FDG PETCT in Staging and Response Assessment in







 Status Limited I One node or a")
")

 image in a patient of diffuse large B-cell lymphoma (DLBCL)")

")
; Bone marrow involvement Transaxial CT image at the level of upper thigh in")

: • There is a high level of concordance between the sites of focal")






 Score Description 1 1 no uptake 2")





: § §")

- Slides: 33
FDG PET/CT in Staging and Response Assessment in Non. Hodgkin Lymphoma Zohreh Adinehpour MD Nuclear Medicine and PET/CT specialist Khatamolanbia PET/CT center
Initial Staging q. Staging of lymphomas is a vital pre-requisite to their appropriate therapeutic management and prognostication. q. Imaging modalities have a fundamental role in the staging of lymphomas. CT is the most commonly used imaging modality for staging malignant lymphoma because of its widespread availability and relatively low cost.
CT lacks functional information • Impedes identification of disease in normal-sized organs and detection of lesions that have poor contrast with the surrounding tissue. • Not reliable in the detection of bone marrow disease, which, if present, by definition indicates stage IV disease. • Ionizing radiation, which may induce second cancers.
Rational behind the use of FDG PET/CT in NHL • Higher overall accuracy • Detects more lesions (intra-nodal and extranodal) • Determine if radiotherapy is appropriate and plan fields • Modifies prognosis
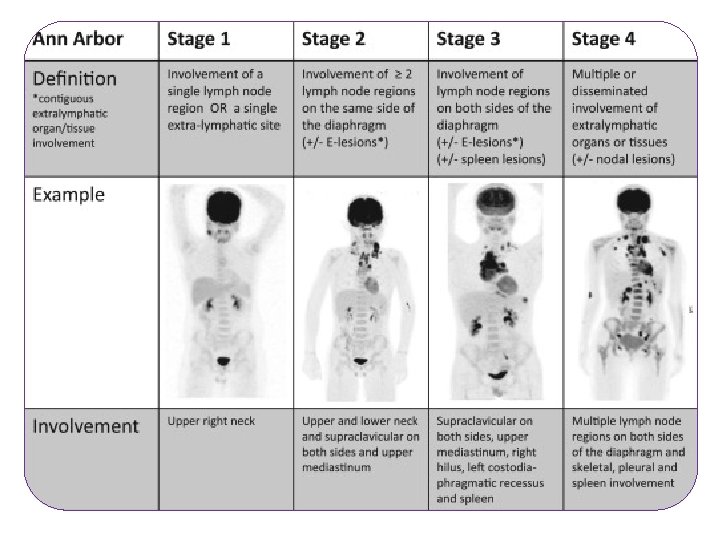
Ann Arbor Staging
Evolution of Lymphoma Staging • 1989 -Costwold modification of Ann Arbor staging system • 1998 - First clinical PET/CT was installed • 1999 - First NHL IWG response recommendations • 2001 - WHO classification, first world-wide consensus • 2007 - IHP redefined the IWG response criteria • 2008 - New WHO classification • 2014 - The Lugano classification
The LUGANO Classification
The LUGANO Classification Stage Involvement Extranodal (E) Status Limited I One node or a group Single extranodal lesions of adjacent nodes without nodal involvemen II Two or more nodal groups Stage I or II by nodal extent with on the same side of the limited contiguous extranodal diaphragm involvement II bulky II as above with bulky disease Not applicable Advanced III Nodes on both sides of the Not applicable diaphragm; nodes above the diaphragm with spleen involvement IV Additional noncontiguous Not applicable extralymphatic involvement
The LUGANO Classification Use of PET/CT • Modality of choice for staging (Gold standard) o More accurate o More sensitive o Improves management • For all FDG avid lymphomas • To identify optimal site for biopsy
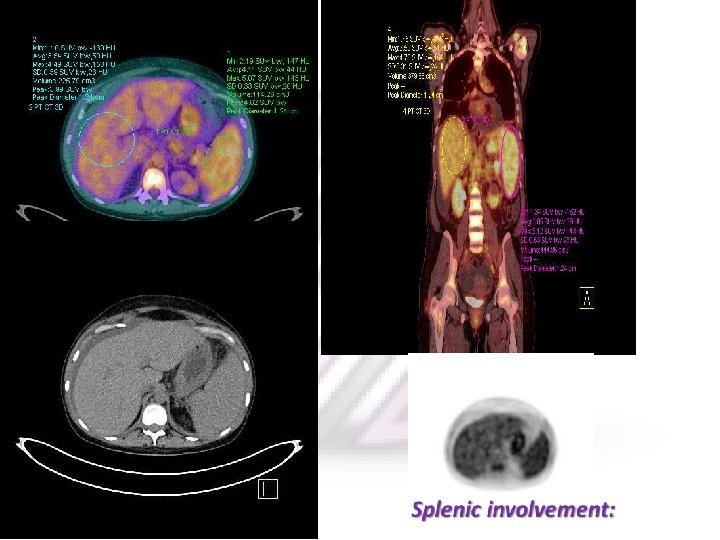
The LUGANO Classification PET may upstage or pick up occult lesions such as splenic, bone marrow , osseous, and gastrointestinal involvement which may otherwise be missed on conventional CT.
Maximal intensity projection (MIP) image in a patient of diffuse large B-cell lymphoma (DLBCL) shows extensive sites of involvement visualized as areas of increased FDG uptake. Transaxial CT images Show axillary and abdominal LAP and a large subcutaneous nodule. Fused PET/CT images show sites of Main advantage over anatomical imaging techniques, such as CT, is its ability to bone marrow involvement in the sternum, spine, and iliac crest, detect metabolic changes in the areas involved with malignant lymphoma before the structural changes become visible. over and above the lesions picked up on CT Usefulness of 18 F-FDG PET in the Initial Staging of Lymphoma
A 19 Y/O gentleman presented for early staging of lymphoma
Staging(cont)
Staging(cont); Bone marrow involvement Transaxial CT image at the level of upper thigh in a case of NHL (DLBCL) appears unremarkable. PET/CT fusion image at the corresponding site shows intense FDG uptake in the bone marrow of proximal right femoral shaft suggestive of marrow involvement
Bony lesions
Staging(cont): • There is a high level of concordance between the sites of focal FDG uptake in the bone marrow and bone marrow biopsy. PET scans have high negative predictive value to exclude bone marrow involvement. • This holds particularly true for HL, and obviates the need for bone marrow biopsy.
The LUGANO Classification • BM involvement; Is routine biopsy needed? BM FDG avid lesion No BM FDG avid or diffuse uptake Hodgkin’s lymphoma X X DLBL X YES
Other Advantage of FDG PET/CT: As it is a whole-body imaging method, it can guide the biopsy from a metabolically active and easily accessible site.
A 59 Y/O male referred for further evaluation of extensive retroperitoneal lymphadenopathy detected in MRI.
Other Advantages of FDG PET/CT: v. Differentiation of indolent from aggressive lymphoma v. Potential to detect transformation of a lowgrade lymphoma to a more aggressive subtype (Richter trnsformation)
PET/CT in Evaluation of Treatment Response: • Evaluating therapeutic response is vital to the management of lymphoma patients. With a larger and more effective therapeutic regimens currently available, it is important to optimize treatment strategies to achieve maximal disease control with minimal toxicity to the patient. • CT has been hitherto the most commonly used imaging modality. A decrease in size of the tumor mass has been the cornerstone in establishing a good therapeutic response. • However, a residual mass picked up on CT may not necessarily be metabolically active.
Deauville Score
Modifed Lugano 5 -point scale (5 PS) Score Description 1 1 no uptake 2 2 Uptake # mediastinum 3 3 Uptake. mediastinum but # liver 4 4 Uptake moderately increased above liver at any site 5 5 Markedly increased uptake above liver at any site ne ne not evaluable X X any areas of uptake not likely to be related to lymphoma Note: Data from cheson et al. 10
Progressive Disease A 29 Y/O lady with Hodgkin’s lymphoma; status post CTX, completed 2 weeks before PET. She is referred for restaging after therapy. 5 months later
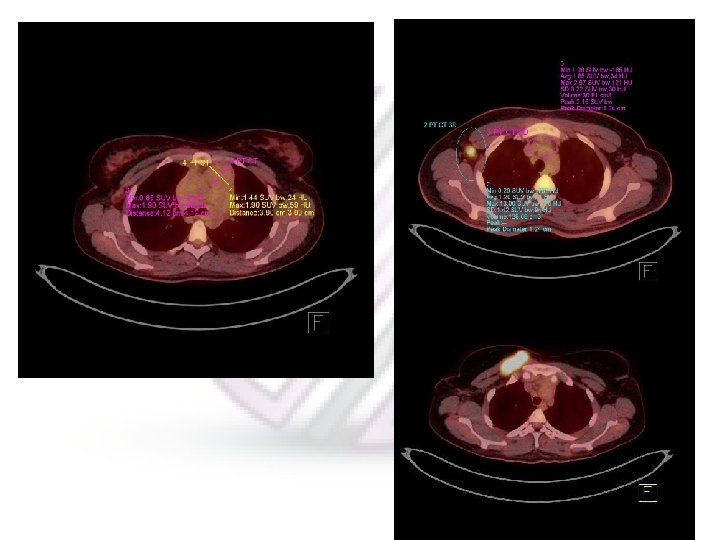
Partial Metabolic Response Left: The patient is a case of biopsy proven diffuse large B cell lymphoma and referred for staging. Right: Monitoring response 17 days after completion chemotherapy
The previously seen, intensely FDG avid, huge retroperitoneal, conglomerate lymphadenopathy is significantly reduced in size (with a small residual remnant) and FDG uptake (SUVmax = 3. 2; prior = 27. 0). However, the uptake in residual mass is mildly greater than the liver (SUVmax = 2. 9) on the current study.
Deauville Score = 5 A 20 Y/O male with NHL status post cx
Major Features of Lugano Classification
PET/CT is recommended for the following childhood malignancies (other than hematological malignancies): § § § To identify site of unknown primary malignancy Staging of sarcoma Germ cell tumors (especially when tumor marker is negative, and there is retroperitoneal lymphadenopathy or mediastinal primary) Patients with hepatoblastoma requiring liver transplant Nephron-sparing surgery in children with synchronous Wilms' tumor planned for bilateral renal surgery Stage III neuroblastoma after initial chemotherapy (if further chemotherapy is being considered to further reduce tumor burden) Mutilating surgery in children with sarcoma MIBG negative or residual neuroblastoma Soft-tissue sarcoma In children where accurate biopsy is essential (e. g. heterogeneous tumors where treatment may be determined by highest grade of tumor as in ganglioneuroma vs. ganglioblastoma, necrotic Wilms' tumor) Children scheduled for radiation therapy planning (gross tumor volume calculation) in head and neck including nasopharyngeal carcinomas.
TNX For Your Attention