Female Genital Cutting in Children Medical Ethical and



























 • 13131 Defibulation (general procedure code) •")






















")








- Slides: 72
Female Genital Cutting in Children Medical, Ethical, and Legal Considerations Janine Young, MD, FAAP November 14, 2019
Financial Disclosures • CDC grant sub-recipient, MN Dept of Public Health, Refugee Centers of Excellence
What is FGM/C? • Medically unnecessary cutting of parts or all of the external female genitalia, including clitoris, prepuce, labia minora and majora • Associated with significant morbidity and mortality • Predates Judaism, Christianity and Islam • Not tied to any specific religion, ethnicity or race • Reasons for FGM/C vary by region and culture – Increases marriageability, preserves virginity, improves hygiene, rite of passage
Photo credit: USAID
FGM/C is a Pediatric Practice • However… • No national/international clinical practice guidelines for medical providers who care for children (UK for abuse) • No training slides • No standard training requirements for Peds, FPs, Child Abuse specialists, Peds Urogyn, Peds surgeons, Adolescent Med docs, Mental health providers • No standard training of Child Protective Services workers, school nurses, teachers
WHY?
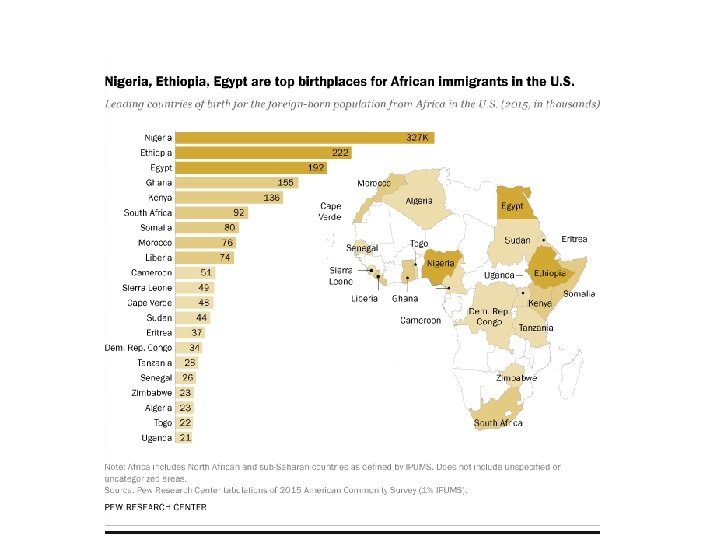
Photo credit USAID PRC, Accessed 9/16/19
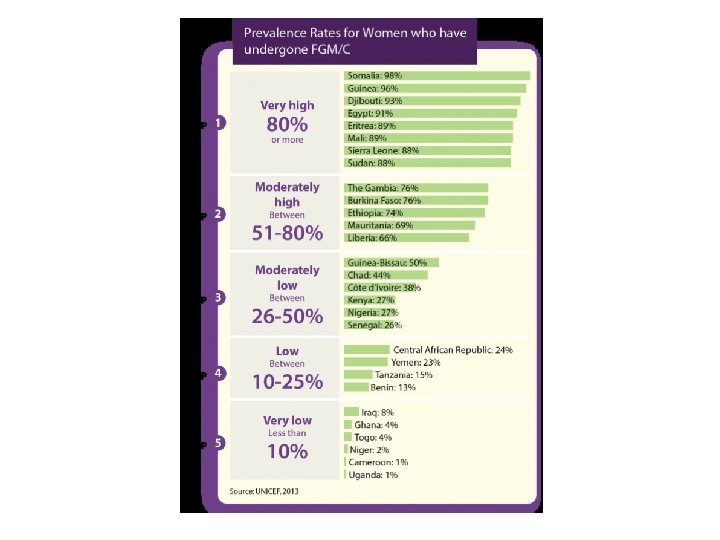
Percentage of girls and women 15 -49 years who have had FGM/C, by country WHO, FGM, https: //www. who. int/reproductivehealth/topics/fgm/prevalence/en/, Accessed 9/16/19
Available at: http: //www. strategiesconcertees -mgf. be/wpcontent/uploads/Captured’écran-2013 -07 -09 -à 23. 22. 37. png
Maternal report of age girls have undergone FGM/C WHO, Human Reproduction Program http: //www. who. int/repro ductivehealth/topics/fgm/ prevalence/en
Girls at risk? How do we know? Population Reference Bureau, https: //www. prb. org/us-fgmc/, Accessed 9/16/19
FY 2017: Illinois resettled 3, 002 refugees Illinois Early Childhood Asset Map, https: //iecam. i llinois. edu/visu al/15932/, Accessed 9/16/19
https: //www. chicago. gov/content/dam/city/depts/mayor/Office%20 of%20 New%20 Americans/PDFs/IL_Refugee_Resettlement_Program_FY 18. pd
Country of origin of at-risk refugee arrivals to ILL, FY 2010 -2015 Benin 1 Cameroon: 1 Central African Republic: 29 Egypt: 9 Eritrea: 157 Ethiopia: 117 Gabon: 1 Indonesia: 3 Ivory Coast: 27 Liberia: 42 Mali: 3 Senegal: 2 Sierra Leone: 3 Somalia: 377 Sudan: 205 South Sudan 1 Togo: 4 Uganda: 11 TOTAL: 993 (45% female) Women and Girls: approx. 447 MN: (1979 -2016): 36, 190 Somalia: 23469 Secondary arrivals to MN 2016: Somalia: 889 CO: (1980 -2017): 10, 805 Somalia: 4646 https: //iecam. illinois. edu/characteristi cs/other-factors/refugees/, Accessed 9/16/19
AAP Clinical Report, Young J, Narang S, et al, pending release
Photo credit: USAID
Standard of care practice? • “At each and every well-child check I examine private parts of all boys and girls to makes sure that everything is normal. I need your parent’s permission and your permission to do so. It takes about 5 seconds and I only check the outside, not the inside. You know that no one should examine your private parts except if a doctor gets permission, right? Do you know that you need to tell a trusted adult if someone is touching your private parts, correct? ”
• • Physical Examination Draped, frog-leg, parent at side for infants, young and mid-aged children Teen with chaperone Document permission and chaperone, as needed Document physical findings • AAP: “A chaperone is recommended during…genital exams and should preferably be a nurse or medical assistant, not a friend or family member. However, offices are not required to have a chaperone. In certain situations, a chaperone may not be present because of patient choice or a chaperone from the office is not available. Pediatricians should develop their own office policy…. . document in the patient’s medical record if and why they are unable to follow it. ” Pediatric Patients and Chaperones in the Exam Room, AAP. Available at: https: //www. aap. org/en-us/about-the-aap/aap-press-room/pages/Pediatric. Patients-and-Chaperones-in-the-Exam-Room. aspx
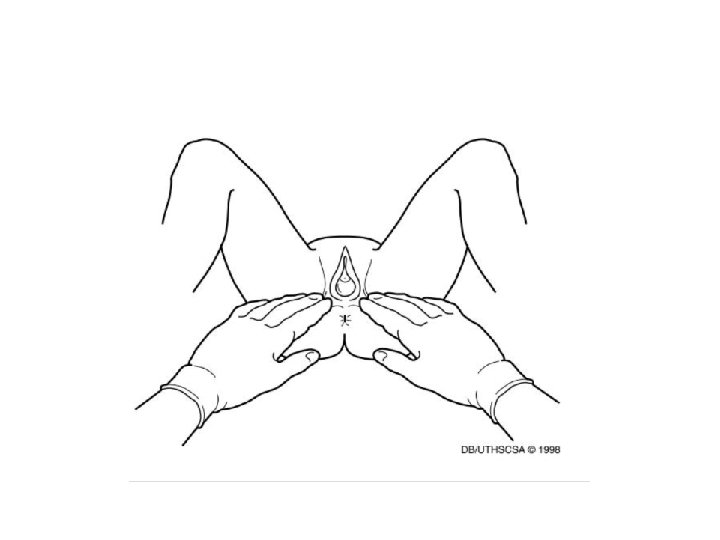
Visual diagnosis of child abuse, CDROM, 3 rd Edition, AAP 2008
Visual diagnosis of child abuse, CD-ROM, 3 rd Edition, AAP 2008
AAP, Visual diagnosis of child abuse, CD-Rom 3 rd
Abdulcadir J, et al. J Sex Med 2016
Abdulcadir J et al. Obstet Gynecol 2016.
Photo credit: USAID
Bright Futures, AAP, Physical Exam Recommendations • Newborn-5 days: “Genitals: Determine whether testes are fully descended. Determine whether labia are open. ” • Infancy: “Genitalia/rectum: Determine that testes are descended; observe for penile anomalies or labial or vaginal anomalies. ” • 6 days-6 years: No genital exam advised, besides asking for concerns in ROS. • 7 -10 years: “Breast and genitalia: Assess for sexual maturity rating. ” • 11 -17 years: “Genitalia: Perform visual inspection for sexual maturity rating. A pelvic examination may be clinically warranted, based on specific problems. ” • 18 -21 years: “Genitalia: Female: Perform examination as indicated by patient or practitioner concerns. Male: Perform visual inspection and examine testicles for sexual maturity rates. Examine testicles for hydrocele, hernias, varicocele, or masses. ” Bright Futures, Guidelines for Health Supervision of Infants, Children
Young J et al, pending publication, J Imm Refugee Health
FGM/C Education, Knowledge, and Comfort in diagnosis among general peds and child abuse peds, n=132
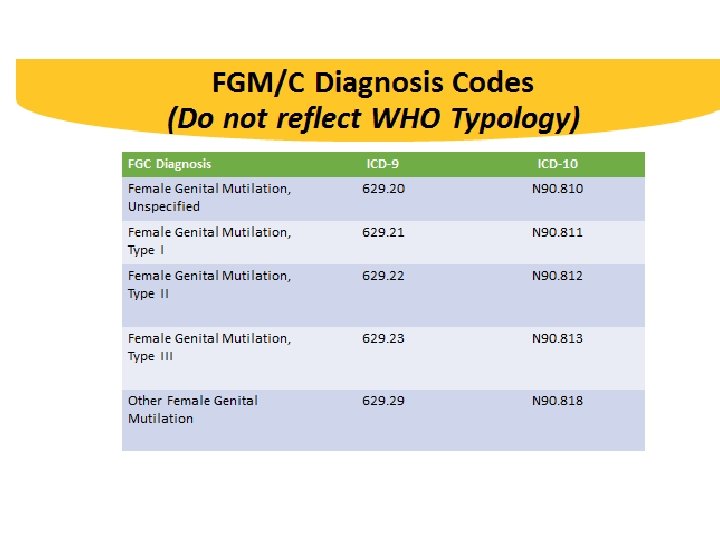
CPT Code Defibulation (Not Specific to FGM/C) • 13131 Defibulation (general procedure code) • 56441 Lysis of labial adhesions • 56800 Plastic repair of introitus Repair, complex procedures on the Integumentary System (forehead, cheeks, chin, mouth, neck, axillae, genitalia, hands and/or feet) For complicated procedures, add the -22 modifier and document any additional physician work
Unpublished data, courtesy of Crista Johnson-Agbakwu, MD, MSc, FACOG
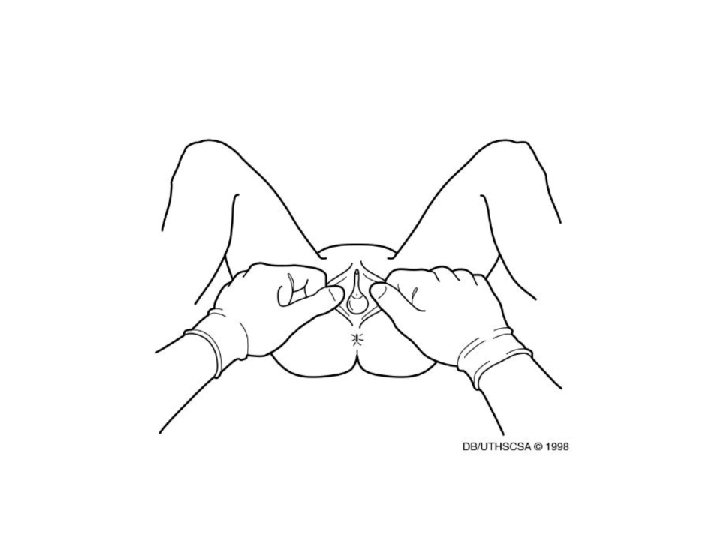
Visual diagnosis of child abuse, CD-ROM, 3 rd Edition, AAP 2008
Visual diagnosis of child abuse, CD-ROM, 3 rd Edition, AAP 2008
Graham, E https: //ethnomed. org/clinical/womenshealth/RFGCGrahamslides. pdf
Young J. et al. AAP FGM/C Clinical Report, pending release
Ethiopian 2 year old, new to US Photo credit: Young, J
Photo credit: Young, J
Graham, E. Reproduced with permission from UW Medicine/Harborview Medical Center for Sexual Assault and Traumatic Stress
Photo credit: M Toure, Bamako, Mali
Photo credit: Sy, Ob. Gyn, Bamako, Mali
BMJ Open, Creighton S et al 2016
Photo courtesy of J. Abdulcadir
Photo credit: USAID
Timeline of International Legislation Against FGM/C Cameroon, The Gambia, Liberia, Sierra Leone and Indonesia do not have any laws or decrees that criminalize FGM/C https: //www. unicef. org/media/files/UNICEF_FGM_report_July_2013_Hi_res. pdf. Accessed May 25, 2018
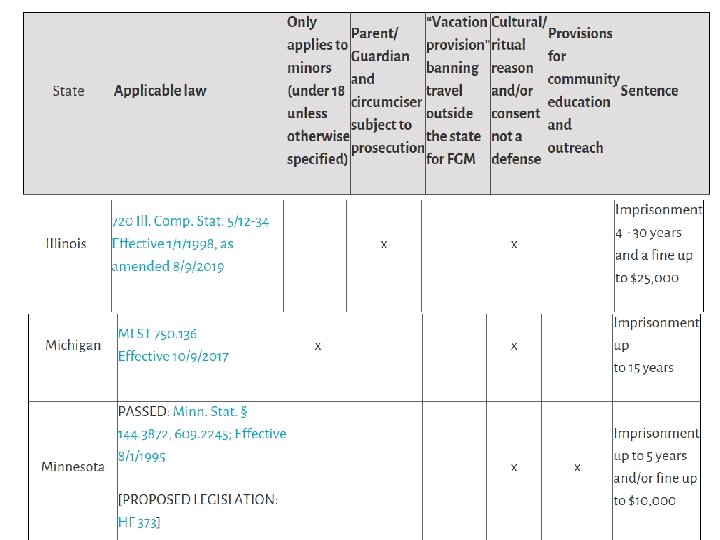
US Laws on FGM/C Equality Now, Available at: https: //www. equalitynow. org/map_fgm_in_the_united_states_ar hived? locale=en, Accessed 9/16/19
• Proposed legislation: – HI – MA – VT – WA – DC Equality Now, https: //www. equalitynow. org/us_laws_against_fgm_state_by_state,
9/13/19, 6 th Circuit Court of Appeals grants the Federal government’s request to dismiss the case against MI medical providers and makes the 1996 Federal law unconstitutional Slide courtesy of Karen Musalo, JD, UC Hastings Law School, updated by J Young 9/16/19
Slide courtesy of Karen Musalo, JD
https: //www. ice. gov/news/releases/ice-homeland-security-investigations-brings-fight-againstfemale-genital-mutilation, Accessed 9/16/19
Slide courtesy of Karen Musalo, JD Decision in Matter of Kasinga broke new ground because it found that 1) FGM/C is persecution – whether or not it is cultural practice, and 2) the ground “particular social group” can include groups defined by reference to gender
Slide courtesy of Karen Musalo, JD
UK Legal Approach • FGM is child abuse and illegal • Health, social care professionals, and teachers are mandatory reporters to the police of FGM/C in girls under 18 years • If a woman 18 and over discloses FGM/C or is diagnosed, no police report, but other local UK safeguarding processes should be followed (i. e. , refer to service offering support, advice and to carry out a risk assessment if she has children at risk).
Call police Available at: https: //www. nhs. uk/conditio /female-genital-mutilationfgm/#the-law-and-fgm (Accessed 11/2/17)
Electronic Medical Record Documentation in Child’s Chart
Atlas for Children with FGM/C • Endorsements from: – EURAPAG (European Association of Pediatric and Adolescent Gynecology – SIGIA (Italian Society of Adolescent and Child Gynecology) • Collaborators: Denver, Phoenix, Brussels, Montreal, Sweden, Paris, Munich, Italy, London
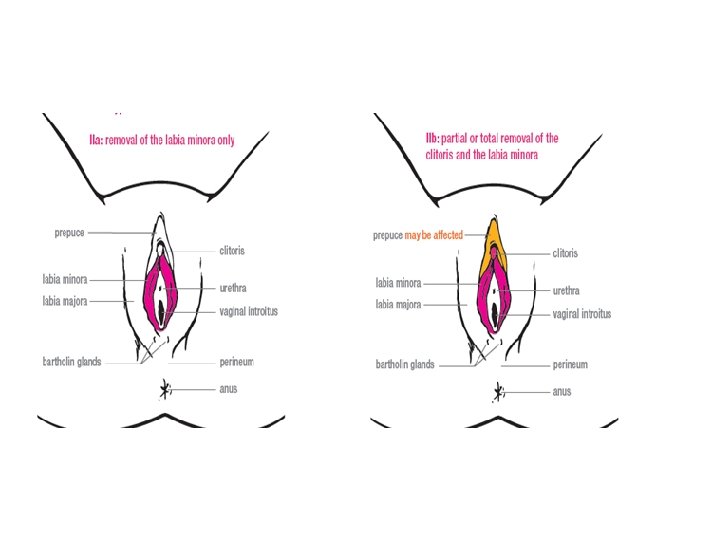
Case 1 • 16 -year-old teen refugee born in Mali and living in Mauritania prior to US arrival. She has established care with her primary care pediatrician who explains that she needs to perform a full physical exam, including examination of her external genitalia. The teen assents to the examination and is found to have Type IIb FGM/C. The girl does not know that she has been cut and has no recollection of the procedure having occurred. She is confused and does not understand what her FGM/C means for her and how she will discuss this with her parents and boyfriend. Young J, Narang S, et al. AAP FGM/C Clinical Report, pending release
Case 2 • 17 -year-old Sudanese girl with Type III FGM/C performed prior to US immigration who has severe dysmenorrhea from partial obstruction of menstrual flow. She wants to undergo defibulation. The teen gives permission for the pediatrician to discuss the issue with her parents and the medical recommendation to undergo defibulation due to medical complications. The parents are very concerned about defibulation and reluctant to give consent. Young J, Narang S, et al. AAP FGM/C Clinical Report, pending
Case 3 • 10 -year-old female born in the U. S. in 2008 to Ethiopian refugee parents presents for well-child care. She had a documented normal physical exam with normal female genitalia at her newborn visit. Well-child care examinations at 4, 6 and 8 years old occurred with the genital exam marked as “deferred” at each visit. Of note, the girl travelled to Ethiopia in 2012 to visit relatives with her mom. A full physical exam, including external genitalia, reveals Type Ib FGM/C. Once the child is dressed, the mother is separately asked if her child had FGM/C performed. She denies any knowledge of her child being cut abroad. Young J, Narang S, et al. AAP FGM/C Clinical Report, pending release
Case 4 • 5 -year-old female refugee from Somalia via a Kenyan refugee camp who had type IIIb FGM/C performed 6 months prior to U. S. immigration. The child has her urethral opening covered by labia minora and urinary stream occurs through a 2 x 2 mm opening in the otherwise sealed labia minora. The patient has reported delay in bladder emptying and pain, per maternal report. She has no report of past urinary tract infections, prolonged fever or vomiting. Young J, Narang S, et al. AAP FGM/C Clinical Report, pending release
Resources • List of US-based Clinical experts in Ob/gyn, Peds, Family Med. —FGM/C Listserv: https: //groups. google. com/forum/#!forum/us-clinician-networkon-fgmc • USG Resources on FGM/C: https: //www. uscis. gov/humanitarian/femalegenital-mutilation-or-cutting-fgmc; brochures in English, French, Arabic, Amharic, Somali, Swahili, and Tigrinya and other information • Caring for Kids New To Canada. http: //www. kidsnewtocanada. ca • CDC Domestic Refugee Screening Guidelines. http: //www. cdc. gov/immigrantrefugeehealth/guidelines/domestic/domes tic-guidelines. html • Care. Ref: https: //carref. web. health. state. mn. us • AAP Immigrant Toolkit. https: //www. aap. org/en-us/about-theaap/Committees-Councils-Sections/Council-on-Community. Pediatrics/Pages/Section-1 -Clinical-Care. aspx
Resources • Hearst A, et al. Female genital cutting—An evidenced-based approach to clinical management for the primary care physician. Mayo Clin Proc. June 2013; 88(6): 618 -629 n http: //dx. doi. org/10. 1016/j. mayocp. 2013. 04. 004 www. mayoclinicproceedings. org • Graham E, Sugar N. Common gynecological problems in pre-pubertal girls. Pediatrics in Review 2006 http: //depts. washington. edu/hcsats/cd/march 2008/Articles/Sugar%20 Gra ham%20 Common%20 Problems%20 in%20 Prepubertal%20 Gyn. pdf • Amanda M. Jacobs, Elizabeth M. Alderman. Gynecologic Examination of the Pre-pubertal Girl. Pediatrics in Review. Mar 2014, 35 (3) 97 -105; DOI: 10. 1542/pir. 35 -3 -97 http: //pedsinreview. aappublications. org/content/35/3/97