EXTRAPYRAMIDAL SYSTEM and BASAL GANGLIA Burcu Ugurel MD

EXTRAPYRAMIDAL SYSTEM and BASAL GANGLIA Burcu Ugurel, MD Department of Neurology

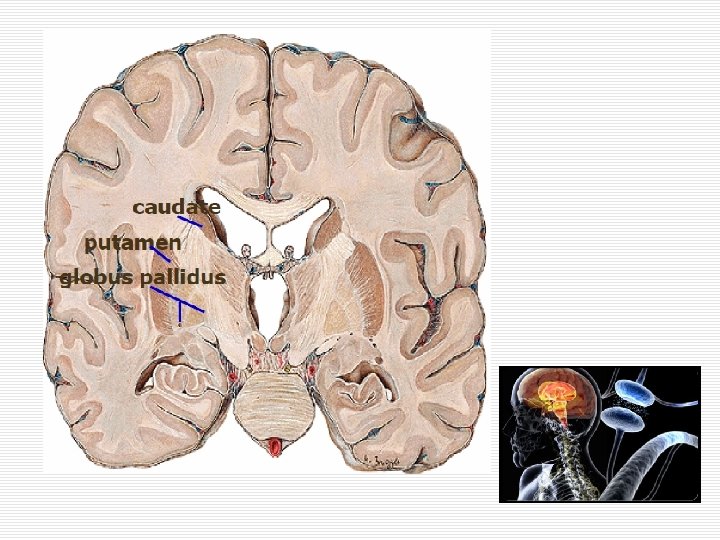
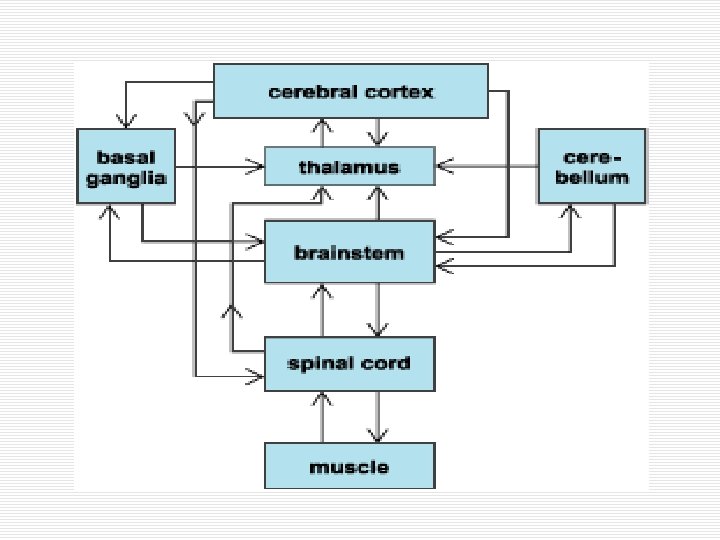
Extrapyramidal System o Motor functions are managed by 2 main system n Pyramidal system o Corticospinal tract n Extrapyramidal system o Basal ganglia n caudate n putamen n globus pallidus

Neurotransmitters/Neuromodulators at Basal Ganglia o GABA inhibitory o Glutamate excitatory o Dopamine n D 1 receptors excitatory n D 2 receptors inhibitory o Acetylcholine modulator n Not excitatory or inhibitory n It changes excitability

Motor Functions of the Basal Ganglia o The initiation and planning of movements o Adjusting speed and magnitude of movement o Automatically implementation of learned motor programs (walking, cycling, etc. ) o Implementation of consecutive or simultaneous movements o Adjustment of muscle tone o Truncal stability

CLASSIFICATION of the MOVEMENT DISORDERS o Movement disorders are classified according to dominant abnormal or involuntary movements n hypokinetic (reduced movement) n hyperkinetic (increased movement)

HISTORY at the MOVEMENT DISORDERS o Determine of the affected body region or regions n In one region o focal n Multiple regions adjacent to each other o segmental n multiple regions independent from each other o multifocal n If entire body is affected o generalized n Predominantly distal or proximal

HISTORY at the MOVEMENT DISORDERS o Does it occur at rest or on movement n Essential tremor typically occurs during the motion, disappears at rest n Opposite for Parkinson's tremor

HISTORY at the MOVEMENT DISORDERS o speed of movement n Myoclonus fast as lightning n Korea fast n Atetoz slow-flowing o Rhythmicity and continuity n Tremor rhythmic n Korea and myoclonus arrhythmic

HISTORY at the MOVEMENT DISORDERS o The emergence or aggravation with certain postures n orthostatic tremor occurs with a fixed standing o Most of them disappear during sleep o Some of them continue during sleep n palatal tremor o Some of them occur when just passing off to sleep or during sleep n Restless legs syndrome n Periodic limb movements of sleep

HISTORY at the MOVEMENT DISORDERS n The presence of sensory symptoms before involuntary movement n Suppresses involuntary movement as a voluntary n The presence of factors that starting, worsening or correcting of involuntary movements o Tic disorders

HAREKET BOZUKLUKLARI o The first step at diagnosis; n Basic movement disorder should be identified and named as a phenomenological o Tremor, dystonia, bradykinesia, etc.

HYPOKINETIC MOVEMENT DISORDERS

HYPOKINETIC MOVEMENT DISORDERS o Akinetic-rigid syndromes o Clinical features n n Decreases of motion Difficulties on motion Slowdown Increased muscle tone o Parkinson's syndrome is prototype of Akinetic-rigid syndromes

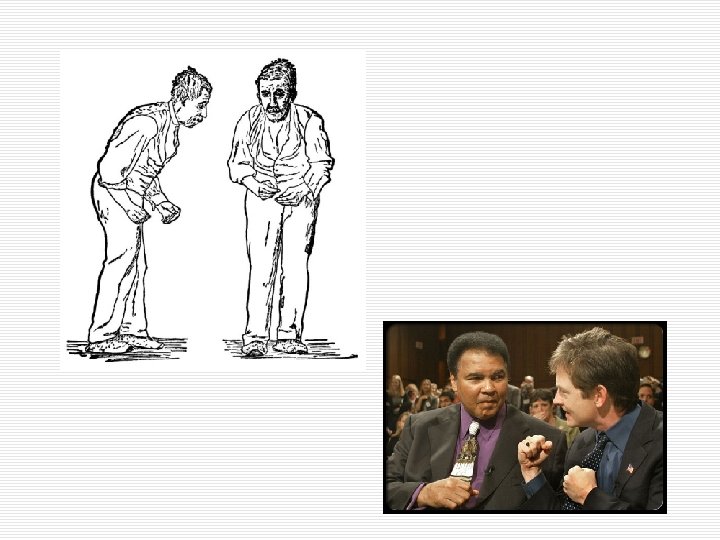
Parkinson’s Syndrom o Symptoms n n Bradykinesia-akinesia Rigidity Postural instability Resting tremor may be accompanied, but it is not necessary
, n Parkinson's plus")
Parkinson’s Syndrom Aetiological Classification o Degenerative n Idiopathic Parkinson's Disease (IPD), n Parkinson's plus syndromes n other degenerative diseases associated with parkinsonism Underlying pathology of these diseases are degenerative cell loss and not be detected in another reason o Symptomatic
 2 - Parkinson's plus syndromes")
Parkinson’s Syndrom DEGENERATİVE 1 - Idiopathic Parkinson's disease (IPD) 2 - Parkinson's plus syndromes multisystem atrophy Progressive supranuclear palsy corticobasal degeneration Lewy Body Dementia 3 - Parkinsonism associated other degenerative diseases Spinocerebellar ataxia type 2, 3, 17 Huntington's Disease Striapallidodentat bilateral calcinosis (Fahr's Disease) Hemiparkinson-hemiatrofi syndrome Frontotemporal dementia-parkinsonism complex Dentatorubropallidolusian atrophy Pallidal degeneration Striatal necrosis associated mitochondrial diseases Pantothenate kinase associated neurodegeneration Nöroakantositoz

Parkinson’s Syndrom Symptomatic 1 - Vascular (small vessel disease-related subcortical encephalopathy, multiple lacunar infarcts, basal ganglia and Brainstem hemorrhages and infarcts) 2 - Normal pressure hydrocephalus 3 - Tumors 4 - Drug-induced (neuroleptics, dopamine exhausting drugs, calcium channel blockers, antiemetics, valproic acid, lithium) 5 - Intoxications (carbon monoxide, manganese, potassium permanganate, ephedrine abuse, mercury and other heavy metals, organic solvents, paint thinner, carbon disulfide, MPTP, cyanide) 6 - Infections (encephalitis, prion disease, neurosyphilis, toxoplasmosis) 7 - Metabolic causes (hypoxia, hypoparathyroidism, extra-pontine miyelinozis, chronic liver disease, Wilson's disease) 8 - Head injury, dementia pugilistica (boxer) 9 - Demyelinating Diseases 10 - Psychogenic Parkinsonism

IDIOPATIC PARKINSON’S DISEASE o Constitutes 80 -85% of parkinsonism o The average of onset is 50 -60 years n Early-onset <40 years n Juvenile <20 years o Loss of dopaminergic cells containing melanin in the substantia nigra pars compacta o Lewy bodies o When dopaminergic cell loss reach to 60 -70%, clinical symptoms start to occur

Pathology of Parkinson's disease

IDIOPATIC PARKINSON’S DISEASE o The cardinal symptoms of Parkinson's disease n Bradykinesia + n Rigidity n Tremor n Postural instability *Not need to be all-in-one *The disease often begins from half of the body asymmetrically

IDIOPATIC PARKINSON’S DISEASE o Other clinical symptoms of Parkinson's disease n n n n n Anteflexion posture Freezing phenomenon Gait disorders Speech disorders Micrography, dysphagia Autonomic disorders Mental-emotional symptoms Sleep disorders Odor and visual perception disorders

IDIOPATIC PARKINSON’S DISEASE o Non-motor symptoms n REM sleep behavior disorder n Loss of smell sense (anosmia) n constipation These symptoms can occur many years before from the start of the motor symptoms n Parkinson's disease dementia reaches to 5080% on fifteenth-twentieth years

IDIOPATIC PARKINSON’S DISEASE o Tremor n Can be seen as resting/postural /re-emergen tremor n Often, the first clinical finding is motor symptoms, 15% never seen n Frequency is 4 -6 Hz n Usually emerges on the hands, sometimes on the feet, tongue, jaw and lip n Audio and head tremor never emerges n Increases with stress, mental activity and walking

IDIOPATIC PARKINSON’S DISEASE

IDIOPATIC PARKINSON’S DISEASE o Bradykinesia / Akinesia n The most characteristic symptom of basal ganglia disorders n Presence is necessary for the diagnosis n Bradimimi, micrography, decrease of associate movements and sialorrhoea develop because of this symptom n The most basic symptom that creates disability

IDIOPATIC PARKINSON’S DISEASE o Rigidity n Develops as a result of simultaneous increased tone of agonist and antagonist muscles n May be located in the proximal or distal n Shows cogwheel rigidity n Determines by passive motion n Increases with other extremity movement (Froment's sign) n Patients describe as a stiffness or hardness

IDIOPATIC PARKINSON’S DISEASE o Postural instability n The least specific symptom but the most common cause of disability n Occurs in later stages of the disease n Occurs due to loss of postural reflex n The most common cause of falls n Pull test is used for diagnosis n Leads to sitting as a block
 o Dopamine can not")
PARKINSON’S DISEASE TREATMENT o Dopaminergic Treatment n Levodopa (dopamine precursor) o Dopamine can not pass the blood brain barrier, levodopa may o Used with peripheral type inhibitors of dopa decarboxylase (benserazide or carbidopa) in order to prevent peripheral side effects of dopamine and increase the amount of levodopa pass through to the brain n These substances can not pass the blood brain barrier so do not prevent translation of Levodopa to dopamine in the brain o Due to the long-term side effects may not prescribed initially n Dyskinesias, such as on-off period

PARKINSON’S DISEASE TREATMENT o Dopamine agonists n These drugs mimic the effect of dopamine binding to dopamine receptors o o o o Bromocriptine (Parlodel) Lisuride (Dopergin) Pergolide (Permax) Piribedil (Trivastal) Cabergoline (Cabaser) Ropinirole (Requip) Piramipexola (Pexola, Parkyn)

PARKINSON’S DISEASE TREATMENT o Anticholinergic agents n Re-provide deteriorated balance between dopamine and acetylcholine in the basal ganglia o Biperiden (Akineton) o Bornaprin (Sormodren) o Triheksifenidil (Artane)

PARKINSON’S DISEASE TREATMENT o MAO-B inhibitors n Main enzyme which destroyed the dopamine n Dopamine stays in the synaptic gap for longer time o Selegiline (Moverdin, seldepar) o Rasajilin (Azilect)
 n Tolcapone o Amantadine (PK-Mertz)")
PARKINSON’S DISEASE TREATMENT o COMT inhibitors n Entacapone (Comtan) n Tolcapone o Amantadine (PK-Mertz)

PARKINSON’S DISEASE TREATMENT o SURGICAL n The target part varies according to symptoms on the foreground o Thalamus o o The globus pallidus internus Subthalamic nucleus n Destruction of these regions o Stereotactic surgery o Gamma-knife n Deep brain stimulation o High-frequency electrical impulses via deep electrodes reduce the activity of the cells in these regions

PARKINSON PLUS SYNDROMS o Common features n Classic signs of Parkinson's syndrome (bradykinesia, rigidity, tremor, postural reflex abnormalities) + n Additional signs and symptoms

PARKINSON PLUS SYNDROMS o Multisystem Atrophy n MSA-P n MSA-C o Progressive Supranuclear Palsy o Corticobasal Degeneration o Lewy Body Dementia

HYPERKINETIC MOVEMENT DISORDERS

DYSTONIA o Characterized by involuntary, continuous, twisting, rotating muscle contraction o Develops as a result of simultaneous contractions of agonist and antagonist muscles o Recurrent o Results with temporary or permanent abnormal postures o Disappears during sleep o Dystonic contractions temporarily loss with touch n Sensory trick
 Dystonia o Idiopathic torsion dystonia (most common) n Dystonias of childhood o")
Primary (Idiopathic) Dystonia o Idiopathic torsion dystonia (most common) n Dystonias of childhood o Usually begins in one extremity often in leg, o Spreads to the other limbs and sometimes cranial muscles within months or years n Dystonias which start over the age of 40 o Often focal or segmental, o Primarily keeps cranio-cervical muscles
 Dystonia Dopa Responsed Dystonia ( Segawa disease) o Autosomal dominant (30 -40%")
Primary (Idiopathic) Dystonia Dopa Responsed Dystonia ( Segawa disease) o Autosomal dominant (30 -40% penetrance) o Usually begins in childhood in the lower extremity with dystonia o There is no involvement of the cranial regions o Shows diurnal fluctuation (less complaint in the morning, dopamine stores run out in the evening and complaint increases) o Good response with low-dose L-dopa (50 -250 mg) o L-dopa therapy should be tried for all kinds of primary dystonia in childhood
 Dystonia Focal Dystonia o Hemifasyal Spasm n Only on half of the")
Primary (Idiopathic) Dystonia Focal Dystonia o Hemifasyal Spasm n Only on half of the face n May be continuous or intermittent n Semi-rhythmic contractions o Blepharospasm n Increasing of eye blink frequency functional blindness o Oromandibulolingual Dystonia n Dystonia around the mouth-jaw-tongue o Laryngeal Dystonia (pasmodic Dysphonia) n Difficulty of voicing and speech
 Dystonia Focal Dystonia o Focal Dystonia (more) n Cervical Dystonia (spasmodic torticollis)")
Primary (Idiopathic) Dystonia Focal Dystonia o Focal Dystonia (more) n Cervical Dystonia (spasmodic torticollis) o o Torticollis Laterocollis Anterocollis Retrocollis n "Task Specific” dystonia o Characterized by excessive muscle contractions producing abnormal postures during selective motor functions o The most common "writer's cramp"
 Autosomal recessive Usually starts between the age of")
Symptomatic Dystonias Wilson's disease (hepatolenticular degeneration) Autosomal recessive Usually starts between the age of 10 -20 Depends on disorder of copper metabolism Copper precipitates on liver, brain and kidney All kinds of movement disorders seen due to involvement of basal ganglia o Behavioral and mental problems o Kayser-fleischer ring o o o

 n Should be investigated WD all kinds of")
Symptomatic Dystonias o Wilson's Disease (more) n Should be investigated WD all kinds of movement disorders in childhood and adolescence o Laboratory investigations n n Level of serum ceruloplasmin is low Level of free copper in serum is high Total amount of copper in serum decreased 24 -hour urine copper excretion is increased

Treatment of Dystonia o Treatment of symptomatic dystonias aimed at reason o idiopathic dystonia n n n Anticholinergics Antidopaminergics (neuroleptics) Baclofen Benzodiazepines Botulinum toxin o In general, the first choice is drug for generalized dystonias, and botulinum toxin for focal dystonias

CHOREA and BALLISM o Arrhythmic, rapid, saltatory or smooth, simple or complex properties Chorea o Amplitude is smaller o Usually seen in distal of extremity n Ballism o Amplitude is greater o Usually seen in proximal of extremity n

CHOREA and BALLISM Huntington's disease o Clinical features; n Korea is the dominant movement disorder o chorea, dystonia, parkinsonism n Psychiatric findings n Dementia o Autosomal dominant o Increased number of CAG repeat o Predictive, and prenatal diagnosis is possible
 n One")
CHOREA and BALLISM Sydenham's Chorea (Rheumatic chorea, St. Vitus dance, chorea minor) n One of the major criteria of acute rheumatic fever (group A streptococcus) n Usually seen between 5 -15 years old, F>M n Chorea starts suddenly or step by step and tends to be rapidly generalized n The most intense in first 3 -6 months, usually resolve within 6 -9 months

TREMOR o Tremor, n is involuntary, rhythmic oscillations n occur as a result of alternating or synchronous contraction of the reciprocal muscles

Tremor According to etiology and clinical symptoms Physiological tremor o Occur with normal muscle contraction o 10 -12 hz, postural tremor with low-amplitude o Etiology n Mental reasons (anxiety, stress, fatigue), n Metabolic causes ( fever, thyrotoxicosis, hypoglycaemia, ect. ), n Drugs (neuroleptics, beta-adrenergic agonists, valproic acid, lithium, steroids, dopamine agonists, antidepressants), n Toxins (mercury, lead, arsenic) n Some food ingredients (caffeine) May lead to increased physiological tremor

Tremor According to etiology and clinical symptoms Essential Tremor o Begins as an asymmetric and postural tremor unilaterally, gradually spread to other part of body o Always bilaterally o İncreases with action and decreases at rest o In general, frequency is fast (4 -12 hz) o More than half of the patients have family history (variable penetrance) o May significantly impair the quality of life

Tremor According to etiology and clinical symptoms o Treatment of Essential Tremor n May use heavy bracelets and heavy cups while drinking or writting n Alcohol? n Beta-adrenergic blockers (dideral) o Heart failure, AV block, asthma and diabetes are relatively contraindicate n Primidone (mysoline) o May does serious sedation, should be initiated with low doses n Surgical o Thalamic stimulation

TIC DISORDERS o May suppress as a voluntary for a short time o Unbearable desire to motion from the inside o Involuntary movement (motor tics) or sound (vocal tics) n n n Short Non-rhythmic Stereotypic As appears aimless Sudden

TIC DISORDERS Simple tics o Motor tics n n blinking grinning mouth opening shoulder shaking o Vocal tics n primitive sounds n throat clearing n sniffle Complex tics o Motor tics n n n touching, tapping sniffing clap echopraxia (repeating the same movement) copropraxia (swearinglike movements) o Vocal tics n n n singing whistle echolalia palilalia (repeat themself) koprolali (swearing)
, as fast as lightning o Form of throwing,")
MYOCLONUS o Sudden, short-term (<100 ms), as fast as lightning o Form of throwing, jumping n Positive myoclonus o The sudden contraction of a particular muscle group n Negative myoclonus (asterixis) o Sudden relaxation of the muscles which maintain a posture

MYOCLONUS o Physiological myoclonus n While falling asleep, after excessive exercise , in anxiety o Essential myoclonus n No pathological signs and symptoms other than myoclonus n Reduce the symptoms with Alcohol is typical o Symptomatic myoclonus n During the course of diseases such as Liver failure, uremia, electrolyte imbalance, poisoning, head trauma, hypoxic-ischemic ensafalopati (Lance-Adams syndrome), neurodegenerative diseases, central nervous system infections, prion diseases

SLEEP-RELATED MOVEMENT DISORDERS o Restless Legs Syndrome n Unidentified leg discomfort at rest or before sleep o Periodic limb movements of sleep n Semirhythmic involuntary movements during sleep especially in the feet

DRUG RELATED MOVEMENT DISORDERS o Acute Dystonic Reactions n Within a few hours after drug intake n Especially around the head, neck, face, tongue and mouth n Form of dyskinetic and dystonic involuntary movements o Subacute Parkinsonism or Akathisia n Neuroleptic use in the last 1 -3 months n Usually reversible o Tardive Syndromes n As a result of long-term use of neuroleptic n Sometime irreversible

PSYCHOGENIC MOVEMENT DISORDERS o o o o Can mimic all kinds of movement disorders such as dystonia, myoclonus, tremor, tic disorder Symptoms onset suddenly Emerge after psychic trauma Produce serious handicaps Demonstrate an outlook except usual form Out of the anatomical and pathophysiological patterns If the patient's attention is disintegrated, symptoms ameliorate There are some periods of self-improvement Positive response to placebo treatment The presence of secondary gain The detection of patients with symptoms of psychopathology in favor of Neurological examination is completely normal The presence of symptoms that suggestive psychopathology
- Slides: 62