Facility Orientation Building Orientation Building Orientation Front Desk

Facility Orientation

Building Orientation

Building Orientation Front Desk

Building Orientation Operating Rooms

Building Orientation Endoscopy Rooms

Building Orientation Nurses Station

Building Orientation Spill Kit Locations Decontamination Rooms

Building Orientation E m e r g e n c y E x i t s

Building Orientation SDS/ MSDS Sheets

Building Orientation

Building Orientation

Building Orientation

Building Orientation

Building Orientation

Building Orientation

Building Orientation Primary Rally Point Call Room

Building Orientation Unless Disaster is in these areas

Building Orientation Then go to Secondary Rally Point Break Room

Trash. Room Building Orientation Biohazard Freight Elevator Boiler Room Central Processing/ Quad Other Locations You Might Need To Know Materials Management Garage Break Room Conference Room Lobby Elevator Call Room

BLOODBORNE PATHOGENS, OCCUPATIONAL EXPOSURE And Injection Safety
 § Estimates more than 5. 6 million healthcare")
OSHA (Occupational Safety and Health Administration) § Estimates more than 5. 6 million healthcare workers are at risk of occupational exposure to pathogens.

§ 1 out of 5 healthcare workers will get a needlestick injury this year. An average of 1, 000 sharps injuries per day. § 800, 000 needlestick injuries are estimated to occur every year in the United States. More than half are never reported.

§ The best way to prevent exposure is to follow proper procedures, including; § § § Standard Precautions Sharps safety Hand hygiene PPE use Environmental cleaning Correct disinfection and sterilization processes.
. Hepatitis C virus (HCV) Human immunodeficiency")
Bloodborne Pathogens These include hepatitis B virus (HBV). Hepatitis C virus (HCV) Human immunodeficiency virus (HIV).

§ Exposures occur through needle sticks § Cuts from contaminated sharp instruments § Contact of the eye, nose, mouth or unintact skin with a patient’s infected blood or body fluid.

§ 500 million people worldwide are currently infected with hepatitis B or C. § This is over 10 times the number infected with HIV/AIDS.

§ Hepatitis B and C kill 1. 5 million people a year. § 1 in 3 people has been exposed to either or both viruses. § Most of the 500 million infected do not know that they are.

FOLLOWING AN EXPOSURE The risk of infection may vary with factors such as: § The pathogen involved § Type of exposure § Amount of blood involved § Amount of virus in the blood §

RISK OF INFECTION AFTER EXPOSURE § Hepatitis B-HBV-There is a vaccination available. § If vaccinated with acquired immunity there is no risk for infection. § Risk for non-vaccinated, susceptible persons from a single needlestick or cut exposure is 6 -30%.

HBV § 1/3 will show no symptoms. § 1/3 will have flu like symptoms that will go away. § 1/3 will have acute symptoms. § 6 -10% will become chronic carriers, able to transmit disease with no symptoms.

HBV § There is post exposure treatment for nonvaccinated workers or non reactors to the vaccine. § Workers should be tested 1 -3 months after receiving the vaccine series to make sure the vaccine has provided immunity.

HBV § The annual number of occupational infections has decreased 95% since the availability of the hepatitis B vaccine.

HEPATITIS C VIRUS-HCV § The risk for infection after a needlestick or cut exposure is 1. 8%. § There have been reported HCV infections from blood splash to the eye and non intact skin.

HCV § Studies have shown 1% of hospital healthcare personnel have evidence of HCV infection. § There is currently no vaccine or post exposure prophylactic treatment available. § Treatment with pegylated interferon therapy is available for hepatitis C positive patients.

HUMAN IMMUNODEFICIENCY VIRUS-HIV § The risk of infection after needle stick or cut exposure to infected blood is 0. 3% or 1 in 300. (99. 7% do not lead to infection). § The risk of infection after exposure of the eye, nose or mouth is 0. 01%(1 in 1, 000). § Exposure to non intact skin is less than 0. 01%.
")
HIV § There is currently no vaccine against HIV. § Post exposure prophylaxis (PEP) can reduce the chance of transmission.

IF EXPOSURE OCCURS § Immediately wash the area with soap and water. § Do not “milk” the wound. § Flush splashes with copious amounts of water. § Irrigate eyes with clean water, saline or sterile irrigant.

§ Immediately report the exposure to your supervisor. § Know where to find the “Needlestick Packet” and fill out the correct paperwork. (Outside Nurse Managers’ Office) § Go to BMC Occupational Med for treatment and counseling. Call first to let them know you are coming.

UNIVERSAL PRECAUTIONS AND STANDARD PRECAUTIONS. § OSHA developed Universal Precautions: § § All bodily secretions are treated as infectious with the exception of sweat. CDC (Centers for Disease Control) Developed Standard Precautions: § All bodily secretions are treated as potentially infectious except sweat PLUS :

STANDARD AND TRANSMISSION BASED PRECAUTIONS Transmission based precautions which include: 1. Airborne 2. Droplet 3. Contact precautions §

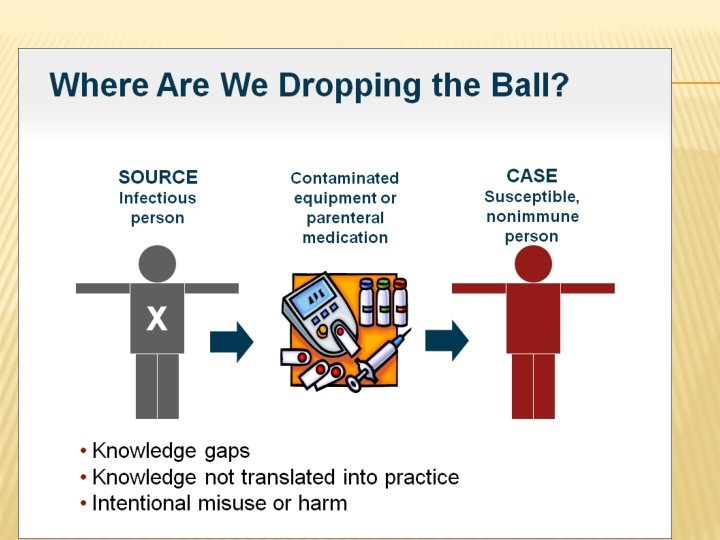
PATTERNS OF TRANSMISSION § § § Direct contact Indirect contact Droplet Airborne Common Vehicle

DIRECT CONTACT: § Source: healthcare workers and patients § Direct physical contact between the source and the patient (person-to-person contact).

INDIRECT CONTACT: § Source: Medical devices, equipment, endoscopes, objects shared with more than one patient. § Transmission of the infectious agent from the source to the patient occurs passively through contact with an intermediate object (usually inanimate); stethoscope, bedside table, BP cuffs, Endoscopes.

DROPLET: § Source: Patients and healthcare workers. § Transmission via large particle droplets (> 5 µm) transferring the germ through the air when the source and patient are within close proximity; e. g. transmission by sneezing, talking, coughing, suctioning.

AIRBORNE: § Source: Patients, health-care workers, hot water, dust. Propagation of germs contained within nuclei (< 5 µm) evaporated from droplets or within dust particles, through air, within the same room or over a long distance; e. g. breathing §

COMMON VEHICLE: § Source: Food, water, medication. § A contaminated inanimate vehicle acts as a vector for transmission of the microbial agent to multiple patients; e. g. drinking contaminated water, unsafe injection.

UNIVERSAL AND STANDARD PRECAUTIONS § Both involve Hand Hygiene as the most important focus to prevent infection. § PPE (personal protective equipment)-the correct use and removal of gloves, gown, mask, eye protection or face shield.

§ Unfortunately the transmission of pathogens from one patient to another via health-care workers’ hands is easy. § By observing the 5 Moments for hand hygiene pathogen transmission can be prevented.

THE “ 5 MOMENTS FOR HAND HYGIENE”

GOAL: TO REDUCE OR ELIMINATE EXPOSURE § § § Engineering Controls; Safety Needles, scalpels, and medical devices. Sharps disposal containers. Work Practice Controls; Reduce exposure by changing the way a task is performed.

§ No recapping Needles! § Use PPE, Hand hygiene. § Reduce the exposure to blood and body fluids. § Minimize splash in procedures (emptying the kickbucket by using the Neptune). § Reduce hand to mouth activities where exposure to blood or body fluids is likely.

TYPES OF PPE § § § Gloves; to protect hands. Gowns; to protect skin and clothing. Masks and respirators; to protect mouth and nose and respiratory tract from infectious agents. § § Goggles; to protect eyes Face shields; to protect face, mouth, nose and eyes.

PPE § Do not wear masks around the neck outside the OR suite. § Wear gowns and gloves for patients on Contact precaution. § Keep gloved hands away from face to prevent contamination.

SEQUENCE FOR DONNING PPE 1. 2. 3. 4. Gown Mask Goggles Gloves

HAND TO SURFACE TRANSMISSION § Gloved hands should be treated the same as bare hands. § Gloves also become contaminated and should be considered a reservoir for pathogens. § Change gloves often and use hand hygiene before and after glove use.

PATHOGEN TRANSMISSION AND ENVIRONMENTAL CLEANING § Organisms are spread most often by skin to skin contact, mostly by the hands. § They can also be transmitted from contaminated surfaces to the hands or gloves of healthcare workers. § In one study, 42% of nurses contaminated their gloves by touching objects in a MRSA room without touching the patient.

IS HAND HYGIENE ENOUGH? § It’s a start, but not enough § As long as the environment is inadequately cleaned, hands will be contaminated seconds after they are washed § A Johns Hopkins Hospital study found 26% of the supply cabinets were contaminated with MRSA and 21% with VRE.

SURVIVAL OF PATHOGENS ON ENVIRONMENTAL SURFACES Pathogen § § § C. Diff S. Aureus E. Coli Norovirus Influenza Presence on Surface > 5 months 7 months up to 16 months 3 months 1 -2 days

INJECTION SAFETY



§ Follow the injection safety guidelines from the CDC § One Needle, One Syringe, Only One Time…

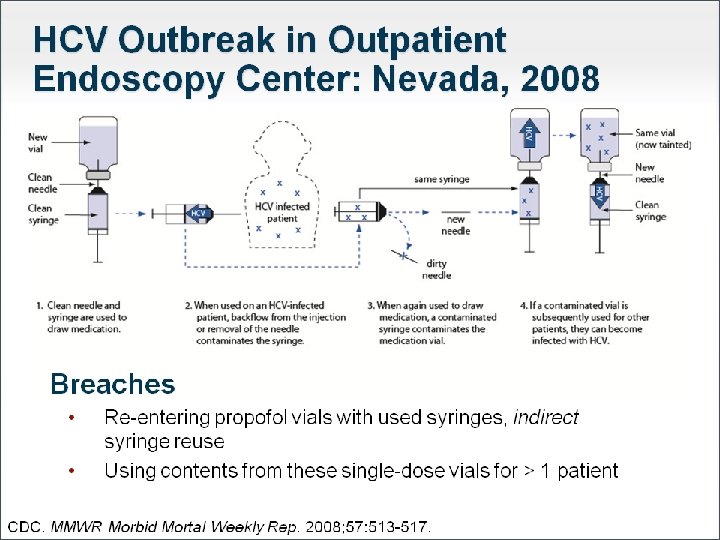
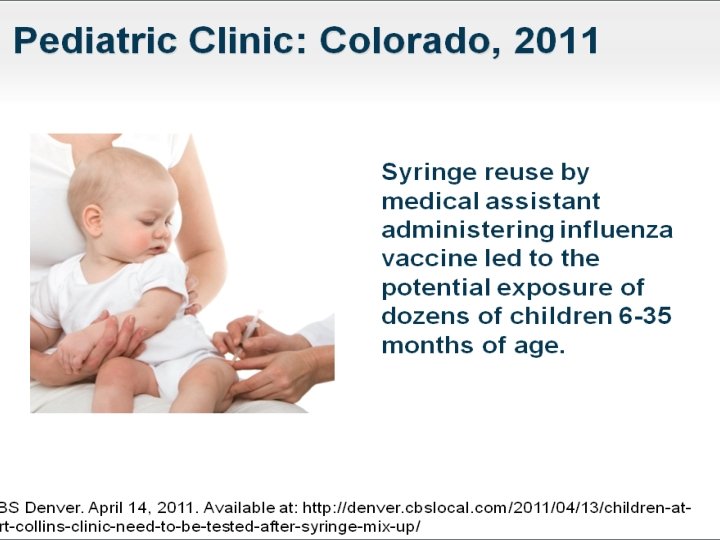
THE ONE AND ONLY CAMPAIGN § Since 1999, more than 130, 000 patients in the United States have been notified of potential exposure to hepatitis B virus (HBV), hepatitis C virus (HCV), and HIV due to unsafe injection practices. § Many of these incidents involved healthcare providers reusing syringes, resulting in contamination of medication vials or containers which were used then on subsequent patients.

THE ONE AND ONLY CAMPAIGN § 1% to 3% of healthcare providers still reuse the same needle and/or syringe on multiple patients.

THE ONE AND ONLY CAMPAIGN § The goal of the One & Only Campaign: 1. To ensure that every injection administered to patients is safe. 2. The Campaign aims to empower patients to ask questions and re-educate healthcare providers regarding safe injection practices.

Injection safety guidelines from CDC ■ Never administer medications from the same syringe to more than one patient, even if the needle is changed. ■ After a syringe or needle has been used to enter or connect to a patient’s IV it is contaminated and should not be used on another patient or to enter a medication vial.

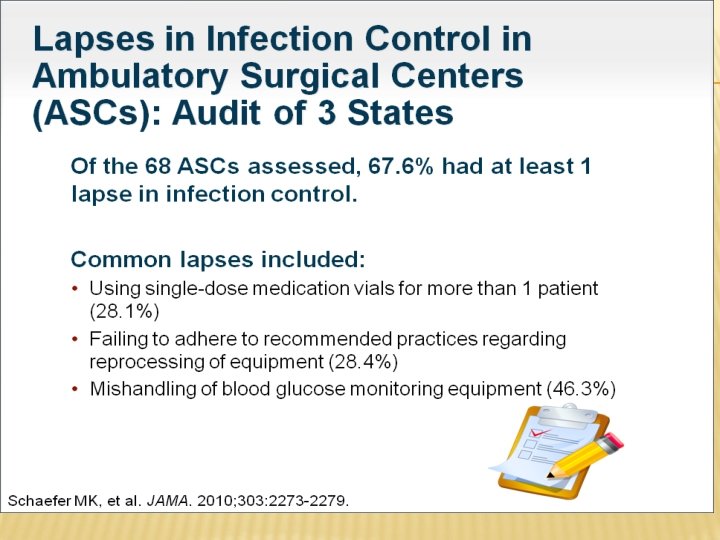
■ Never enter a vial with a used syringe or needle. ■ Never use medications packaged as single-dose vials for more than one patient.

THE ONE AND ONLY CAMPAIGN Three things every provider needs to know about injection safety : 1. Needles and syringes are single use devices. They should not be used for more than one patient or reused to draw up additional medication. 2. Do not administer medications from a single-dose vial or IV bag to multiple patients. 3. Limit the use of multi-dose vials and dedicate them to a single patient whenever possible.

§ Remember: § ONE Needle, § ONE Syringe, § ONLY ONE Time.
Avoid the use of needles where safe and")
NINE STEPS TO AVOID NEEDLESTICKS 1. )Avoid the use of needles where safe and effective alternatives are available. 2. )Help your employer select and evaluate devices with safety features. 3. )Use devices with safety features provided by your employer. 4. )Avoid recapping, bending, or removing used needles.
Plan safe handling and disposal before beginning any procedure using needles. 6. )Dispose")
5. )Plan safe handling and disposal before beginning any procedure using needles. 6. )Dispose of used needle devices promptly in appropriate sharps disposal containers. Change containers when full, don’t leave it for the next person to do 7. )Report all needlestick and other sharpsrelated injuries promptly.
Tell your employer about hazards from needles that you observe in your work")
8. )Tell your employer about hazards from needles that you observe in your work environment. 9. )Participate in bloodborne pathogen training and follow recommended infection prevention practices, including hepatitis B vaccination.

EVALUATION AND USE OF SAFETY DEVICES § § Be aware of all safety devices in use and how to use them. Then, USE THEM -CORRECTLY! If you do not like the way a safety device works, let management know so we can evaluate other alternatives.

POINTS TO TAKE AWAY § Everyone is responsible as a team to ensure the safety of the patient as well as your co workers and yourself. § Know your job and take pride in a job well done. § Safe injection practice should be a priority for patient safety and infection prevention. § Something as simple as hand hygiene can prevent infection so do it often.

Bloodborne Pathogen Exam 1. You should always treat an unidentified body fluid or substance as infectious. a. True b. False 2. Your employer must offer the hepatitis B vaccine to all employees who may be exposed to blood or bodily fluids on the job within 10 days of employment. a. True b. False 3. Health care facilities can choose whether or not to comply with OSHA’s bloodborne standard. a. True b. False 4. How are bloodborne pathogens transmitted? a. Needlesticks, cuts b. Splashes, sprays c. All of the above

Bloodborne Pathogen Exam 5. OSHA stands for which agency? a. Oregon State Health Agency. b. Occupational Safety and Health Administration. c. Oregon Sharps and Health Administration. d. None of the above. 6. To prevent exposure to BBP: a. Use Standard Precautions. b. Follow proper procedure including; sharps safety, hand hygiene, and PPE. c. Avoid all patient care/contact. d. a and b 7. Use PPE: a. Only in the OR. b. When there is a risk of exposure to blood or body fluids. c. All of the time.
 treats all blood and")
Bloodborne Pathogen Exam 8. Standard precautions (created by the CDC) treats all blood and body fluids as infectious and also includes transmission based precautions such as airborne, droplet, and contact. a. True b. False 9. The best way to prevent the spread of BBP is to: a. Follow Universal or standard precautions. b. Use PPE and hygiene. c. Observe safe needle practice. d. All of the above. 10. Eating and drinking is acceptable in areas where there is a possibility of blood/body fluid contamination as long as you keep it hidden and are careful. a. True b. False

Cultural Competence in Healthcare An Important Refresher for Physicians

Session Objectives After this session physicians will be able to: Define Cultural Competence Describe why delivering Culturally Competent Care is important Understand being Culturally Competent is a continual process Use Culturally Competent Practices in the provision of care

Why do we focus on Cultural Competence at Bend Surgery Center? It is our Mission • “to provide a safe, comfortable and healthy patientfocused environment, promoting exceptional, outpatient care in a physician owned ambulatory surgery. ” Important Clinical Excellence • Ensure equal and individualized care is delivered to all patients Our Patient and Family Experience • Nothing is more important than our patient’s health and well being reminder! Culturally competent care meets the needs of our cultura lly diverse patient population !

The next few slides are common words and information to help you learn more about what cultural competence is and why it matters in healthcare and the workplace

What is Culture? It is the learned and shared values of a particular group that: - Guides thinking - Actions - Behaviors - Emotional reactions to daily living It is the sum of beliefs, practices, habits, likes and dislikes. It is norms and customs that are learned.

Culture is central to the Delivery of Healthcare • It influences patients’ healthcare beliefs, practices attitudes toward care, and trust in the system and in the individual providers • Cultural differences affect how health information and healthcare services are received, understood and acted upon. *US Department of Health & Human Services/ Office of Minority Health

Our Patients Represent Many Cultures Group Percentage of Oregon Residents White alone 87. 9% American Indian Black or and African Alaska American Native alone 2. 0% 1. 8% Asian alone Native Hawaiian and Other Pacific Islander alone Two or More Races 4. 3% 0. 4% 3. 6% White alone, not Hispanic or Latino 12. 5% 77. 0%

Our Patients Represent Many Religions and Languages Religions Apostolic Church of God Greek Orthodox Methodist Baptist Congregational Hindu, Hmong Mormon Buddhist Eastern Orthodox Jehovah’s Witness Muslim/Islam Catholic Episcopal Jewish Pentecostal Lutheran Presbyterian Christian Science Evangelical Languages Arabic Farsi Japanese Serbian Bosnian French Laotian Sign language Chinese Greek Polish Spanish Danish Hebrew Punjabi Somali Bantu English Italian Russian Vietnamese

What is Cultural Competence? Cultural competence is the ongoing capacity of healthcare systems, organizations and professionals to provide for diverse patient* populations high quality care that is safe, patient- and family- centered, evidence-based, and equitable The National Quality Forum * The term “patient” refers to the individual recipient of care – i. e. patient, client, legal surrogate or person.

Cultural Competence in Health Care Primary concerns: 1. Eliminate misunderstandings in diagnosis or in treatment planning that may arise from differences in language or culture 2. Improve patient adherence with treatments 3. Eliminate health care disparities

Associations We Make What type of person do you think of when you hear the following descriptions? • • • Alzheimer’s patient Black male Asian man Welfare recipient Teenager

Associations We Make The people shown below fit into the descriptions reviewed on the previous slide Alzheimer’s victim Black male Asian man Welfare recipient Teenager President Ronald Reagan Dr. Ben Carson Jackie Chan JK Rowling Ferris Bueller

Associations We Make • When we initially hear the profile of a patient, we all make associations and assumptions based on our past experience. We have a perception of the person before we ever meet them. • Our patients make the same associations when they meet us. • This can be described as a component of transference and counter-transference.

Transference • Transference occurs when the physicians or patients transfer past emotions, beliefs or experiences to the present situation. • The feelings can be positive or negative(Countertransference), but are ALWAYS a distortion of reality. • Transference is an unconscious process. When transference occurs around cultural issues, it becomes a serious barrier that keeps the patient from being receptive to medical advice and treatment. It is up to us as Culturally Competent Providers to maintain and convey unconditional positive regard for our patients The American Journal of Psychiatry, VOL. 157, No. 9

Cultural Competence is a Continuum • Gaining cultural competence is an ongoing PROCESS. It is developed as cultural knowledge increases • In order to achieve higher levels of competence, it is helpful to engage in self assessment SKILLS • Self assessment provides direction for improvement ATTITUDES KNOWLEDGE The Center for Public Health Education

Cultural Competence is a Continuum Moving From Basic Knowledge to Clinical Practice KNOWLEDGE ATTITUDES Understanding the meaning of culture and its importance to healthcare Having respect for variations in cultural norms SKILLS Eliciting patients’ explanatory models of illness Physicians must continue skill development to learn each culture Journal of the Nation Medical Association, Nov. 2008

Eliciting Patient’s Explanatory Model of Illness Role of the Physician. . 1. Asking questions to elicit the patient’s understanding of their illness 2. Having strategies for identifying and bridging the different communication styles 3. Having skills for assessing decision-making preferences and the role of family Journal of the Nation Medical Association, Nov. 2008

Eliciting Patient’s Explanatory Model of Illness 4. Utilizing techniques for ascertaining the patient’s perception of using biomedicine and his or her use of complementary and alternative medicine 5. Having tools for recognizing sexuality and gender issues 6. Having communication strategies for negotiating 7. Methods for bringing to bear an awareness of issues of mistrust and prejudices and of the impact of race and ethnicity on clinical decisionmaking Journal of the Nation Medical Association, Nov. 2008

The Culturally Competent Physician • Knows competency involves a deeper commitment to the people for whom we provide services • Recognizes and learns to work within the context of different languages, customs, worldviews, religions, spiritual views, health beliefs, gender roles, sexuality and family relationships when interacting with clients/patients • Develops specific practice skills The Center for Public Health Education

The Culturally Competent Physician • Practice Skills - Has an awareness and acceptance of difference whereby diversity is valued - Understands how his own culture influences how he thinks, acts and delivers services - Understands the dynamics of difference and is conscious of those dynamics inherent when cultures interact The Center for Public Health Education

The Culturally Competent Physician • Becomes familiar with the different aspects of various cultures in target areas where service is provided • Has the ability to adapt practice skills that fit the cultural context of the patient/client Physicians must continue skill development to learn each culture The Center for Public Health Education

Why is this important for Physicians? At Bend Surgery Center, we recognize our patients as individuals with unique physical, emotional, spiritual, and cultural needs. As a compassionate, health care provider, we believe developing a positive relationship with our patients and families is essential to the healing process and key to carrying out our Mission of promoting exceptional, outpatient care in a physician-owned ambulatory surgery.

The Goal of Each Physician To always provide culturally competent health care services that are respectful of and responsive to the health beliefs, practices, cultural and linguistic needs of our diverse patients.

Pain Management at Bend Surgery Center

Pain Management Policy All patients must have effective pain management Appropriate screening and pain assessment Documentation Care and treatment Pain education Patient self report of pain must be source of assessment whenever possible Patient’s acceptable level of pain must guide treatment

Determination of Pain Patient self report of pain must be source of assessment whenever possible Patient’s acceptable level of pain must guide treatment If the patient is unable to self report, assessment strategies should include: Observable behaviors (facial expressions, body movements, crying) Physiological measures (heart rate and blood pressure).

What is Pain? �“An unpleasant sensory and emotional experience associated with actual or potential tissue damage, or described in terms of such damage. ” International Association for the Study of Pain (Merskey, 1979) �Pain is always subjective. �The patient’s self-report of pain is the single most reliable indicator of pain. �The clinician must accept the patient’s self report of pain.

Acute Pain Acute pain presents most often with a clear cause, relatively brief in duration and subsides as healing takes place. Acute pain is often accompanied by observable objective signs of pain increased pulse rate increased blood pressure Non-verbal signs and symptoms such as facial expressions and tense muscles.

Chronic Pain that is persistent and recurrent. When pain persists, it serves no useful purpose and may dramatically decrease the quality of life and function. Chronic pain rarely has any observable or behavioral signs although persons may appear anxious or depressed.

Cancer Pain that is associated with cancer or cancer treatment. May be attributed to: Tumor location Chemotherapy Radiation therapy Surgical treatment
 Intensity Sensory quality Alleviating and aggravating")
Pain Assessment �Initial Pain Assessment should include: Location(s) Intensity Sensory quality Alleviating and aggravating factors � Any new onset of pain requires a new comprehensive pain assessment.

Pain Reassessment �Every 1 hour minimally �Following the administration of pain medications to determine the effectiveness of the medication and/or need for further intervention. IV within 15 mins of administration PO/IM/SC within 1 hour of administration
 �Term used to document pain in a patient who")
Assume Pain is Present (APP) �Term used to document pain in a patient who cannot self report pain. �Because of injuries or the nature of a procedure the patient would be assumed to have pain.
 �A behavioral scale for scoring pain in individuals")
FLACC: (Face, Legs, Activity, Cry, Consolability) �A behavioral scale for scoring pain in individuals who are unable to self-report pain. �Used for age two months to seven years �May have use beyond this age for the cognitively impaired patient

OAAS: Observer’s Assessment of Alertness and Sedation �A tool used to assess patients level of sedation. �May be used to guide titration of pain medication.

Pain Management Approach Should be interdisciplinary and multimodal. Care is individualized and may depend on: Pain source and intensity Patient’s age Developmental, physical, emotional and cognitive status Cultural beliefs Treatment preferences Concurrent medical conditions

Multimodal Analgesia This term describes the use of multiple modalities that are used to provide pain relief with various parts of the pain pathway targeted. Decreased dependence on single modality agents decreases the risk of side effects. May include: Pharmacological (opioids, NSAIDS, gabapentanoids) Relaxation techniques (biofeedback, deep breathing) Regional analgesia (nerve blocks, epidural catheters)

Treatments May Include: Non-pharmacologic Methods • • • Heat/cold Relaxation Distraction Guided imagery Acupressure/acupuncture Repositioning Pharmacologic Methods �NSAIDS �Anti-seizure medications �Anti-depressants �Opioid analgesics �Local anesthetics �Neurolytics

Acute vs. Chronic Pain Management Chronic Pain Acute Pain Most often treated with: NSAIDS Opioids Local anesthetics Splinting Positioning changes Ice �Most often treated with: Anti-seizure medications Anti-depressant medications NSAIDS Implantable devices Psychological therapy Acupuncture �When all else fails and benefits outweigh risks: Opioids

Responsible Opioid Prescribing There is a national epidemic occurring involving the misuse, abuse and diversion of prescription opioids. The majority of these medications enter circulation through the legitimate prescription by physicians from all specialties. Prescribers must be aware that their opioid prescription could potentially end up being used for reasons not prescribed (sold, snorted, traded).

Responsible Opioid Prescribing Assess risk for opioid abuse or diversion prior to prescribing opioid. Risk factors for misuse or abuse of opioids include the following: Males between 18 and 45. A personal history of substance abuse A family history of substance abuse A personal history of preadolescent sexual abuse A personal history of psychological disease (depression, anxiety, obsessive-compulsive disorder

Responsible Opioid Prescribing Doctor Shopping Using more than one doctor to obtain opioids Prevent by checking databases External medication history on EMR Oregon State Prescription Drug Monitoring System http: //www. orpdmp. com/ Phone: 866 -205 -1222 Email: orpdmp-info@hidinc. com

If you have any questions or would like a hardcopy of this training, please visit the Administration office Or Email info@bendsurgery. com
- Slides: 125