Femoral Artery Access Using Landmarks and Fluoroscopy Zoltan
































- Slides: 33
Femoral Artery Access Using Landmarks and Fluoroscopy Zoltan G Turi MD, MSCAI Seton Hall University School of Medicine Hackensack University Medical Center
Disclosure Statement of Financial Interest Zoltan Turi MD, MSCAI Clinical Events Committee - Mitralign Research Support - Abbott Vascular Training Grant Support - Abbott Vascular, Medtronic
Step 1 Recognize That Vascular Access in the New Percutaneous Technologies Era is: Taken for Granted Under-investigated but Way Over-represented in Complications
TAVR Complications NEJM 2010
Usual Approach • Keep poking until you get a gusher
Step 2 – Choose a Landmark 3. Bone landmarks X 2. Maximal pulsation 4. Prior puncture site 1. Inguinal crease X
Landmarks Used for Femoral Puncture All Three 1% Skin Crease Maximum Pulse Bony Landmarks Pulse/Bone 7% Crease/Bone 1% Crease/Pulse 13% Crease 40% Bone 13% Pulse 25% Skin Crease Most Common Grier D. Br J Radiol 1990; 63: 602.
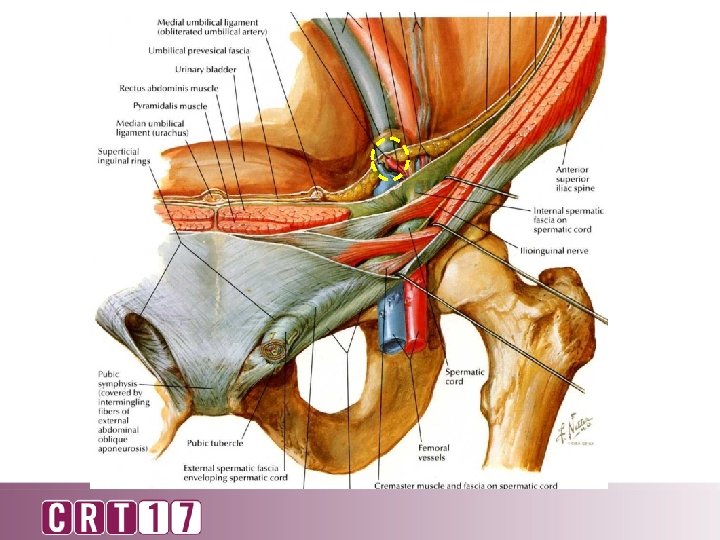
Inguinal Crease UC San Diego New Jersey
This is NOT Normal Anatomy CFA PFA SFA 3 Misconceptions despite 60 years experience
Stick at the crease • Right at the inguinal crease • Steep angle of attack • Some difficulty with inserting sheath over wire
PFA
Odds Ratio RPH 18: 1
Femoral Artery Anatomy: A Prospective Study • 200 consecutive patients • All undergoing coronary angiography • Femoral angiography at end of procedure • Quantitative angiography Schnyder et al CCI 2001
Femoral Head and the CFA Bifurcation 1. 5% 4. 0% 17% V 55. 5% IV 22% III II I I: III: IV: V: Number of patients 111 44 34 8 3 Below inferior border At inferior border Below center of head At center of head Above center of head n=200
Femoral Angiogram LAO RAO
Common Femoral Artery – Classic Measurements • From top of femoral head to femoral bifurcation • Does not take IEA into consideration • Does not consider implications of CFA stick above bifurcation, but below femoral head
Target Zone
Centerline Target Zone TYPE 1
TYPE 2 Centerline Target Zone
Cumulative Probability of Being Outside Target Zone Above FH Centerline Below
IEA FH Centerline Cumulative Target Zone BIF
Step 3 – Iterative Fluoroscopy
N=296
Fluoro guidance is not just using a hemostat 56% Abu-Fadel CCI 2009
How to Decrease Risk of Complications 1. Access using fluoroscopy and/or ultrasound 2. Needle entry below centerline of femoral head 3. Femoral angiogram regardless of closure device use 4. Proceed to PCI (and anticoagulate) only if puncture in safe zone
How to Decrease Risk of Complications 1. Access using fluoroscopy and/or ultrasound 2. Needle entry below centerline of femoral head 3. Femoral angiogram regardless of closure device use 4. Proceed to PCI (and anticoagulate) only if puncture in safe zone
How to Decrease Risk of Complications 1. Access using fluoroscopy and/or ultrasound 2. Needle entry below centerline of femoral head 3. Femoral angiogram regardless of closure device use 4. Proceed to PCI (and anticoagulate) only if puncture in safe zone
How to Decrease Risk of Complications 1. Access using fluoroscopy and/or ultrasound 2. Needle entry below centerline of femoral head 3. Femoral angiogram regardless of closure device use 4. Proceed to PCI (and anticoagulate) only if puncture in target zone
How to Decrease Risk of Complications 1. Access using fluoroscopy and/or ultrasound 2. Needle entry below centerline of femoral head 3. Femoral angiogram regardless of closure device use 4. Proceed to PCI (and anticoagulate) only if puncture in target zone 5. Use micropuncture
Step 4 – Micropuncture • Micropuncture
The Way To The Heart Is Through The Wrist: Radial Catheterization Comes To America (Finally)