Female pelvis Consist of four bones 2 hip


Female pelvis • Consist of four bones: - 2 hip bones - Sacrum - coccyx

Hip bone • Ilium • Ischium • Pubic bone

Pelvic brim oval shape , transverse diameter > AP diameter canal , , , circular , AP=transverse outlet , AP> T Formed from : 1. Sacral promontory. Anterior and upper part of 1 st sacral vertebra. 2. Ileopectineal line. Line that runs downward and forward around the inner surface of the ilium. 3. symphysis pubis Joint bet. Bodies of pubic bone. Pelvic brim divides the pelvis into two parts a true pelvis (below the brim –smaller , more important) and a false pelvis ( above the brim-larger).
: §")
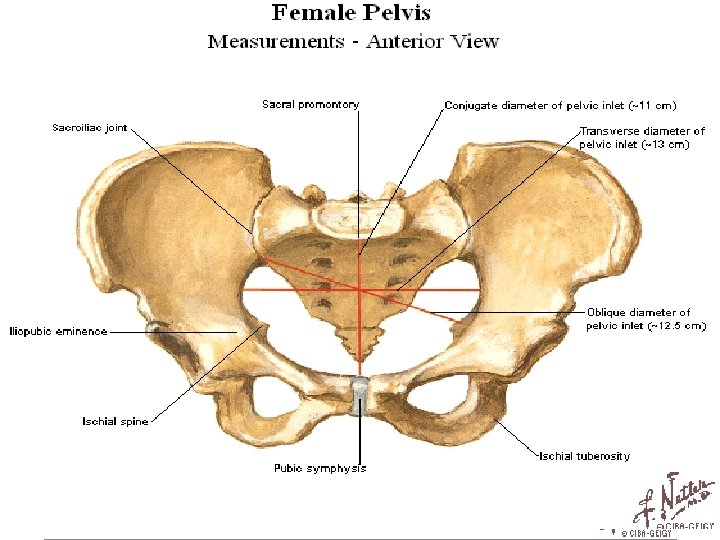
True pelvis Has inlet , a cavity & outlet. Pelvic inlet (pelvic brim): § Posterior: sacral promontory + ala of sacrum. § Lateral: Ileopectineal line. § Anterior: Symphysis pubis and pubic crest. Pelvic Cavity: § Lies bet. Inlet and outlet. § Short and curved.
 Outlet: § Posterior: The Coccyx. § Lateral: Ischial tubrosity. §")
True pelvis (cont. ) Outlet: § Posterior: The Coccyx. § Lateral: Ischial tubrosity. § Anterior: Pubic arch.

Pelvic inclination • Angle of the brim is 600 in the erect position. Inerect = angle of inclination • In Afro-caribbean women this angle may be 900. -more difficult delivery - this increase angle may delay the head entering the pelvis in labour. ’ – more difficult to descend Decrease in angle = decrease difficulty to descend

• Most tight part of pelvis is the transverse diameter • How we assess pelvis clinically ? 1. sacral curvature / angle of inclination 2. pubic angle 3. interspinous diameter
 Spine lordotic=increase 2) 2. abnormality in pelvic Downward")
Angle of inclination = 60 1) Spine lordotic=increase 2) 2. abnormality in pelvic Downward and backward Sacral curvature Pelvic axis

• Pelvic inclination angle is the angle of between pelvic inlet and horizontal plane.
 11 cm. -not")
Pelvic diameters Pelvic inlet: • True conjugate diameter of inlet (A-P) 11 cm. -not enter it ? Thick bones + fascia/muscles • Obstetric conjugate diameter ( about 10 cm)- the baby enters through it – (TC-Thick fascia. muscle) • Diagonal conjugate diameter 13 cm ( you can examine it by digital vaginal examination towards promontrory of sacrum ) with lower border of symphysis pubis , 2 or 2. 5 bigger than obstetric – if got through it it can get through any other diameter - very difficult to enter fingers , but if we could = very small pelvis / if couldn’t = more likely adequate • Transverse diameter (about 4 cm in front of the promontory) 13. 5 cm • Oblique diameter 12. 5 cm. Transverse + oblique not important

Pelvic mid-cavity Area bounded : • Infront: Middle of the symphasis pubic. • Each side: -Pubic bone. - obturator fascia - inner aspect of isch. bone and spines. • posterior: Junction of 2 nd and 3 rd sacral vertebra. The A-P diameter is around 11. 5 cm. To equal diameter but projecting spine because it will norrow them , the smallest ever =10. 5

Pelvic mid-cavity • The cavity almost round. ( Transverse and anterioposterior diameters are similar 12 cm). • Ischial spines are palbable vaginally. • Interspinous diameter: 10 cm. Clinical importance of ischial spines: 1. landmark to assess the descend of of the haed on vaginal examination. 2. landmark for providing an anaesthetic block to the pudendal nerve. (medial and below the spine).

Pelvic outlet
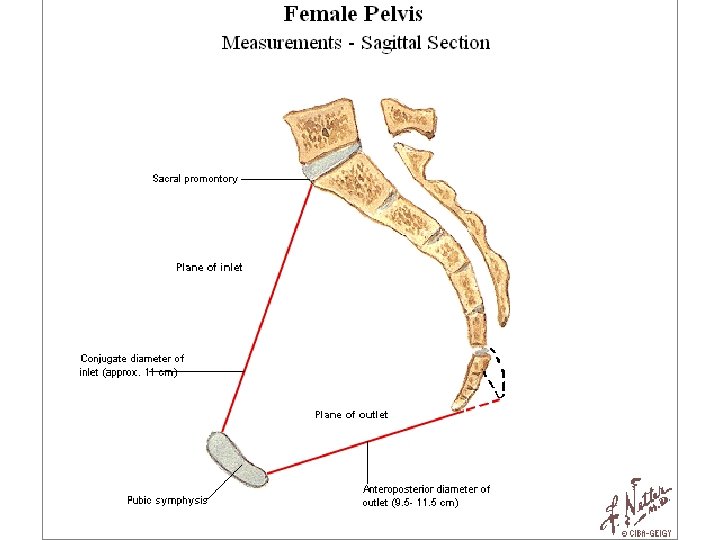

Pelvic outlet • Consists of two triangular areas having the same base ( intertuberous diameter). • The A-P diameter 12 -13 cm • The transverse diameter (Intertuberous diameter) 10. 5 - 11 cm

varieties of female pelvis • Gynecoid: 50 % of women. • android : 33% of women • anthropoid : 24% white females 41% black females • Platypelloid : 2% of women •

Gynecoid pelvis

Android pelvis male funnel-shaped pelvis , contracted outlet INLET 1. Heart shaped AP>T 2. Bones are not parallel to each other OUTLET Intertuberous <AP diameter The head of it can pass the inlet then it can pass to outlet 3. Pubic arch more acute

Anthropoid pelvis long, narrow, oval shaped large pelvic in shape of android –no problem

Platypelloid Pelvis Wide pelvis, flattened at the brim, promontory pushed forward large pelvic in shape of gynecoid –no problem

Fetal skull Ovoidal in shape 1. vault: extends from the supra-orbital ridges to the nape of the neck. 2. face: from the root of the nose to the junction of the head and neck. 3. Base. The best method to diagnose cephalopelvic disproportion is by delivery Why we concentrate on head not body ? In body no moulding just minimum reduction // in head – moulding For best engagment ? Longitidual > transverse >>more flexed = ﺑﺎﻟﻄﻮﻝ Deflexed = ﺑﺎﻟﻌﺮﺽ Fully extended = ﺑﺎﻟﻄﻮﻝ

Fetal skull Grades of moulding : Grade 0 = suture lines between bones Grade 1 = obliterate suture lines but with direct contact Grade 2= can be returned to normal Grade 3= can’t be returned

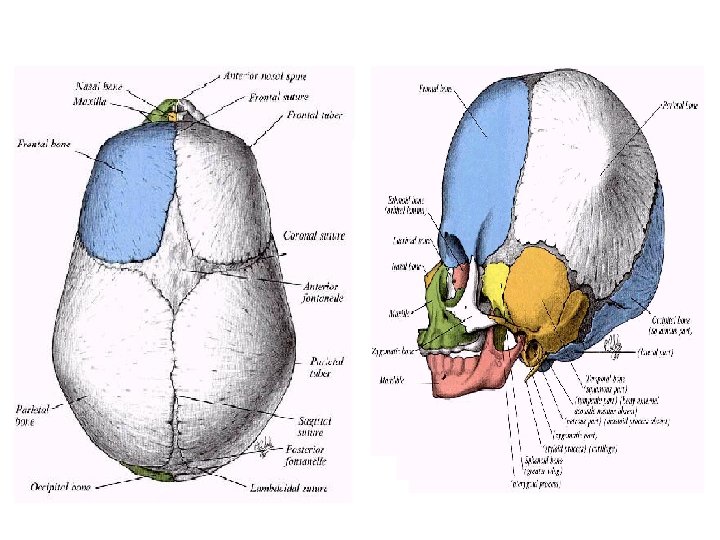
Fetal skull • Compared to an adult skull it has large cranium relative to the face • Most bones are incompletely ossified : > vault bones: ossify in membrane > base bones: ossify in cartilage During parturition bones can be displaced to the extent that they overlap each other at the sutures 1)'moulding‘. 2) Also the pelvic bones dilate through symphysis and sacroiliac bones
 : 4 sutures Diamond-shaped,")
Disappear with moulding G 2, 3 The anterior fontanelle (Bregma) : 4 sutures Diamond-shaped, lies in between the 2 halves of the frontal bone and the 2 parietal bones (junction of the sagittal , frontal and coronal sutures). The fibrous membrane forming its floor is replaced by bone and closed by 18 months of age

The posterior fontanelle: Triangular in shape, lies between the 2 parietal bones in front and the occipital bone behind (junction of sagittal suture and lambdoidal sutures). Closed by the end of 1 st year.

THE VERTEX: Is the area bounded by the 2 parietal eminences and the anterior and posterior fontanelles

Longitudinal diameters of fetal head Mentovertical is very difficult – no diameter allows passage , so CS

Longitudinal diameters of fetal head 1. suboccipito- bregmatic: well-flexed foetal head in vertex presentation. 2. suboccipito-frontal: from sub-occipital region to forehead prominence (10 cm) less well-flexed head in OP position. 3. occipito-frontal: more extension. 4. occipito-mental(mento-vertical): greatest longitudinal diameter that may present = Brow presentation. too large to pass through normal pelvis 5. submento-bregmatic : more extension but less diameter. face presentation

Head presents on delivery depending on flexion of the head (the longitidual diameter that passes through ) VERTEX = well flexed /partially flexed (occipitofrontal ) >>suboccipito bregmatic =9. 5 Biparietal =9. 5 Sinciput =deflexed=Brow FACE=extended =submentobregmatic Vertex /SOB/wellflexed OP/SOF/partial Brow/OM/deflexed Face/SMB/extended

Transverse diameters of fetal head Smaller than all pelvis diameter except interspinous
- Slides: 33