FEMALE GENITAL MUTILATION health issues for childbearing women

FEMALE GENITAL MUTILATION: health issues for childbearing women Stephanie Reed UW School of Nursing

Outline § Sufia: A Case Presentation § Anatomy of FGM § Prevalence: globally and locally § Social and Cultural Context of FGM § Health risks and complications associated with FGM § Practice implications for perinatal care providers

Sufia § 23 years old § Immigrated from Somalia as a teen § Underwent infibulation, WHO Type III FGM § G 3 P 3 § 1 st birth was cesarean due to fetal distress § 2 nd birth was vaginal, with vacuum extraction and episiotomy § Two very young children at home § Husband only support person present, other support unclear

Sufia’s Delivery § 1257: Arrival in triage. 6 cm/75%/-1. Bulging bag. Desires unmedicated vaginal birth. § 1457: SROM. § 1501: Pushing effectively, presenting part visible. § 1502: FHT: 80 s. § 1504: FHT: 70 s. Medial perineal episiotomy started. § 1505: FHT: 60 s. More medial perineal episiotomy. § 1506: OB paged. Anterior episiotomy performed. Crowning. § 1510: Newborn extracted by KIWI vacuum, 1 pull by midwife.

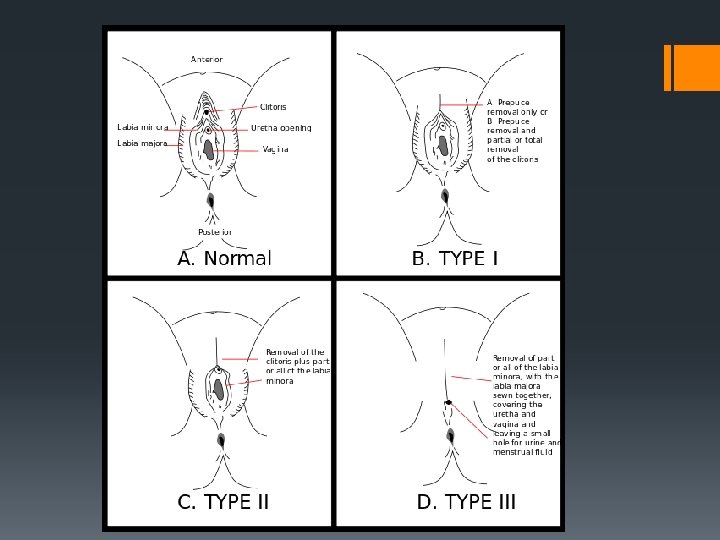
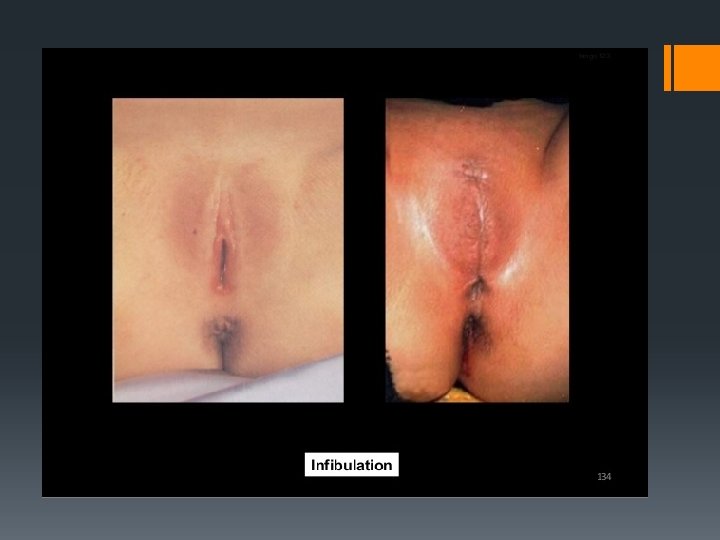
Anatomy of Female Genital Mutilation § WHO definition: “…partial or total removal of the external female genitalia or other injury to the female genital organs for non-medical reasons. ” § Clitordectomy (Type I): removal of prepuce and clitorus (rarely just prepuce). § Excision (Type II): removal of clitorus, prepuce, and inner labia, sometimes also outer labia. § Infibulation (Type III): removal of all, combined with the sewing together of the tissue to leave one small opening for both urination and vaginal function. § Opening is enlarged and sometimes reclosed during the course of the woman’s life to allow for or prevent intercourse, and to allow for childbirth. § Use of hygienic practice and anesthetic varies widely. § Age at time of procedure varies from newborn to adolescent.

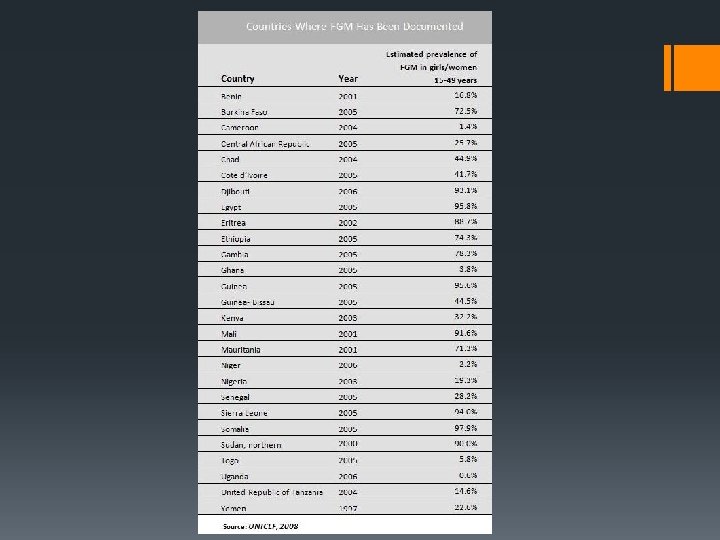
Prevalence of FGM § FGM is most common in the western, eastern, and northeastern regions of Africa, in some countries in Asia and the Middle East, and among migrants from these areas. § Procedures are mostly carried out on young girls sometime between infancy and age 15, and occasionally on adult women. In Africa, more than three million girls have been estimated to be at risk for FGM annually. § More than 125 million girls and women alive today have been cut in the 29 countries in Africa and Middle East where FGM is concentrated.

FGM in the US § In 2000, the African Women’s Health Center at Brigham and Women’s Hospital estimated that 227, 887 women and girls had been at risk of being subjected to FGM in the U. S. that year § Although there are significant communities of people who practice FGM in the US, there are only 2 clinics in the country that specialize in helping these women (in the UK, there are 15) § Seattle has over 25, 000 immigrants from the East African region where FGM is commonly practiced § US federal law prohibits FGM, but only some states have enacted laws—Washington has not § Three states have enacted laws prohibiting “vacation cutting” § There is a lack of information and training in schools and healthcare about how to address FGM or treat victims adequately, and a general silence about the topic

Social and Cultural Context § Religious § Psychosexual Beliefs § Social Convention/Tradition

Social and Cultural Context § Where FGM is a social convention or cultural tradition, the social pressure to conform to what others do and have been doing is a strong motivation to perpetuate the practice. § FGM is often considered a necessary part of raising a girl properly, and a way to prepare her for adulthood and marriage. § FGM is often motivated by beliefs about what is considered proper sexual behavior, linking procedures to premarital virginity and marital fidelity. FGM is in many communities believed to reduce a woman's libido and therefore believed to help her resist "illicit" sexual acts. § FGM is associated with cultural ideals of femininity and modesty, which include the notion that girls are “clean” and "beautiful" after removal of body parts that are considered "male" or "unclean". § Though no religious scripture prescribe the practice, practitioners often believe the practice has religious support. § Religious leaders take varying positions with regard to FGM: some promote it, some consider it irrelevant to religion, and others contribute to its elimination. § Local structures of power and authority, such as community leaders, religious leaders, circumcisers, and even some medical personnel contribute to upholding the practice, which in all cases is rooted in the control of women’s sexual behavior, never for any medical benefit

Common Beliefs in Communities that Practice FGM § It will “cleanse” girls of improper or sexual thoughts or actions. § Women who are circumcised are more faithful. § Circumcision prevents anxiety, neurosis, masturbation, and homosexuality. § Uncircumcised females have such a strong libido, men will have to resort to drugs to match them. § A girl who is not circumcised will have unclean genitals after urination, leading to cervical cancer. § If one prays with unclean genitals, their prayers will not be heard. § The clitoris is poisonous, and if the penis comes in contact with it, the man will become impotent or ill. § The baby will be damaged by contact during birth, and the mother’s milk will become poisonous if the baby contacts it.

Immediate Health Risks § severe pain § shock § hemorrhage § tetanus or sepsis (bacterial infection) § urine retention § open sores in the genital region § injury to nearby genital tissue § fractures/dislocations § failure to heal § death

Long Term Health Consequences § § § § § chronic bladder and urinary tract infections pain cysts, fistulas, abscesses infertility reduction or total loss of sexual sensation/pleasure painful intercourse difficult and painful childbirth--complications higher infant mortality the need for later surgeries. For example, the FGM procedure that seals or narrows a vaginal opening (type 3 above) needs to be cut open later to allow for sexual intercourse and childbirth. Sometimes it is stitched again several times, including after childbirth, hence the woman goes through repeated opening and closing procedures, further increasing and repeated both immediate and long-term risks § Psychsocial complications—not much data, complicated by balance of negative impacts with positive social impacts § There are no medical or health benefits to FGM. The international community regards this practice as a human rights violation rooted in deep seated gender inequality.

Practice Implications § TRAINING! § Planning and education with women of childbearing age to begin discussion of possible complications and management § Careful documentation of perinatal complications believed to be due to circumcision to ensure informed treatment during future pregnancies § Sensitivity to cultural beliefs, while still providing accurate education § Outreach, community education, political action

Questions?
- Slides: 19