Family Medicine Gait Analysis Knee Injuries FootAnkle Injuries
































 • Rehab • Surgery if continued")

























































- Slides: 95
Family Medicine: Gait Analysis, Knee Injuries, Foot/Ankle Injuries and Overuse Injuries Selina Silva, MD Associate Professor, Pediatric Orthopaedics Medical Director, UNM Carrie Tingley Hospital
Outline • • Gait Analysis Knee injuries Foot/Ankle injuries Pediatric overuse injuries
Gait Analysis • Can be informal with clinical evaluation of gait during a routine visit • Tip: have child walk in hallway if they are older. Easier to see abnormalities. • Can also get formal gait analysis in a gait laboratory.
Femoral Anteversion
Internal Tibial Torsion
Miserable Malalignment
Miserable Malalignment
Gait lab • Video analysis of children walking to aid in preoperative planning. • Goal would also be for every child with movement disorder (cerebral palsy, muscular dystrophy, etc) have a simple video of them walking stored annually. • Research is another large parts of plans for the gait lab
Gait lab
Gait lab
Gait lab
Gait lab
Gait lab
Knee Injuries • • • Anatomy and Physical Exam ACL MCL Patella Dislocations
Anatomy • • • ACL PCL MCL LCL Meniscus – Medial – Lateral
Knee Anatomy
Physical Exam of the Knee • Inspection • Palpation • Range of Motion • Special tests • Neurovascular assessment
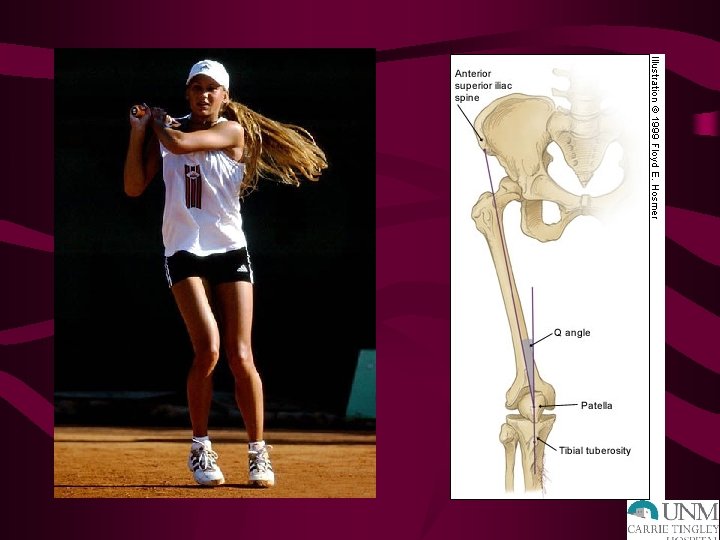
INSPECTION • Effusion • Q angle • Erythema • Angular deformities • Ecchymosis • Edema • Muscular asymmetry
PALPATION ANTERIOR MEDIAL • Tibial tubercle • MCL • Infrapatellar tendon • Meniscus • Quad insertion • Pes anserine insertion • Patellar facets • Tibial plateau • Crepitus ? • Femoral condyle
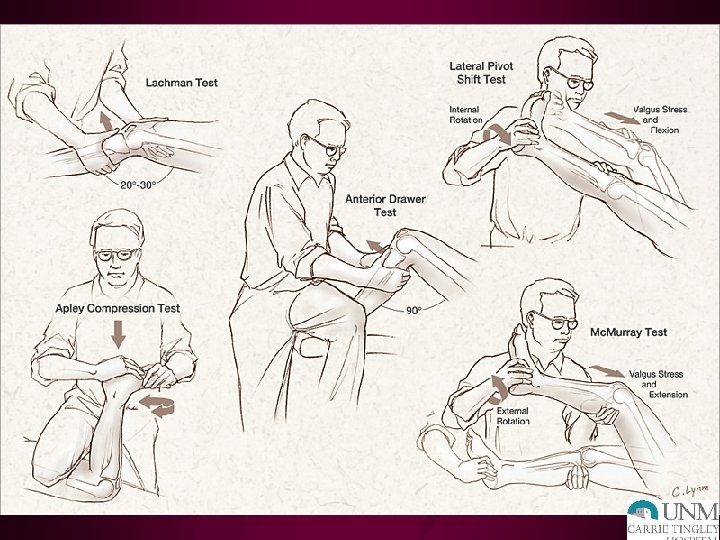
ACL Special Tests • Anterior drawer • Lachman test • Pivot shift test • Valgus stress test at full extension!
Grading Ligament Injuries
ACL: PHYSICAL EXAM • Decreased ROM • Effusion-hemarthrosis, immediate • + Instability tests – Lachman: most accurate – Pivot shift – Anterior drawer • + MCL and meniscus tests
LIGAMENT INJURIES: XRAY • AP – Lateral capsular sign: Segond fx – Tibial spine avulsion fx – Physeal injuries • Lateral – Lateral condyle divot – Obliques ? • Tangential (Merchant)
MRI
ACL TREATMENT • Grade 3 Injuries- Surgery • Indications – Most active people will require surgery to restore adequate function and decrease instability – Recurrent instability – Inability to modify activity – Associated injuries: meniscus – Age? • Wait three weeks due to arthrofibrosis risk • 100% @ 6 -12 months
MCL INJURIES HISTORY • Mechanism = valgus stress • Medial joint line pain • Lack of large effusion • Difficulty weight-bearing
MCL Injuries - Physical Exam • Tender to palpation along MCL • Pain + instability with valgus stress – 30 o flexion = MCL – 90 o flexion = associated ACL • COMPARE SIDES
MCL Injuries – Treatment Grade 1, 2 • Early mobilization • Weight-bearing as tolerated • Hinged knee brace • Recovery 4 -6 weeks
MCL Injuries – Treatment Grade 3 • Isolated = nonsurgical management • Combined = surgery consistent with associated injuries • Natural Hx = lack of long-term degenerative changes seen with ACL, meniscus
PCL INJURIES • Mechanism – Sports = fall on flexed knee with foot plantarflexed, hyperextension, pivot – MVA = dashboard injury • Effusion (less than with ACL) • Shifting/instability (chronic) • Less distinctive
PCL Injuries – Physical Exam • + Effusion • + Posterior drawer test • + Posterior sag sign • False positive Lachman test • Common to have isolated injuries
PCL Injuries - Treatment • Functional bracing (early) • Rehab • Surgery if continued instability, effusions • Note- 2% of NFL preseason exam with incidental isolated PCL tear
PATELLAR INSTABILITY • Acute patellar dislocation • Acute patellar subluxation • Patellar tracking dysfunction
PATELLAR DISLOCATION History • • Mechanism = pivot Immediate effusion May visualize patella dislocated laterally + Instability (chronically) Frequently Patella spontaneously relocates
Patellar Dislocation – Physical Exam • Tender peripatellar structures – Medial retinaculum – Lateral femoral condyle • Effusion • ? Patella dislocated laterally X-rays- osteochondral fracture, effusion
XRAYS
PATELLAR DISLOCATION • • Treatment Knee extension immobilizer in ER Early quad setting exercises Change to Shield’s Brace Return to sport – Full, painless ROM – Normal strength – Adequate aerobic fitness
Fractures and Dislocations about the Knee in Pediatric Patients
Anatomy • Distal femoral physis- large, undulatingirregular • Proximal tibial physis- contiguous with tibial tubercle apophysis • Ligament and muscular attachments may lead to avulsion injuries, fracture angulation
Anatomy- Neurologic and Vascular Structures • Popliteal artery tethered above and below knee • Common peroneal nerve vulnerable at fibular neck/head
Distal Femoral Physeal Fractures • Direct blow mechanism • Salter I or II common • Check neurologic & vascular status
Distal Femoral Physeal Fractures • Closed reduction and pinning for displaced fractures • Long leg cast
Distal Femoral Physeal Fractures • High rate of premature growth arrest – rare < 2 yo – 80% 2 - 11 yo – 50% > 11 yo • Angular deformity • Leg length discrepancy
Patella Fractures in Children • Largest sesamoid bone, gives extensor mechanism improved lever arm • Uncommon fracture in skeletally immature patients • May have bipartite (superolateral) patella- avoid misdiagnosis
Patellar Sleeve Fracture • 8 -12 year old • Inferior pole sleeve of cartilage may displace • May have small ossified portion • <2 mm displaced, intact extensor mechanism- treat non-operatively
Patella Sleeve Fractures • Avulsion mechanism • Management same as adults • Restore articular surface and knee extensor mechanism
Tibial Tubercle Fractures • Primary insertion of patellar tendon into secondary ossification center of proximal tibia • Mechanism- jumping or landing, quadriceps resisted contraction • Common just before completion of growth (around 15 years in males)
Tibial Tubercle Fractures. Treatment • Nondisplaced, intact extensor mechanism- above knee immobilization for 6 weeks in extension • Displaced, loss of extensor mechanism integrityoperative fixation
Tibial Tubercle Fracture • 10 - 14 year old • Often during basketball • Surgery for displaced fractures, inability to extend knee
Proximal Tibial Physeal Fractures • Usually Salter II fractures. • Occasionally Salter I or IV • Posterior displacement of epiphysis or metaphysis can cause vascular compromise
Proximal Tibia Fracture
Proximal Tibia Salter I Fracture
Proximal Tibia Physeal Fractures • Open reduction for irreducible Salter I and II, displaced Salter IV • Observe closely for vascular compromise or compartment syndrome in first 24 hours • Follow for growth disturbance, angular deformity
Complications • • Angular deformity Malunion Physeal bar Leg length discrepancy
Proximal Tibial Metaphyseal Fractures • Younger patients, less than 6 years • Often nondisplaced, nonangulated • Later progressive valgus deformity can result from medial tibial overgrowth (Cozen Phenomenon)
Proximal Tibial Metaphyseal Fractures • Initial treatment- try to mold into varus to close any medial fracture gap • Notify parents initially of possible valgus deformity development • Follow 2 -4 years
Genu Valgum following Proximal Tibia Metaphyseal Fracture
Valgus after Proximal Tibia fx
Proximal Tibia Metaphyseal fx, Displaced- Often Young Child, High Energy 3 yo boy Careful assessment of distal perfusion necessary, monitor for compartment syndrome
Foot and Ankle Injuries
Pediatric Ankle Fractures • 2 nd most common site of physeal fractures in children • Most occur between ages 10 - 15 y. o. • Boys > girls • Direct and indirect mechanisms
Ankle Anatomy • All ligamentous structures attach distal to the physis • Ligaments are stronger than physis • Physeal injury more common
Distal Tibial Physeal Closure
Classification - Ankle Fractures • Anatomic: Salter. Harris • High interobserver correlation • Correlated with outcomes
Accessory Ossification Centers – Smooth Borders
Salter I Distal Fibula – typical “goose egg” swelling over distal fibula with tenderness over distal fibular physis
Salter II Distal Tibia Fracture
Salter III Injury- CRIF
Salter IV Distal Tibia Fracture Fixation avoids physis
Salter-Harris Type V fxs • Crush injury to physis • No associated displacement • Diagnosis made with follow-up xrays revealing premature physeal closure • treatment directed primarily at sequelae of growth arrest
“Transitional” Fractures • Fxs occurring during asymmetric closure of distal tibial physis – Triplane fx • 2, 3 or 4 -part fxs • lateral more common – Juvenile Tillaux fx
“Transitional” Fractures • Triplane fx – tend to be seen in younger pts than pts with Juvenile Tillaux fx – more displacement/swelling more severe – Treatment decisions usually based on articular displacement
Juvenile Tilleaux Fracture-ORIF
Pediatric Ankle Sprains • Should be diagnosis of exclusion • Where is tenderness – over bone/physis or ankle ligaments? • Often represent missed Salter I ankle fractures, non-displaced calcaneal fractures • Follow-up persistent pain
Pediatric Foot Fractures • Often missed diagnosis • Reductions of fractures important – less remodeling potential – reach 50% of mature length of foot bones by 18 mo. (compared to femur/tibia - do not reach until 3 y. o. )
Pediatric Foot Fractures • Types of foot injuries 1 – metatarsal fractures 90% – phalangeal fractures 18% – navicular fractures 5% – talar fractures 3% – calcaneal fractures 3% – cuboid fractures 2% • 1 data from Cleveland Fracture Service, A. Crawford (Skeletal Trauma)
Pediatric Overuse Injuries
“PEDIATRIC SPORTS INJURIES: A COMPARISON OF MALES VERSUS FEMALES” STRACCIOLINI A ET AL, AM J SPORTS MED 2014 Ø Cross sectional study Ø Chart review performed using 5% random sampling (N=2133) of children aged 5 -17 over a 10 year period Ø Females had higher incidence of overuse injuries at 62. 5% Ø Males had more traumatic injuries at 58. 2% Ø Females had more injuries in the lower extremities. Males had more injuries in the upper extremities. Ø ACL tears were equal
“SPORTS-SPECIALIZED INTENSIVE TRAINING AND THE RISK OF INJURY IN YOUNG ATHLETES: A CLINICAL CASECONTROL STUDY” JAYANTHI NA ET AL, AM J SPORTS MED, 2015 Ø Case Control Study to determine if sports specialization, weekly training volumes, or growth rates are associated with increased risk for serious overuse injuries Ø Injured athletes aged 7 -18, years 2010 -2013 Ø 1214 athletes enrolled, 822 were injured and 368 uninjured Ø Injured athletes were older (14. 1 vs 12. 9) and more total active hours (19. 6 vs 17. 6) Ø Sports specialization was an independent risk of serious overuse injury with odds ratio of 1. 27 and 95% CI Ø Also at significant risk are children that spend more hours/wk in sports than their age. This is different from “free play”
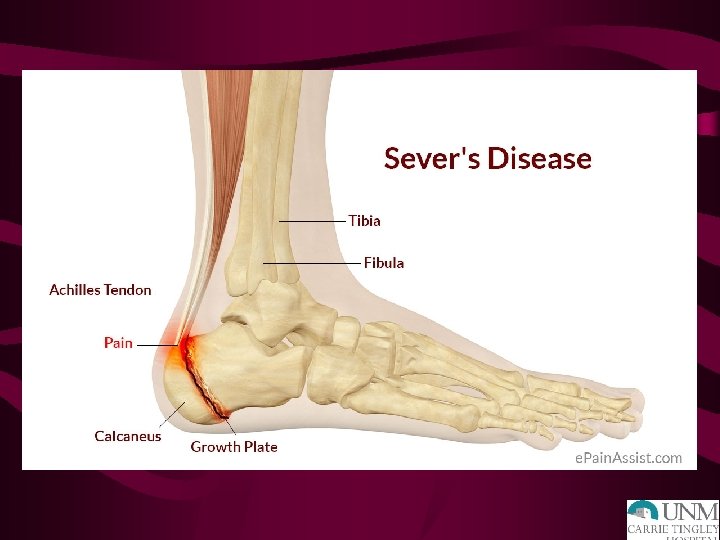
“SPORTS-RELATED OVERUSE INJURIES IN CHILDREN” LAUNAY F, ORTHOP TRAUMATOL SURG RES, 2015 Ø Overuse injuries are better known as “osteochondrosis” Ø This refers to the inflammatory conditions of bone and cartilage Ø Most overuse injuries affect the lower extremities and most common types are Sever’s and Osgood-Schlatter Ø In both of these conditions: the tendon remains relatively short during the pubescent growth spurt which may contribute to their increased incidence Ø Seems to be correlation with not just increased sports activity, but concurrent decreased “free play” or activity out of sports
DIAGNOSIS Ø Primarily history and physical exam Ø Radiographs to rule out other problems, such as stress fractures, osteochondritis dissecans, infection, tumor, etc. Ø Some osteochondrosis can be seen on x-ray, but not common Ø Getting an MRI or CT scan is not necessary to confirm diagnosis
CASE - OD Ø 9 yo male complaining of left heel pain. Started during basketball season. No injury, no fever. Parents concerned about his pain not improving and now starting to have noticeable limp after basketball. Ø Lateral left foot xray is shown:
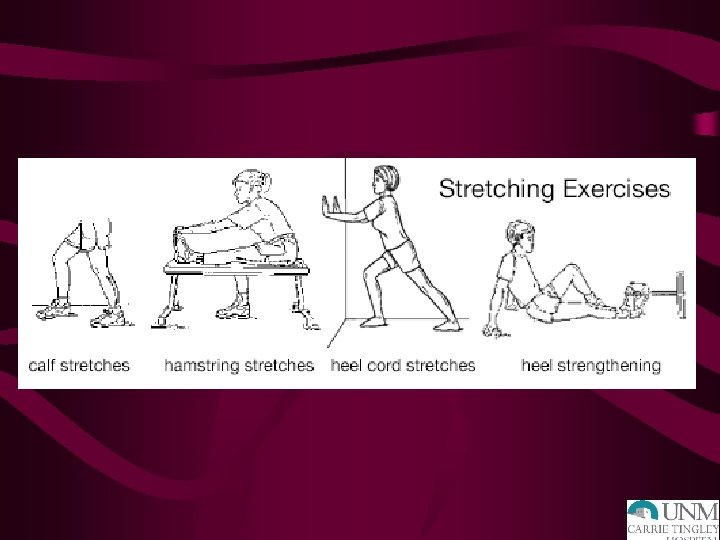
TREATMENT Ø Break from sport Ø Anti-inflammatories Ø Ice/heat compresses Ø Then stretching program and slow return to sport Ø Really need to speak with the family why their child is in pain and get them on board with prevention of this happening again Ø Unfortunately, commonly a rollercoaster until the child is done growing
“A HEEL CUP IMPROVES THE FUNCTION OF THE HEEL PAD IN SEVER’S INJURY: EFFECTS ON HEEL PAD THICKNESS, PEAK PRESSURE AND PAIN” PERHAMRE S ET AL, SCAND J MED SCI SPORTS, 2012 Ø Apophysitis calcanei is a common cause of heel pain in children 815 years old. Ø Purpose was to assess the effect of a heel cup on heel pad thickness and heel peak pressure Ø 50 subjects evaluated Ø The heel pad thickness improved and heel peak pressure was significantly reduced with use of the heel cups Ø This translated to significant reduction in pain when using a heel cup in a sports shoe versus not using one
“THE EFFECTIVENESS OF EXERCISE INTERVENTIONS TO PREVENT SPORTS INJURIES: A SYSTEMATIC REVIEW AND META-ANALYSIS OF RANDOMIZED CONTROLLED TRIALS” LAUERSEN JB ET AL, BR J SPORTS MED, 2014 Ø To determine if physical activity exercises can reduce sports injuries Ø 3462 studies, 25 trials ultimately selected for total of 26, 610 participants with 3, 464 injuries Ø Favorable estimates were obtained for all injury prevention measures except for stretching. Ø Strength training reduced sports injuries to less than 1/3 and overuse injuries can be reduced by almost 50%
SUMMARY Ø There is more awareness of overuse injuries and there is increased risk in females, older children (teenagers), kids that participate in the same sport year-round, and kids that have sports: free play ratio of 2: 1 Ø Treatment is still rest, ice, anti-inflammatories, and strengthening/stretching program Ø Prevention is the key: Ø More cross training Ø Kids being more active in “free play” Ø Not pushing kids into excessive hours of sport training
THANK YOU!