Family Systems Intervention with Pediatric Patients YOLANDA C









 a n d Four Tenets � Patient (Child) �")






 � A c c e p t")

 � C")


 Universal – about 33")




 � Vocational Rehabilitation �")





- Slides: 33
Family Systems Intervention with Pediatric Patients YOLANDA C. LEON, PSY. D. , ABPDN SOUTHEASTERN INTEGRATED MEDICINE (SIMED) GAINESVILLE, FLORIDA CROWN PLAZA –HOUSTON , TEXAS INTERNATIONAL CONFERENCE ON ADOLESCENT HEALTH AND CHILD PSYCHOLOGY - SEPTEMBER 29 TH, 2015
Clinically Relevant and Evidence Based Research Family Systems in Pediatric Neuropsychology � Family Systems research (and practice) in pediatric neuropsychology is almost non-existent. � The goals of this presentation include the following: a. familiarize clinicians with family systems concepts b. to assist with c a s e conceptualization c. to help guide referral to other appropriate clinicians
What’s been studied: � Holmbeck – Transition toa d o l e s c e n c e in spina bifida � Wood – Gastrointestinal Disorders, asthma, a n d epilepsy � Quittners – cystic fibrosis � Hoekstra Weebers – children with c a n c e r � Kaslow – Cultural c o m p e t e n c e � M u c h of the work d o n e examining family systems in pediatric psychology is disorder/disease specific
The Research � Early research in pediatric psychology was designed to d e t e c t psychology difficulties a n d e v i d e n c e of family dysfunction. � Findings indicate that children with c a n c e r a n d other pediatric health issues are competent a n d a b l e to c o p e a n d adjust well over time despite initial and/or recurrent periods of extreme distress. � The shift from deficit b a s e d to c o m p e t e n c e b a s e d conceptualization calls for a corresponding c h a n g e in intervention paradigms; A model that will foster c o m p e t e n c e in families, while simultaneously identifying families with elevated and/or escalating psychological distress a n d provide tailored services for their adjustment.
Focus a w a y from Deficit-Based conceptualization � In traditional neuropsychology, deficit b a s e d conceptualization (and focus on psychopathology) m a y not effectively address the needs of the child. � We will review two models b a s e d on the work of Anne Kazak, Ph. D. , ABPP and colleagues at Children’s Hospital of Philadelphia. � Pediatric Psychosocial Preventative Health Model a n d � Medical Traumatic Stress Model
Before we review the models…. . � First some terminology � Next, let’s look at Family systems Frameworks
Terminology � Boundary – A c o n c e p t used in structural family therapy to describe emotional barriers that protect a n d e n h a n c e the integrity of individuals, subsystems, a n d families. � Emotional Cut-off – Flight from a n unresolved emotional attachment. � Enmeshment – Loss of autonomy d u e to a blurring of psychological boundaries. � Expressive Role – Serving social and emotional functions; in traditional families the wife’s role. � Family Homeostasis – Tendency of families to resist c h a n g e in order to maintain a steady state � Family Structure – The functional organization of families that determines how family members interact. - � Family Myths – A set of beliefs b a s e d on a distortion of historical reality a n d shared by all family members that help shape the rules governing family functioning. � Family Projection Process - The mechanism by which parental conflicts are projected onto the children or a spouse.
Terminology � Family rules – A descriptive term for redundant behavioral patterns. � Heirarchical structure – Family functioning b a s e d on clear generational boundaries, where the parents maintain control a n d authority. � Identified Patient- The symptom bearer or official patient as identified by the family. � Joining – A c c e p t i n g a n d a c c o m m o d a t i n g to families in order to win their c o n f i d e n c e a n d circumvent resistance. � Multigenerational transmission process – projection of varying degrees of immaturity to different children in the s a m e family; the child most involved in the family emotional process emerges with the lowest level of differentiation. � Process/Content – Distinction b e t w e e n how members of a family or group relate a n d what they talk about. � Resistance – Anything that patients or families d o to oppose or retard the progress of therapy. � Separation/Individuation – Process whereby the infant begins, at about two months, to draw apart from the symbiotic b o n d with mother a n d develop his or her own autonomous functioning. � Triangulation – Detouring conflict b e t w e e n two p e o p l e by involving a third person, stabilizing the relationship b e t w e e n the original pair.
Family Systems Frameworks � Are broad a n d multidisciplinary � Share c o m m o n assertion that human behavior should b e conceptualized at a broader level than the individual � Families are viewed as “interactive systems” with shared histories and a focus on c h a n g e at the level of the family system � Usually involve consideration of more than o n e generation of the family � Often encompass systems outside of the family in implementing c h a n g e
Therapeutic Triad (Kazak, et. al) a n d Four Tenets � Patient (Child) � Family � Health C a r e Team � Join � Focus � Promote C o m p e t e n c e � Collaborate
Steps to effective Consultation � 1. Join – Process of relationship building with members of a family � 2. Focus – Narrow to the issues directly relevant to the referral � 3. Competence – Strength b a s e d conceptualization � 4. Collaborate – Shared responsibility in problem-solving (collaborator vs. isolated service provider) �
Three Tasks Families F a c e Daily � To soothe themselves in order to handle emotional challenges � To develop trusting relationship to ensure effective collaboration over the course of /diagnosis/illness/treatment � To m a n a g e conflict within the family a n d between the family a n d others
Three Tasks Providers F a c e Daily � Regulate emotional reactions � Trust o n e another, patients, a n d families � Navigate conflict a n d help other professionals navigate conflict
What leads to consultation/Referral? � Families Providers � Handle Emotion Regulate Emotion � Develop trust Trust � M a n g e conflict Navigate conflict � From a systems perspective, consultation request implies that at least o n e of these has g o n e awry
Goals of effective consultation: � 1. Help reestablish effective emotional responses � 2. Help Maintain Trust � 3. Help Navigate conflict
Therapeutic Triad
Joining using the ARCH model (Miccuchi, 1998) � A c c e p t a n c e of patients, families, a n d staff as they are. � Respect � Curiosity – ask questions about their reality/perceptions; how they handle � Honesty in all interpersonal interactions with a n d about the family
Consultation Focus � Although intervention will result in c h a n g e at the systems level, the consultation focus must b e narrowed to the issues directly relevant to the referral. � Keep in mind that a tighter focus c a n b e challenging for a systems oriented consultant trained to conceptualize broadly. (Think of ASD a n d ADHD type referral where referral source (school/physician) wants to address a specific problem or behavior ).
C o m p e t e n c e (strength based) � C o m p e t e n c e b a s e d family systems conceptualization views symptoms as well intentioned attempts at adaptive functioning that have been thwarted a n d seeks to enhance functioning by identifying and refining the competence underlying the symptoms (Waters & Lawrence, 1992) � C o m p e t e n c e b a s e d family systems conceptualizes the presenting concern in terms of competencies, not psychopathology or deviant behavior. � C o m p e t e n c e b a s e d family systems necessitates uses a different l a n g u a g e than that of a psychopathology or diagnosis oriented approach a n d aims to probe for alternative understandings of the behavior rather than “controlling” the behavior. � * b y understanding symptoms as responses to adversity, the situation c a n b e NORMALIZED a n d a collaborative intervention c a n b e d e v e l o p e d.
Collaborate – vs. isolated service provider � Partner with the family/patient a n d treatment t e a m. Shared responsibility for problem-solving, thereby encouraging the c o m p e t e n c e of all parties is encouraged
Pediatric Psychosocial Preventative Health Model � Builds on the assumption that most families of children with illness/disorders are competent a n d adaptively organized families without elevations in their risk for psychopathology. � All Families have understandable distress associated with child’s diagnosis (or in the c a s e of initial referral for differential diagnosis, the POTENTIAL dx) � Evidence supports the diagnosis of childhood illness (cancer) as a series of post traumatic events that c a n l e a d to trauma symptoms including a v o i d a n c e , numbing, physiological arousal, intrusive memories a n d helplessness.
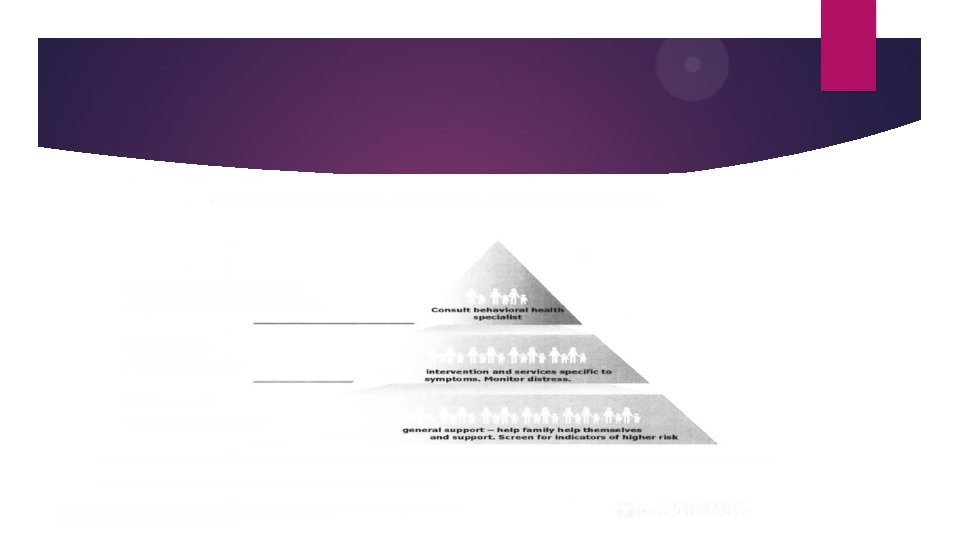
Levels of N e e d or Risk (Kazak, 2006) Universal – about 33 % Targeted 25% � Lowest risk Higher risk Highest risk � M a y or m a y not n e e d services Needs Services Escalating n e e d for services � Psychologically healthy Stressors/adjustment Severe psychopathology � Clinical/Treatment < 10% � These levels are not static - families c a n m o v e from level to level � Movement of the family or the child to a lower level c a n b e a c h i e v e d through � A. Effective Intervention � B. Change in the child’s condition
A c u t e Stress/Post Traumatic Stress in Families of Newly Diagnosed � N = 140 children diagnosed with c a n c e r : � 50 % mothers a n d 40% of fathers met criteria for ASD � 124/125 parents with a child in treatment for c a n c e r reported PTSD symptoms with PTSD Reaction Index Scores in the Moderate Range � 1/3 of the siblings of survivors report Moderate to severe PTSD
Medical Traumatic Stress Model � Empirically derived a p p r o a c h , utilizing a developmental conceptualization of traumatic illness across the trajectory, for understanding the family’s experience throughout child’s diagnosis of cancer. Three stages: � 1. Peri-Trauma – The immediate time period around the traumatic event (eg; diagnosis of ASD, Intellectual Disability, TBI, Seizures) c a n l e a d to trauma symptoms � 2. Treatment – Period of time during treatment (variable in length a n d course) and continues to expose patient and family to ongoing PTE’s. � 3. Long Term - Children who h a v e c o m p l e t e d treatment or died.
Points to k e e p in mind: � Trauma reaction after significant childhood illness/diagnosis is not always pathological or negative a n d c a n b e potentially adaptive. � General trauma informed c a r e is utilized in the model.
Implementing the Model � 1. Assess the family’s level of risk � 2. Reassessment of risk � 3. Collaboration a m o n g clinicians to address needs of the family � 4. Be a facilitator of collaboration across psychosocial providers* � 5. Take on the role of c o a c h or trainer � (provide education, resources, problem-solving that will allow other treatment t e a m members to integrate psychosocial c a r e into daily work) � * The “blindfolded men” story
Potential Resources � School � Daycare � Military (base programs) � Vocational Rehabilitation � SSDI � Early Childhood Programs � Faith Communities (specialized programs) � Community Based Disorder specific Programs (CHAD, ASD, Brain Injury support groups, ADHD groups, Life Center, etc. )
Two Treatment A p p r o a c h Models � 1. Family Systems Oriented Model – Provide structure for the entire family. Although the child m a y b e the target of the intervention, the emphasis is on providing the structure necessary for all participants in the triad to function more competently. � Highly Focused � Sets realistic goals � Assures that service delivery is provided safely a n d a c u t e distress is r e d u c e d without attempting to “cure” more severe and chronic family problems that may be contributing to the Presenting Problem
Two Treatment A p p r o a c h Models � 2. When Difficult Situations Arise (verbal/physical aggression; perceived interference from family members; non-compliance) � Provide consistency � C r e a t e strong t e a m leadership � Have frequent t e a m meetings a n d solid support of staff � Be aware of traumatic stress during the “survivorship” stage � Educate other providers about traumatic stress
E m b e d d e d vs. Consultant role � E m b e d d e d Role – This model provides for more opportunity for the development of services that are integral to patient c a r e a n d facilitates multidisciplinary e x c h a n g e s that foster collaborations on research, practice, a n d teaching. � Consultative Role – A more limited model in which services are typically provided to individual patients and the consultant’s role is defined more narrowly. � Biggest Consideration………. COST
Questions? . . � Questions, Comments, Discussion
Final Thoughts……. . � Thank you for your time, attention, a n d courtesy. � Best Wishes, yours truly Yoli