/w. o. fistula, duodenal atresia, gastroschizis,")






















- Slides: 41
FETAL MRI an approach to practice Yarmaniani M Muchtar, MD Ido N. Bramantya, MD Department of Radiology
PRINCIPLES OF IMAGING DURING PREGNANCY • Avoid ionizing radiation (IR) (X-ray; CT) • US modality of choice • MRI adjunct diagnostic test for fetal ab. N interpretation clinical history & US
PRENATAL US LIMITATIONS • • • Large maternal body habitus Abdominal scars decrease US beam penetration Fetal lie Oligohydramnios Small FOV Limited resolution (relative)
WHEN TO PERFORM MRI • Valid medical reason • Only in select circumstances for screening • US limitations inconclusive ACR-SPR Practice Parameter For The Safe And Optimal Performance OF Fetal Magnetic Resonance Imaging (MRI) (Resolution 11; Revised 2015)
IS MRI SAFE IN PREGNANCY? • No effect on embryogenesis • No effect / risk to fetal hearing (Reeves et al 2010, Strizek et al 2015) • Not known significant side effects • Accepted at any stage of pregnancy • Informed consent The safety committee of the society of MRI 1991 Clements H et al, 2000. Kok RD et al, 2004; white paper (Kanal et al, 2002) ACR & SPR, 2012 (revised 2015)
COMFORT IS KING Stacey Goergen. Obstetric MR. Melbourne 2017
CHALLENGES AND SOLUTIONS • Fetal motion. We avoid maternal sedation Solution: ultrafast MRI sequences • Small-sized developing structures Solution: advances MRI surface coils & gradients
CHALLENGES AND SOLUTIONS • 3 T Machine: Artifacts, SNR, SAR Solution: technical, patient screening • Peri-procedural ethics • Communicating with pts • Don’t give results independently to pts • Discuss with FM Obgyn, Neurosurgeon, etc
WHO? ? WHERE? ? • MR technologist & attending radiologist familiar with fetal MR procedure & diagnosis • Preferred in 1, 5 T MR machine • We used 3 T MR machine
FETAL MRI INDICATIONS FETAL ORGANS Indications Brain Congenital anomalies, vascular abnormalities Spine NTD, etc Head and Neck Mass, airways obstruction Thorax Congenital lung malformation, CDH, mass, lung volumetry; assessment of esophageal atresia Abdomen & Pelvis Mass, GU anomatlies, renal anomalies, bowel anomalies Twins Complications of MCT Fetal surgery planning Assessment ACR-SPR Practice Parameter For The Safe And Optimal Performance OF Fetal Magnetic Resonance Imaging (MRI) (Resolution 11; Revised 2015)
FETAL MRI: a screening tool In a study of 66 fetuses at high risk for brain anomaliles (16 WG and above), fetal MRI changed US diagnosis in 40%, changed counseling in 55%, and management in 46% Saleem SN, et al. The impact of fetal MRI findings on counseling and management in high risk pregnancies for brain malformations. EJRNM 2008; 1(2): 20 -25
RSAB HK: our almost-one-year experience 8 44 FETAL MRI(s) 6 4 2 0 Feb Mar Apr May Jun Jul Aug Sept Oct Nov Dec
ANOMALIES (WE HAVE) DETECTED BRAIN: anencephaly, microcephaly, cephalocele, porenchepalic cyst, ventriculomegaly, intraventricular bleeding, dysgenesis corpus callosum, megasisterna magna, etc SPINE: spinal dysraphism THORACIC: CPAM, CDH
ANOMALIES (WE HAVE) DETECTED ABDOMEN : esophageal atresia w/w. o. fistula, duodenal atresia, gastroschizis, cloacal malformation, renal agenesis, MDK, ARPKD MSK : skeletal dysplasia TWINS : complications
FETAL BRAIN: normal & abnormal • Sulci – Gyri • Midline structures & CC • Ventriculomegaly • Parenchymal lesions • Posterior fossa • Complex anomalies
NORMAL FETAL BRAIN ABNORMAL FETAL BRAIN
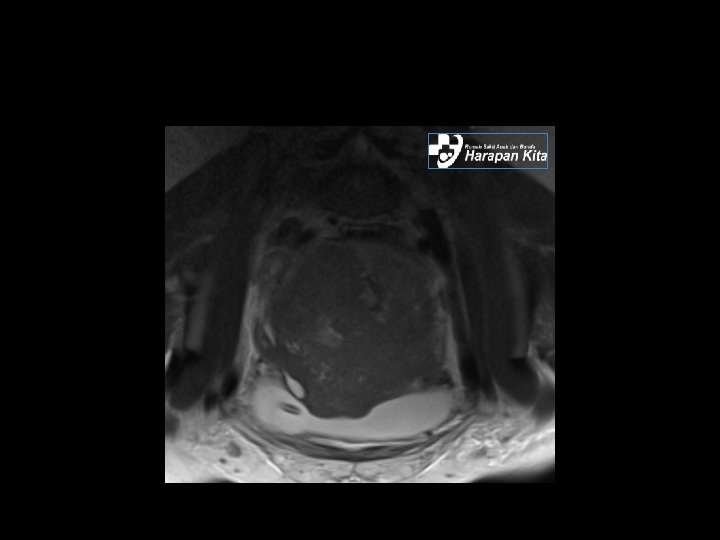
FETAL HEAD & NECK • Neck mass • Cyst / Solid • Extension • Airways obstruction • Neck masses or encephalocele?
FETAL HEAD & NECK MASSES INTRA-ORAL TUMOR Obstetric MR. Melbourne 2017 THYMIC CYST LYMPHATIC MALFORMATION GOITER
FETAL LUNG • Lung volume and maturity • Mediastinal & Diafragm • Masses: MRI differentiates between congenital masses as most have characteristic MRI appearance • CPAM • CDH Pulmonary sequestration Pleural effusion
NORMAL FETAL LUNG Cassidy. Obstetric MR. Melbourne 2017
NORMAL FETAL LUNG
FETAL LUNG: CPAM 32 W GA; type 1 CPAM
One week post-natal chest CT Pathology specimen in concordance with type 1 CPAM
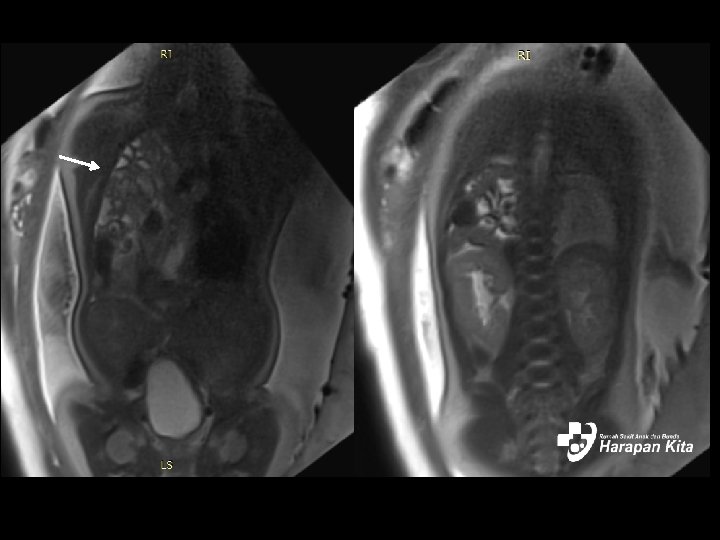
FETAL THORAX: CDH • US: lung tumor? MRI conclude as CDH • MRI differentiate between lung mass and CDH • Characteristic appearance of viscera & bowel
G 1 P 0 A 0, 37 W, SUSP. CDH
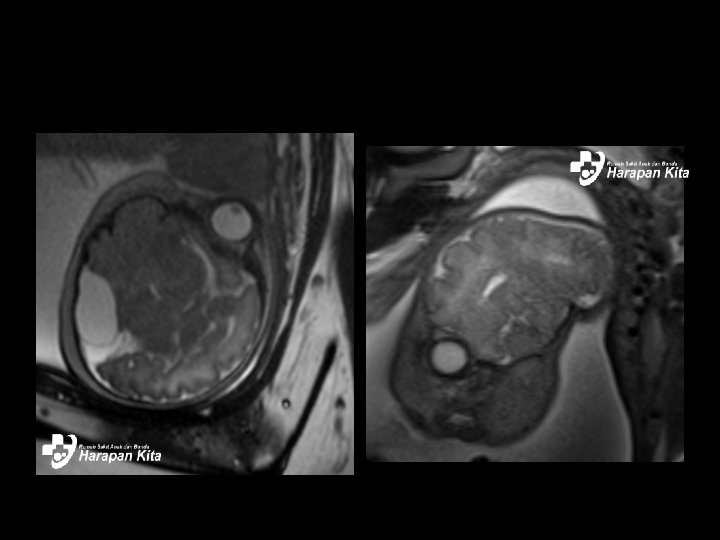
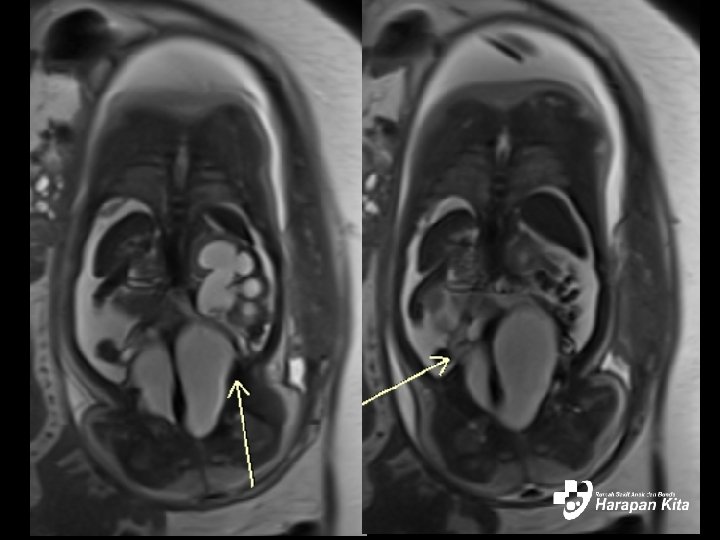
FETAL ABDOMEN-PELVIS • Intestinal obstruction • Complex genital anomalies, fetal syndrome • US: intestinal obstruction? Biliary cyst? • MRI conclude the diagnosis
Esophageal atresia Intestinal atresia, gastroschizis, Meconium peritonitis, ascites
G 5 P 3 A 1, 31 W, GASTRIC-DUODENAL OBSTRUCTION USG: suspected for UVJ obstruction. MRI: Cloacal malformation, hydrocolpos, hidronephrosis, hidroureter. Confirmed by post natal genitography.
G 1 P 0 A 0, 33 W, CLOACAL MALFORMATION USG: suspected for UVJ obstruction. MRI: Cloacal malformation, hydrocolpos, hidronephrosis, hidroureter. Confirmed by post natal genitography.
MRI TWIN PREGNANCY • Complicated twins pregnancy http: //radnet. bidmc. harvard. edu/fetalatlas/gestations/demise. html
WOMEN’S IMAGING: GYNECOLOGIC CASES • Deep Infiltrating Endomeriosis • Placental Adhesive Disorders • Malignancies
DEEP INFILTRATING ENDOMETRIOSIS endometriosis infiltrating the rectum and bladder
DEEP INFILTRATING ENDOMETRIOSIS Rectal Endometriosis
PAD EVALUATION
PREGNANCY WITH MALIGNANCY
THANK YOU