FERTILIZATION TILL FORMATION OF GERM LAYERS Fertilisation Fertilisation








 �The")





 on dorsal surface of epiblast")


 Neural")






- Slides: 25
FERTILIZATION TILL FORMATION OF GERM LAYERS
Fertilisation � Fertilisation is the union of the male and female gametes. It is pertinent to note that the female gamete has not completed the second meiotic division at the time of release from the ovary, and should be correctly called an oöcyte. In the adjoining picture note that its is surrounded by a thick ‘wall’ called the zona pellucida (‘clear zone’). This is in turn surounded by a layer of supporting cells forming a ‘crown’, the corona radiata. At this stage the zona pellucida also includes the polar body formed at the end of meiosis I (not shown in this picture). � Fertilisation most commonly takes place in the ampulla of the uterine tube. Zona pellucida Corona radiata
Fertilisation Acrosome At the tip of the sperm head is an enzyme-containing structure called acrosome. Acrosomal enzymes allow the sperm to ‘bore’ through the zona pellucida. The entry of one sperm causes a molecular reaction in the zona pellucida which prevents the entry of any other sperm. The entry of the sperm is also followed by the completion of the second meiotic division and a second polar body is formed. The ovum now has two ‘pronuclei’ male and female. These soon lose their nuclear membranes and a diploid cell is formed, called the zygote. These events are shown in the next slide where the polar bodies are also shown.
Fertilisation thus has some ‘consequences’ : • • Restoration of diploidy Chromosomal sex determination Completion of meiosis II in the oöcyte Initiation of the first cell division (cleavage)
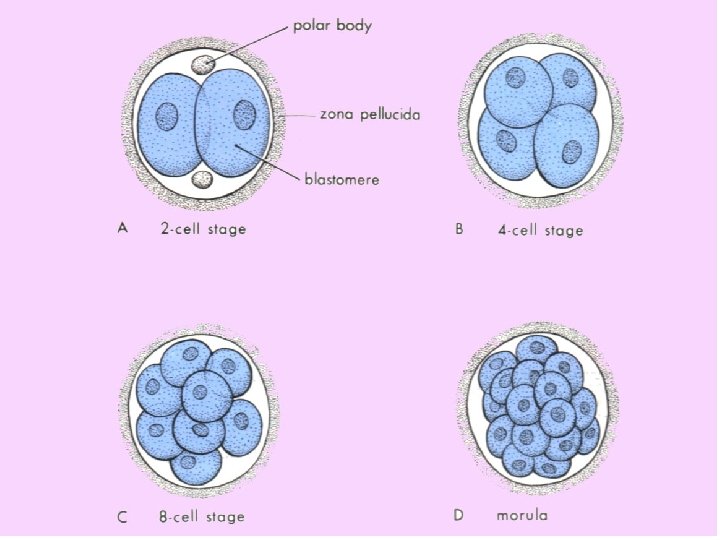
CLEAVAGE Important points Definition: one cell divides into 3 cell stage then into 4 cell, 5 cell stage etc. this process of subdivision of fertilized ovum is called cleavage 2 daughter cells are still surrounded by the zona pellucida Each daughter cell is much smaller than the ovum As subcequent divisions, the cell becomes smalller and smaller until they acquire the size of most cells of the body
Cleavage, Morula and the Blastocyst � The fertilised ovum or zygote has a very large cytoplasmic volume. During the first few divisions separation of chromatids of replicated chromosomes follows the same pattern of mitosis, but the cytoplasm does not increase. The division of cytoplasm in fact reduces the cytoplasmic volume in daughter cells. � These divisions lead to a group of cells that collectively appear like a mulberry and called as the morula. Soon a cavity appears in the cell mass which now is called the blastocyst. In the blastocyst we see two groups of cells – a smaller ‘inner cell mass’ destined to become the embryo proper and an outlying layer which later forms the tissues that connect the embryo and the foetus to the mother. This cell layer is known as the trophoblast. � The zona pellucida persists almost throughout these stages while the cell mas is slowly propelled towards the uterus by the action of cilia in the epithelium of the uterine tube. � The persistence of the zona pellucida is a factor in preventing the implantation of the embryo in the wall of the tube. This is important as the trophoblast is highly invasive in nature. � These stages are illustrated in the next two slides.
Blastocyst �Inner cell mass �Trophoblast �Zona pellucida disappears �Implantation • • • Implantation is the process of embedding the embryo in the uterine wall. Disappearance of the zona pellucida and the invasive nature of trophoblastic tissue are the major factors in implantation. The second picture shows significant changes in the embryo – these are explained in the next two slides.
Fertilization to Implantation
Week 1 post conception �Zygote divides repeatedly moving down tube toward uterus (cleavage) �The daughter cells are called blastomeres �Morula: the solid cluster of 12 -16 blastomeres at about 72 hours �Day 4: late 60 cell morula enters uterus, taking up fluid becoming blastocyst
Blastocyst stage _____inner cell mass ______trophoblast �Two distinct types of cells �Inner cell mass: forms the embryo �Trophoblast: layer of cells surrounding the cavity which helps form the placenta �Floats for about 3 days �Implantation on about day 6 post conception � Trophoblast erodes uterine wall � Takes 1 week to complete �If inner cell mass of a single blastocyst divides: monozygotic (identical) twins
Week 2 Inner cell mass divides into epiblast and hypoblast 2 fluid filled sacs Amniotic sac from epiblast Yolk sac from hypoblast Bilaminar embryonic disc: area of contact (gives rise to the whole body)
Implantation and beyond… � First of all, notice the nature of the endometrium : � A : surface epithelium, B : connective tissue, B C � C : glands. � Implantation is said to be complete when the surface epithelial layer of the uterus regains its continuity over the embryo. � Trophoblast has now differentiated into two parts: B � D : cytotrophoblast – cell boundaries are clear. A � E : syncytiotrophoblast – cell boundaries have D disappeared. (Syncytium = ‘cells together’). � A part of these trophoblastic masses will form the placenta. � The embryo itself has two layers called the epiblast (F) and the hypoblast (G). � Two cavities appear around the embryo –one on the epiblast side : amniotic cavity, that on the other side is the yolk sac. The epiblast continues as the amnion (an epithelial layer) around the amniotic cavity. F G The E terms epiblast and hypoblast are introduced here to make the description cohesive and complete. The concepts introduced in the next slide are more important.
Trilaminar Embryo In surface view, the embryo appears as a flat disc with the future head and tail ends established. At the tail end, cells of the epiblast begin to migrate as indicated by the curved arrows in the sectional view below. The site of this migration is seen as the ‘primitive streak’. This migration establishes the final three layers of the embryo – ectoderm, mesoderm and endoderm (entoderm). Embryonic disc Yolk sac The core concepts here are : 1. From the inner cell mass, a trilaminar embryo emerges. 2. The amnion is continuos with the ectoderm and encloses the amniotic cavity. Embryonic disc, Top view Head end Embryonic disc, Sectioned along this line Primitive streak The hypoblast is replaced by the endoderm and the yolk sac also changes its nature. However, you may overlook this detail!
Week 3 �Bilaminar to trilaminar disc �Three primary “germ” layers: all body tissues develop from these �Ectoderm �Endoderm �Mesoderm
Formation of the 3 “germ” layers Primitive streak (groove) on dorsal surface of epiblast Grastrulation: invagination of epiblast cells Days 14 -15: they replace hypoblast becoming endoderm Day 16: mesoderm (a new third layer) formed in between Epiblast cells remaining on surface: ectoderm
The three “germ” tissues �“Germ” as in germinate, not germs �Early specialization of cells �Are precursors �Ectoderm and endoderm are epithelial tissue (form sheets of tissue) �Mesoderm is a mesenchyme tissue �Mesenchyme cells are star shaped and do not attach to one another, therefore migrate freely
Notochord Days 16 -18 Primitive node epiblast cells invaginate and migrate anteriorly with some endoderm cells Rod defining the body axis is formed Future site of the vertebral column
Neurulation Notochord signals overlying ectoderm Formation begins of spinal cord and brain (neurulation) Neural plate to neural groove to neural tube: pinched off into body
Closure of neural tube: begins at end of week 3; complete by end of week 4 (folic acid important for this step) Extends cranially (eventually brain) and caudally (spinal cord) Neural crest, lateral ectodermal cells, pulled along and form sensory nerve cells and other structures
�Mesoderm begins to differentiate �Lateral to notochord, week 3 �Extends cranially and caudally (from head to tail or crown to rump) �Division of mesoderm into three regions �Somites: 40 pairs of body segments (repeating units, like building blocks) by end week 4 �Intermediate mesoderm: just lateral to somites �Lateral plate: splits to form coelom (“cavity”)
Divisions of the mesodermal lateral plate �Somatic mesoderm: apposed to the ectoderm �Splanchnic mesoderm: apposed to the endoderm �Coelom in between will become the serous cavities of the ventral body cavity: �Peritoneal �Pericardial �Pleural
Major derivatives of the embryonic germ layers
Salient Landmarks � We now attempt to place some of these events on an approximate timescale, � � � � bearing well in mind that there are bound to be a few variations. We might as well consider the beginning of this story at the moment of ovulation. Both the sperm and the oöcyte have a finite period of viability. The oöcyte degenerates after a day or so from ovulation if not fertilised, the sperm lives for about three days. We might say that in the ideal case fertilisation takes place within 12 to 24 hours of ovulation. By 30 hours the first division is complete (two cell stage). 12 to 16 cells are seen by the third day, and in 4 days a well-formed morula is in the uterine cavity. By day 5, the blastocyst stage is evident and the zona pellucida has disappeared (also described as the hatching of the blastocyst!). Implantation begins by day 6 and is completed between days 8 and 10. Between the 14 th and 18 th day we see the appearance of the primitive streak and the formation of the trilaminar embryo. By the end of the third week the formation of the neural tube is well established and somites begin to appear. This timeline is not intended for memorising individual dates! Some key concepts emerge from this account. These are elaborated next.
Some Clinical Correlates A key event of great concern from the mother’s point of view is the time and site of implantation. Though we have considered ovulation as the starting point of the story, subsequent events are more accurately timed as after fertilisation. When the conceptus reaches the blastocyst stage, the zona pellucida disappears and the invasive activity of the trophoblast begins. If this happens before the embryo reaches the uterus, implantation occurs in the tube. The tube is not equipped to handle the growing embryo. Implantation in the tube therefore invariably causes rupture of the tube or the death of the embryo. In the latter case the dead embryo is simply aborted, but the rupture of the tube is a potential emergency. In rare cases implantation may occur on the surface of the ovary or even in the peritoneal cavity (the oöcyte is released in the peritoneal cavity whence it is picked up by the fimbriae of the tube). In exceptional cases a peritoneal implantation may even reach full term. The commonest (and the ideal) site of implantation is the fundus or the upper part of the body of the uterus. In this case the trophoblast forms a placenta which is attached to the same part of the uterus. Too late an implantation may occur in the lower part of the uterus, in which case the placenta may be placed across the inner opening of the cervix. Distention of the uterus in the later part of pregnancy may cause premature separation of the placenta with bleeding that threatens both the foetus and the mother.