FETAL CIRCULATION IN HEALTH AND DISEASE Characteristics of





![Cardiac output and its distribution Fetal lamb § About 265 ml/mt [60%]passes through ductus](https://slidetodoc.com/presentation_image_h/288967fb98fa871bf782a1c0f7342b0a/image-9.jpg "Cardiac output and its distribution Fetal lamb § About 265 ml/mt [60%]passes through ductus")

































![Cardiac output and its distribution Fetal lamb § About 265 ml/mt [60%]passes through ductus](https://slidetodoc.com/presentation_image_h/288967fb98fa871bf782a1c0f7342b0a/image-44.jpg "Cardiac output and its distribution Fetal lamb § About 265 ml/mt [60%]passes through ductus")































































- Slides: 107
FETAL CIRCULATION IN HEALTH AND DISEASE
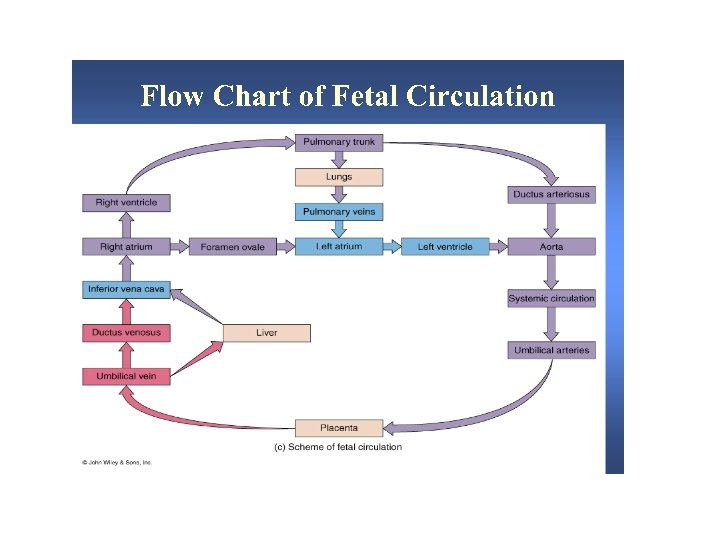
Characteristics of fetal circulatory dynamics § Parallel arrangement of two main arterial systems and their respective ventricles. § Mixing of venous return and preferential streaming. § High impedance and low flow of pulmonary circulation. § Low impedance and high flow of placental circulation. § Presence of shunts.
Cardiac output and its distribution Fetal lamb § § CVO is 450 ml/kg/wt RV ejects 2/3 and LV ejects 1/3 of CVO UV flow is 200 ml/mt/kg [45% of CVO] Of this, 110 ml/mt [24%] passes through DV and 90 ml/mt[21%] passes through hepatic circulation
Cardiac output and its distribution Fetal lamb § Portal venous flow forms 7% and of CVO and abdominal IVC blood forms 30% of CVO. § Total venous return to heart from IVC is 315 ml/mt and represents 70% of CVO. § Of this 115 ml/mt [25% of CVO] passes through FO and 200 ml/mt [44%] passes through TV.
Cardiac output and its distribution Fetal lamb § Venous return to heart from SVC is 90 ml/mt/ and represents 21% of CVO most of this passes through tricuspid valve. § RV ejects about 300 ml/mt or about 66% of CVO. § About 35 ml/mt [8% of CVO] enters the pulmonary circulation
Cardiac output and its distribution Fetal lamb § About 265 ml/mt [60%]passes through ductus arteriosus. § LV ejects 150 ml/kg [ 33% ]. § Of this, 90 ml/mt [20%] distributed to head and upper half and 45 ml/mt [10%]passes through isthmus. § 3% of CVO enters coronary circulation.
60% 20% AA 33% 21% 8% 28 19 18 66% 70% 24 70% 21% 45% 32 55%
65% 50% 65% 55% 35%
Cardiac output and its distribution human fetus § Limited data only is available based on doppler studies. § Umbilical blood flow is 180 ml/mt /kg of estimated fetal weight. § Pulmonary blood flow is estimated to be 75 ml/kg of fetal weight
Cardiac output and its distribution human fetus § CVO appears to be similar to that in lamb, 450 ml/mt/kg fetal weight § Ratio of RV output to LV output is only 1. 2 to 1. 3 as compared to 2: 1 in fetal lamb
140 45 175 15 75 250 200 220 95 125 140 75 180 15 220 40
31 39 10 3 58 17 44 49 31 28 21 17 3 49 39 10
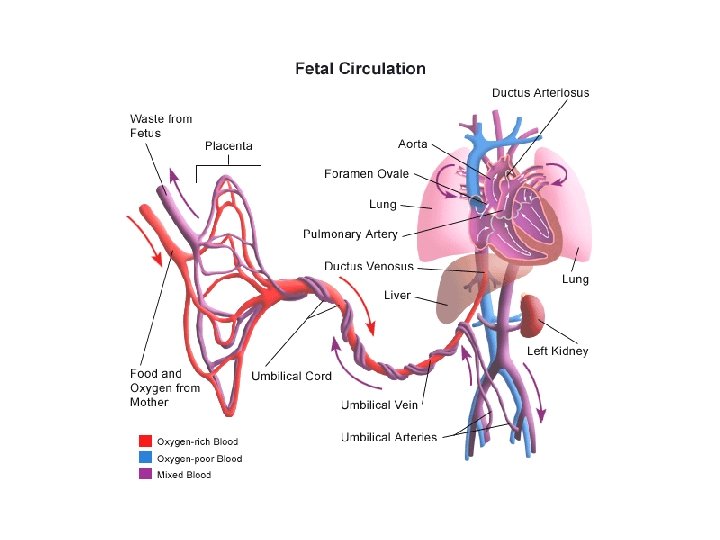
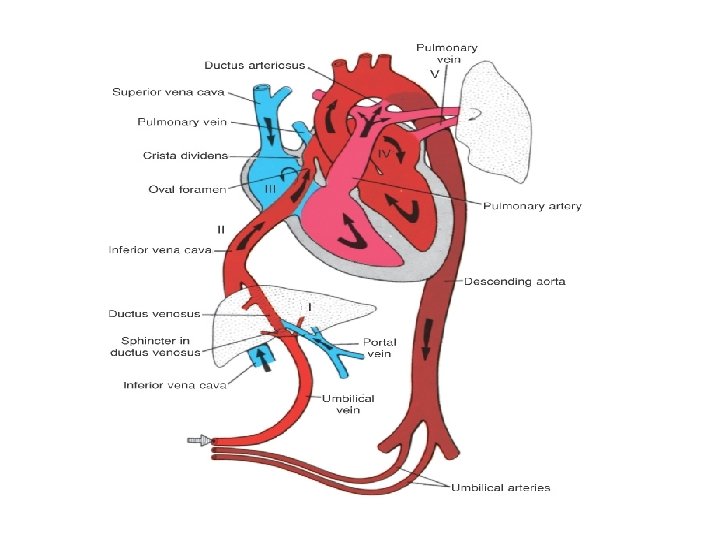
Venous return to heart § Umbilical vein gives branches to left lobe of liver and then divides into DV and arcuate vien. § Arcuate vien joins the portal vein and then gives of branches to right lobe of liver. § Left hepatic vein joins the DV at it’s entry to IVC and Right hepatic vein joins the IVC directly.
Venous return to heart § Right lobe of liver poorly oxygenated portal venous blood and left lobe receives well oxygenated umbilical venous blood. § Both lobes receive small contribution of blood from hepatic artery. § Saturation of RHV is lower than that of LHV.
Venous return to heart § Posterior and left stream of IVC blood carries oxygenated blood while anterior and right stream carries poorly oxygenated blood. § Preferential streaming of DV and LHV blood across the foramen ovale and abdominal IVC and RHV blood across the TV.
Venous return to heart § Eustechian valve helps to direct the IVC blood to cross the foramen ovale. § The lower margin of septum secundum [christa dividens] helps to direct the left posterior stream to preferentially across the foramen ovale. § SVC blood is directed aross the TV.
Shunts in fetal circulation § Ductus venosus § Foramen ovale § Ductus arteriosus or aortic isthmus
Shunts in fetal circulation § The blood returning to heart through venacavae and then redistributed to tissues without being delivered to placenta represents effective R to L shunt. § The blood which passes through DV and then reaches DA and goes to placenta without getting distributed to tissues represent effective L to R shunt. § Combined R to L and L to R shunts forms 33% of CVO.
PULMONARY CIRCULATION § Fetal lung does not serve gas exchange function. § PVR is high and PBF is low. § This helps to reduce workload of fetal heart.
PULMONARY CIRCULATION § MPA continues as Ductus and RPA and LPA arise as branches. § Medial layer is composed of smooth muscle predominantly in small pre acinar and large acinar level arteries. § Further branches have no muscular component.
PULMONARY CIRCULATION § PA pressure rises gradually paralleling the rise in aortic pressure. § TPR falls gradually but this fall when correlated with rise in lung weight, there is actually an increase in PVR towards term. § PBF increases gradually.
PULMONARY CIRCULATION § MPA has forward flow throughout systole with a short period of backflow at end of systole. § DA also has forward flow throughout systole. § BPA has forward flow only through initial one third of systole followed by back flow through rest of systole and diastole. § In humans forward flow is more prolonged.
PULMONARY CIRCULATION § Experiments show fetal PBF increases dramatically in response to increase in maternal PO 2. § This response is evident only in latter part of gestation. § Doppler studies indicate similar changes in humans as well.
PULMONARY CIRCULATION § Fetal pulmonary endothelium behaves in a similar fashion as adult endothelium to vasodilators. § Adrenomedullin has a potent and prolonged vasodilatory effect. § Leukotriens may be responsible for maintaining high fetal PVR.
PULMONARY CIRCULATION § Breathing at birth is associated with a marked fall in PVR and rise in PBF. § PA pressure does not fall as rapidly and remain elevated till the Ductus is widely patent. § Once the ductus is closed, PA pressure can vary independent of systemic pressure.
Oxygen exchange function § Higher hemoglobin level in fetus as compared to mother facilitates oxygen uptake by the fetus in the placenta. § Oxygen dissociation curve of fetal red cells is shifted to left as compared to adult red cells. § Hb. F has less affinity towards organic phosphates like 2, 3 DPG and ATP.
Oxygen exchange function § These phosphates that are present in red cells compete with oxygen for binding to hemoglobin. § Affinity of reduced hemoglobin to 2, 3 DPG is higher than that of oxyhemoglobin and this facilitates oxygen delivery at tissue site. § This is not significant in fetal hemoglobin.
Oxygen exchange function § As CO 2 crosses placenta from fetus to mother, it creates a local acidosis. § In the face of decreasing Ph, mothers hemoglobin shows less affinity towards Hb and oxygen release is enhanced. [Bohr effect] § This supports diffusion of more oxygen across the diffusion membrane to fetus.
Oxygen exchange function § As O 2 is released, maternal Hb acts as a buffer that removes H+ from local environment. § This encourages production of bicarbonate from H 2 O and CO 2 thereby reducing local PC 02 and facilitating diffusion of CO 2 from fetus.
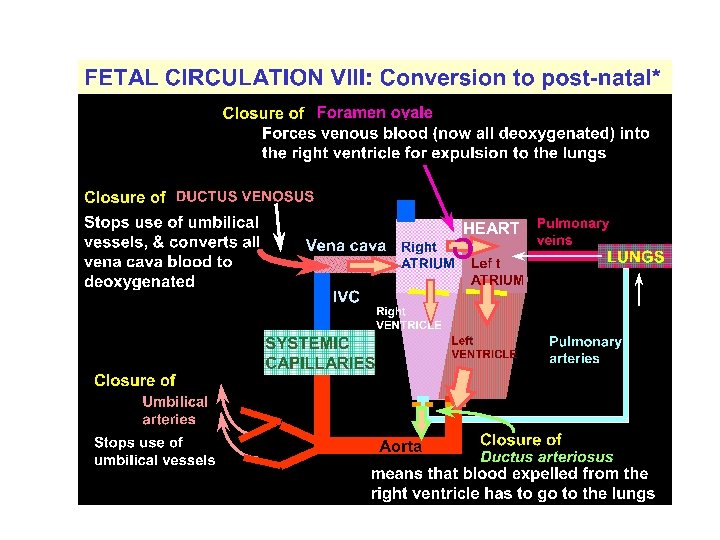
Post natal changes § Gas exchange function is transferred from placenta to the lungs. § Separation of systemic and pulmonary circulations § Increased metabolism to maintain body temperature and hence increased cardiac output.
Post natal changes in various circulatory beds § Coronary Blood flow decreases dramatically as the oxygen content increases. § Cerebral circulation also behaves in the same fashion as coronary circulation.
Post natal changes in various circulatory beds § Skin blood flow is high in utero as the vessels are dilated because the skin is exposed to warm amniotic fluid. § Cutaneous vasoconstriction occurs post natally as evaporation from skin starts. § Cutaneous flow falls and the vascular resistance increaes.
Post natal changes in various circulatory beds § Hepatic blood flow falls rapidly post natally with reduction in umbilical venous return and then increases as the GI flow is re established. § Hepatic blood flow progressively increases after birth and by 7 days after birth reaches a level of 250 ml/minute /100 g by which time there is no flow through ductus venosus.
Changes in Cardiac output § Oxygen consumption increases from 6 -8 ml/mt/kg body weight pre natally to 15 – 20 ml/mt/kg post natally. § CVO of fetal lamb is 450 ml/mt/kg. § C. O of neonatal lamb is 300 -425 ml/mt/kg. So the CVO will be 600 -850 ml/mt/kg. § So the increase is 1. 5 to 2 times.
Changes in Cardiac output Mechanisms § Neonate has to increase the metabolism to increase the body temperature as it is exposed to external temperature. § Improved diastolic function due to removal of compression by maternal organs and uterus causes increased cardiac filling and hence the cardiac output.
Characteristics of fetal circulatory dynamics § Parallel arrangement of two main arterial systems and their respective ventricles. § Mixing of venous return and preferential streaming. § High impedance and low flow of pulmonary circulation. § Low impedance and high flow of placental circulation. § Presence of shunts.
Cardiac output and its distribution Fetal lamb § § CVO is 450 ml/kg/wt RV ejects 2/3 and LV ejects 1/3 of CVO UV flow is 200 ml/mt/kg [45% of CVO] Of this, 110 ml/mt [24%] passes through DV and 90 ml/mt[21%] passes through hepatic circulation
Cardiac output and its distribution Fetal lamb § Portal venous flow forms 7% and of CVO and abdominal IVC blood forms 30% of CVO. § Total venous return to heart from IVC is 315 ml/mt and represents 70% of CVO. § Of this 115 ml/mt [25% of CVO] passes through FO and 200 ml/mt [44%] passes through TV.
Cardiac output and its distribution Fetal lamb § Venous return to heart from SVC is 90 ml/mt/ and represents 21% of CVO most of this passes through tricuspid valve. § RV ejects about 300 ml/mt or about 66% of CVO. § About 35 ml/mt [8% of CVO] enters the pulmonary circulation
Cardiac output and its distribution Fetal lamb § About 265 ml/mt [60%]passes through ductus arteriosus. § LV ejects 150 ml/kg [ 33% ]. § Of this, 90 ml/mt [20%] distributed to head and upper half and 45 ml/mt [10%]passes through isthmus. § 3% of CVO enters coronary circulation.
Cardiac output and its distribution human fetus § Limited data only is available based on doppler studies. § Umbilical blood flow is 180 ml/mt /kg of estimated fetal weight. § Pulmonary blood flow is estimated to be 75 ml/kg of fetal weight
Cardiac output and its distribution human fetus § CVO appears to be similar to that in lamb, 450 ml/mt/kg fetal weight § Ratio of RV output to LV output is only 1. 2 to 1. 3 as compared to 2: 1 in fetal lamb
Venous return to heart § Umbilical vein gives branches to left lobe of liver and then divides into DV and arcuate vien. § Arcuate vien joins the portal vein and then gives of branches to right lobe of liver. § Left hepatic vein joins the DV at it’s entry to IVC and Right hepatic vein joins the IVC directly.
Venous return to heart § Right lobe of liver poorly oxygenated portal venous blood and left lobe receives well oxygenated umbilical venous blood. § Both lobes receive small contribution of blood from hepatic artery. § Saturation of RHV is lower than that of LHV.
Venous return to heart § Posterior and left stream of IVC blood carries oxygenated blood while anterior and right stream carries poorly oxygenated blood. § Preferential streaming of DV and LHV blood across the foramen ovale and abdominal IVC and RHV blood across the TV.
Venous return to heart § Eustechian valve helps to direct the IVC blood to cross the foramen ovale. § The lower margin of septum secundum [christa dividens] helps to direct the left posterior stream to preferentially across the foramen ovale. § SVC blood is directed aross the TV.
Shunts in fetal circulation § Ductus venosus § Foramen ovale § Ductus arteriosus or aortic isthmus
Shunts in fetal circulation § The blood returning to heart through venacavae and then redistributed to tissues without being delivered to placenta represents effective R to L shunt. § The blood which passes through DV and then reaches DA and goes to placenta without getting distributed to tissues represent effective L to R shunt. § Combined R to L and L to R shunts forms 33% of CVO.
PULMONARY CIRCULATION § Fetal lung does not serve gas exchange function. § PVR is high and PBF is low. § This helps to reduce workload of fetal heart.
PULMONARY CIRCULATION § MPA continues as Ductus and RPA and LPA arise as branches. § Medial layer is composed of smooth muscle predominantly in small pre acinar and large acinar level arteries. § Further branches have no muscular component.
PULMONARY CIRCULATION § PA pressure rises gradually paralleling the rise in aortic pressure. § TPR falls gradually but this fall when correlated with rise in lung weight, there is actually an increase in PVR towards term. § PBF increases gradually.
PULMONARY CIRCULATION § MPA has forward flow throughout systole with a short period of backflow at end of systole. § DA also has forward flow throughout systole. § BPA has forward flow only through initial one third of systole followed by back flow through rest of systole and diastole. § In humans forward flow is more prolonged.
PULMONARY CIRCULATION § Experiments show fetal PBF increases dramatically in response to increase in maternal PO 2. § This response is evident only in latter part of gestation. § Doppler studies indicate similar changes in humans as well.
PULMONARY CIRCULATION § Fetal pulmonary endothelium behaves in a similar fashion as adult endothelium to vasodilators. § Adrenomedullin has a potent and prolonged vasodilatory effect. § Leukotriens may be responsible for maintaining high fetal PVR.
PULMONARY CIRCULATION § Breathing at birth is associated with a marked fall in PVR and rise in PBF. § PA pressure does not fall as rapidly and remain elevated till the Ductus is widely patent. § Once the ductus is closed, PA pressure can vary independent of systemic pressure.
Oxygen exchange function § Higher hemoglobin level in fetus as compared to mother facilitates oxygen uptake by the fetus in the placenta. § Oxygen dissociation curve of fetal red cells is shifted to left as compared to adult red cells. § Hb. F has less affinity towards organic phosphates like 2, 3 DPG and ATP.
Oxygen exchange function § These phosphates that are present in red cells compete with oxygen for binding to hemoglobin. § Affinity of reduced hemoglobin to 2, 3 DPG is higher than that of oxyhemoglobin and this facilitates oxygen delivery at tissue site. § This is not significant in fetal hemoglobin.
Oxygen exchange function § As CO 2 crosses placenta from fetus to mother, it creates a local acidosis. § In the face of decreasing Ph, mothers hemoglobin shows less affinity towards Hb and oxygen release is enhanced. [Bohr effect] § This supports diffusion of more oxygen across the diffusion membrane to fetus.
Oxygen exchange function § As O 2 is released, maternal Hb acts as a buffer that removes H+ from local environment. § This encourages production of bicarbonate from H 2 O and CO 2 thereby reducing local PC 02 and facilitating diffusion of CO 2 from fetus.
Post natal changes § Gas exchange function is transferred from placenta to the lungs. § Separation of systemic and pulmonary circulations § Increased metabolism to maintain body temperature and hence increased cardiac output.
Post natal changes in various circulatory beds § Coronary Blood flow decreases dramatically as the oxygen content increases. § Cerebral circulation also behaves in the same fashion as coronary circulation.
Post natal changes in various circulatory beds § Skin blood flow is high in utero as the vessels are dilated because the skin is exposed to warm amniotic fluid. § Cutaneous vasoconstriction occurs post natally as evaporation from skin starts. § Cutaneous flow falls and the vascular resistance increaes.
Post natal changes in various circulatory beds § Hepatic blood flow falls rapidly post natally with reduction in umbilical venous return and then increases as the GI flow is re established. § Hepatic blood flow progressively increases after birth and by 7 days after birth reaches a level of 250 ml/minute /100 g by which time there is no flow through ductus venosus.
Changes in Cardiac output § Oxygen consumption increases from 6 -8 ml/mt/kg body weight pre natally to 15 – 20 ml/mt/kg post natally. § CVO of fetal lamb is 450 ml/mt/kg. § C. O of neonatal lamb is 300 -425 ml/mt/kg. So the CVO will be 600 -850 ml/mt/kg. § So the increase is 1. 5 to 2 times.
Changes in Cardiac output Mechanisms § Neonate has to increase the metabolism to increase the body temperature as it is exposed to external temperature. § Improved diastolic function due to removal of compression by maternal organs and uterus causes increased cardiac filling and hence the cardiac output.
Changes in Cardiac output Mechanisms § Perinatal but not post natal increase in thyroid hormones is the principal mechanism for increase in cardiac output. § Improvement in myocardial growth and maturation brought about by cortisol may also play important role.
Changes in hemoglobin and tissue oxygen delivery § Human new born has a high hemoglobin level (about 16 g/dl) so that the oxygen carrying capacity is quiet high and the total amount of oxygen transported to tissues is quiet high. § Since the Hb F levels are still high facilitation at tissue site is not as great as in adults. § Over the first 8 -10 weeks after the birth, Hb concentration falls to 10 -11 g/dl. This is accompanied by loss of Hb F and almost 100% is adult type.
Regulation of fetal circulation § Arterial baroreceptors are funtional in fetus from early in the gestation § Near term, it is as sensitive as adults in fetal lambs. § Chemoreceptors are active only in latter part of gestation.
Fetal circulation in pathological conditions
Fetal circulation in pathological conditions § Development of a structural abnormality will modify the fetal circulation. § This will affect the development of other components and can lead to other defects. § The impact of a defect will depend on it’s severity and time of gestation at which it occurs.
Fetal circulation in pathological conditions § Many of the defects, though it modifies the circulation, will not significantly affect fetal perfusion and hence the growth and development. § This is because of the presence of shunts and mixing of blood. § Fetus tolerates the obstructive lesions very much. § Fetal circulation is jeopardized by regurgitant lesions and myocardial disease.
Septal defects § They in general do not modify the fetal circulation significantly. § VSD may have a transient left to right shunt in systole. § In OP ASD, due to close proximity of defect with TV, more than normal amount of SVC blood may enter the LA.
Septal defects § In atrioventricular septal defects, the obligatory flow from LV to RA will result in decrease in LV output and an increase in RV output. § This will reduce the flow across the isthmus and can predispose to coarctation. § It is the degree of severity of AV valve lesion and regurgitation which will determine the outcome.
LVOT Obstruction § Severe obstruction developing early result in a small LV with an increased mass. § RV is able to compensate fully if LVOTO develops slowly.
LVOT Obstruction § SVC flow courses normally. § Majority of IVC blood flow crosses TV to RV. § Flow across the ductus increases. § PBF has higher than normal saturation.
LVOT obstruction § Decrease in saturation between DA and AA. § LV systolic pressure increases slightly but not EDP. § A retrograde flow in arch and ascending aorta indicates severe obstruction.
62 75/50 75/4 65 60 90/ 5 60 70/45 70
Aortic arch abnormalities § Most of the alteration in the circulation are due to co existing intra cardiac defects. § Common features are, reduced flow in to ascending aorta, increased flow in to the pulmonary trunk and greater proportion of CVO carried across ductus to descending aorta. § The decreased volume loading of LV may possibly interfere with it’s development.
Mitral and aortic atresia § All blood must pass through RV and ductus has to provide for both AA and DA blood flow. § Complete mixing of blood occurs in RA and saturation in PA, AA and DA are all same. § If the foramen ovale is sufficiently large and ductus accomodates whole of systemic blood flow, there will be no significant interference with intrauterine development and survival.
70/40 60 70/2 60 40 70 60
Mitral and aortic atresia § If the foramen ovale is restrictve, severe pulmonary venous hypertension develops. § If the ductus does not enlarge to accommodate the whole of systemic blood flow increased blood flow to lungs and pulmonary hypertension develops. § Both these can lead to increased development of smooth muscle in the pulmonary vasculature.
RVOTO with intact IVS § In rapidly developing RVOTO, RV and LV cannot compensate for and the CVO falls. § If RVOTO developing slowly, both LV and RV can compensate for and CVO is maintained. § In pulmonary atresia, total cardiac output is carried by the left heart.
63 63 63 100/4 63 70/3 40 70
RVOTO with intact IVS § In pulmonary atresia, all systemic venous blood is carried to left side through foramen ovale and all blood supply to DA is provided through isthmus. § Larger than normal foramen ovale, left sided chambers, AA and aortic isthmus.
RVOTO with intact IVS § If severe RVOTO develops early in gestation, the flow through the ductus is reversed and carries only 8 to 10 % of cardiac output. § The ductus will be narrower and will make an acute inferior angle with aorta. § The ductus will remain patent for longer than normal duration.
RVOTO with intact IVS § If the fetus develops significant TR, RV pressure remains low and myocardial sinusoids and coronary fistulae do not develop. § If TR does not develop, significant RV systolic pressure develops and if occurs early in gestation, intramyocardial sinusoids and coronary fistulae develop.
TAPVC § Usually does not affect the development of fetus. § If whole of PV return drains to SVC, LV will be totally free of PV blood and hence will be of higher saturation. § Left atrium and left ventricle will be relatively small in TAPVC.
TOF and related disorders § Does not appear to affect fetal circulation adversely. § The volume and direction of flow across the PA and ductus are dependant on the severity of obstruction. § Total flow through the ductus will be reduced considerably.
TOF and related disorders § This can markedly reduce the diameter of fetal ductus and also reduce the development of smooth muscle in it’s wall. § If blood flows from aorta to PA in fetal life, the orientation of ductus changes and it forms an acute inferior angle with aorta. § AA and the isthmus carries large than normal amount of blood and they tend to be larger.
70/45 63 60 70/4 65 55 70 70/4
TOF with absent PV § Ductus is frequently either atretic or not developed. § RV would be subjected to both volume and pressure overload and can develop in utero. § Significant pulmonary regurgitation can seriously affect perfusion of pulmonary vessels and cause abnormal development of intrapulmonary vessels.
Aortopulmonary transposition § Compatible with fetal survival and normal intrauterine development. § Does not affect the pattern of venous return. § Blood with higher oxygen saturation will go to lungs. This will reduce the PVR and hence increase in PBF.
Aortopulmonary transposition § This will reduce the blood flow across the ductus and increases the flow across the isthmus. § Blood with lower oxygen saturation perfuses coronary and cerebral circulation. § Hence cerebral and coronary blood flow are increased considerably.
70/45 55 70/45 65 70/4 55 40 70 70 70/3
TGA with VSD § Bi directional shunting occur depending on after load of each ventricle. § The difference in saturation between AA and DA will be lesser.
TGA with VSD and PS § Almost complete admixture of SVC and IVC streams in RV. § AA and DA will have similar oxygen saturations. § Blood flow in the ductus will be from aorta to PA.
70/45 65 65 70/4 55 40 70 65
Truncus arteriosus § Various degree of mixing occurs just above the semilunar valve. § Degree of mixing depends on morphology. In type 1, there is differential streaming of blood and in others there will be complete mixing. § Ductus is usually small or absent and increased flow traverses through isthmus and it is large.
Ebstein’s anomaly § Severe TR can manifest as in utero cardiac failure especially if foramen ovale is restrictive. § Marked enlargement of RA and atrialised RV can cause septal displacement and compromise LV output. § Functional pulmonary atresia can result and ductal flow may be reversed.
Ebsteins anomaly § Marked enlargement of right atrium can cause pulmonary hypoplasia § Severe TR alters the preferential drainage of venacaval blood and causes complete mixing of blood in right atrium.
Tricuspid atresia § All of the venous return traverses foramen ovale and it is considerably larger than normal. § Complete admixture of blood in the left atrium § It is compatible with normal intrauterine development and survival.
Tricuspid atresia § If IVS is intact, whole PBF is from aorta through ductus and ductal flow is lesser than normal. § 75% of combined VO traverses the isthmus and it tends to be larger. § In the presence of VSD, the flow pattern is decided by the size of the defect and presence of pulmonary stenosis.