Exercise training in diabetes Prof dr Dominique Hansen

Exercise training in diabetes Prof. dr. Dominique Hansen

Obesity epidemic

Obesity epidemic Prevalence of obesity and severe obesity 2008– 30 in USA

Obesity epidemic

Diabetes epidemic

Diabetes epidemic

Diabetes epidemic

Diabetes epidemic European Opinion Research Group: Eurobarometer Report 2014

Exercise: why? EXERCISE TRAINING = INVESTMENT IN MORE AND BETTER TIME

Exercise: why?

Exercise: why?

Exercise: why?

Exercise in type 2 diabetes: why? Prevention of type 2 diabetes – 3234 glucose-intolerant subjects Daily metformin intake = -33% T 2 DM incidence Change in lifestyle = -58% T 2 DM incidence Knowler et al. N Engl J Med 2002; 346: 393

Exercise in type 2 diabetes: why? Prevention of type 2 diabetes Through exercise training only? 37 -49% risk reduction Laaksonen DE, et al. Diabetes 2005; 54: 158 -65

Exercise in type 2 diabetes: why? • In 1982 it was found how blood glucose content could decrease as result of exercise – Elevation of skeletal muscle insulin sensitivity – Richter EA, et al. J Clin Invest 1982; 69: 785 -93 – Richter EA, et al. Am J Physiol 1984; 246: E 476 -82 – Elevation of skeletal muscle glucose uptake…but also by a noninsulin dependent pathway – Garetto LP, et al. Am J Physiol 1984; 246: E 471 -5 – Glucose utilisation could increase 20 -fold as result of exercise

Exercise in type 2 diabetes: why? 13. 30 h hyperglycemic 0. 4 h hyperglycemic Praet et al. Clin Sci 2006; 111: 119

Exercise in type 2 diabetes: why? Praet et al. Med Sci Sports Exerc 2006; 38: 2037

Exercise in type 2 diabetes: why? Qiu S, et al. PLo. S One. 2014 Oct 17; 9(10): e 109767

Umpierre D, et al. JAMA 2011; 305: 1790 -99 Exercise in type 2 diabetes: why?

Exercise in type 2 diabetes: why? Umpierre D, et al. Diabetologia 2013; 56: 242 -51

Exercise in type 2 diabetes: why? • Long-term exercise training in type 2 diabetes patients also positively affects: – Quality of life – Physical fitness – Inflammatory markers – Cardiovascular disease risk factors • Blood pressure, waist circumference, lipid profile

Exercise in type 1 diabetes: why? Fear of exercise No exercise Increase in fat mass Lowering in endurance capacity Worsening in CVD risk factors Worse glycemic control Further decrease in motivation to exercise Further worsening in fat mass, exercise tolerance, CVD risk factors and glycemic control

Exercise in type 1 diabetes: why?

Exercise physiology in obesity Can be significantly different!

Exercise physiology in obesity § Muscle fibre type composition = Tanner CJ, et al. Am J Physiol 2002; 282: E 1191

Exercise physiology in obesity § Body composition Biolo G, et al. Clin Nutr 2014; 33; 737

Exercise physiology in obesity § Hormonal disturbances Mittendorfer et al. Am J Physiol 2004 Vettor R, et al. Acta Diabetol 1997; 34: 61 Goodpaster B, et al. Obes Res 2002; 10: 575

Exercise physiology in obesity Cedric Moro Adapted from: Hansen D, Exercise therapy in adult individuals with obesity. 2013, Nova Science Publishers, NY, USA

Exercise physiology in obesity § Suppressed lipolysis Mittendorfer B, et al. Am J Physiol 2004; 286: E 354

Exercise physiology in obesity § Cardiovascular disturbances Adapted from: Hansen D, Exercise therapy in adult individuals with obesity. 2013, Nova Science Publishers, NY, USA Gondoni et al. Nutr Metab Cardiovasc Dis 2008

Exercise physiology in obesity § Cardiovascular disturbances Salvadori A, et al. J Clin Basic Cardiol 1999; 2: 229

Exercise physiology in obesity § Cardiovascular disturbances Ardevol A, et al. Eur J Physiol 1998; 435: 495

Exercise physiology in obesity § Ventilatory abnormalities Satiago Lorenzo and Tony Babb Adapted from: Hansen D, Exercise therapy in adult individuals with obesity. 2013, Nova Science Publishers, NY, USA

Exercise physiology in obesity § Ventilatory abnormalities Could lower Pa. O 2 during exercise Satiago Lorenzo and Tony Babb Adapted from: Hansen D, Exercise therapy in adult individuals with obesity. 2013, Nova Science Publishers, NY, USA

Exercise physiology in obesity § Disturbed muscle function § Muscle overload during walking/running § Increased RPE Borg especially during weight -baring exercises

Exercise physiology in obesity § Disturbed muscle function § Lowered fat oxidation capacity Percentage of plasma free fatty acid (FFA) uptake oxidized during basal and exercise (50% maximum O 2 consumption). *Significantly decreased in extremely obese and extremely obese subjects after weight reduction (weight-reduced) compared with lean (P < 0. 05). Houmard J A Am J Physiol Regul Integr Comp Physiol 2008; 294: R 1111 -R 1116

Exercise physiology in obesity § Greater likelihood for development of orthopedic limitations § § § (knee) osteo artritis Plantar heel pain (plantar fasciitis) Carpal tunnel syndrome Rotator cuff tendinitis Low back pain

Exercise physiology in type 2 diabetes Type 2 diabetes patients show different physiological responses to exercise as compared to healthy individuals Type 2 diabetes patients are often overweight/obese, so typical anomalies in exercise response which occur in the obese may be expected

Exercise physiology in type 2 diabetes § Substrate selection is altered
 and during exercise (b) and post-exercise recovery")
Whole-body substrate source utilisation at rest (a) and during exercise (b) and post-exercise recovery (c). Black, plasma NEFA; White, muscle and lipoprotein-derived triacylglycerol; Grey, carbohydrate in a and c, plasma glucose in b; hatching (b), muscle glycogen. *Substrate source oxidation significantly different from control group (p<0. 05) †total fat oxidation significantly different from control group (p<0. 05) Boon et al. Diabetologia 2007; 50: 103 -12

Exercise interventions in type 2 diabetes

Exercise interventions in type 2 diabetes § How to prescribe exercise? § Adapt the exercise modalities! § § § Exercise intensity Session duration Exercise frequency Program duration Addition of strength-training

Exercise intensity Van Loon LJ, et al. J Physiol 2001; 536: 295

Exercise intensity Hansen D, et al. Diabetologia 2008: 52: 1789 -97

Exercise intensity Umpierre D, et al. Diabetologia 2013; 56: 242 -51

Exercise intensity Mitranun W, et al. Scand J Med Sci Sport 2013; e-pub ahead of print

Session duration/volume § Assumption § Longer exercise sessions = greater effect § Greater decrease in plasma glucose levels in T 2 DM patients when cycling for 40 minutes at 70% VO 2 peak compared with 40 minutes at 50% VO 2 peak Sriwijitkamol A, et al. Diabetes 2007; 56: 836 -48

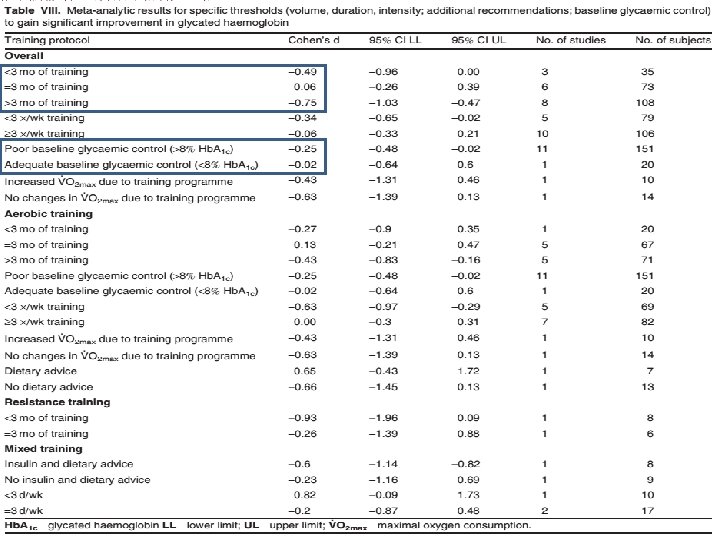
Program duration § International guidelines § Minimal 2 months in order to detect clinical benefits § Elevated physical activity should be sustained after supervised program completion

Program duration Hansen D, et al. Sports Med 2010: 40: 921

Program duration months Hb. A 1 c Cessation of exercise training

Exercise frequency § International guidelines § 3 to 5 d/week § At start of programme: 3 days § After 4 -6 months of exercise training: increase training frequency § On a regular base!

Exercise frequency days Insulin sensitivity

Exercise frequency Umpierre D, et al. Diabetologia 2013; 56: 242 -51

Addition of strength exercises § International guidelines § Strength training exercises should be added: § 10 -15 reps, 3 series, 65 -70% 1 RM

Addition of strength exercises Cauza et al. Arch Phys Med Rehabil 2005; 86: 1527

Addition of strength exercises Cauza et al. Arch Phys Med Rehabil 2005; 86: 1527

Addition of strength exercises Hansen D, et al. Sports Med 2010: 40: 921

Exercise in type 1 diabetes: how?

Exercise in type 1 diabetes: how? Increased synthesis of epinephrine and growth hormone Increased glucose release by liver

How to maximize medical safety Increase the medical safety of intervention in following conditions: • Peripheral neuropathy and/or delayed wound healing = be alert to wounds and/or peripheral sensation disturbances • Autonomic neuropathy = be alert to deregulated blood pressure • Cardiovascular disease = rule out coronary and/or peripheral vascular disease • Retinopathy = no high-intensity exercises • Nephropathy = avoid high blood pressures ACSM & ADA. Med Sci Sports Exerc 2010; 42: 2282 -303

How to maximize medical safety • Orthopedic screening – Diabetic hand syndrome – Dupuytren contracture – Trigger finger – Diffuse idiopathic skeletal hyperostosis – Charcot foot

How to maximize medical safety • Check feet – Shoes: worn out or too narrow? – Feet: dermatologic risk factors

How to maximize medical safety Glycemic control • Start training session • Glucose <75 mg/dl: consume monosaccharides • Glucose <100 mg/dl: be alert for hypoglycemia • Glucose >300 mg/dl: rule out keto-acidosis, no high-intensity exercise • Risk factors for hypoglycemia during exercise • Prolonged (>60 min), and/or intense exercise • Exercise in fasting condition? • Medication: sulfonyloreas, meglitinide, exogeneous insulin therapy • During follow-up • Regularly assess blood glucose content • Always carry monosacharides with you • Exercise in group ACSM & ADA. Med Sci Sports Exerc 2010; 42: 2282 -303

How to maximize medical safety • Check prescribed medication – Cardioprotective drugs • Diuretics – Dehydration and electrolyte imbalances when dosed too high • Beta-blockers – Lowering in exercise HR – Lowers sensation of hypoglycemia • Lipid-lowering medication – Statins could lead to myopathies

How to maximize medical safety Hansen D, et al. Phys Ther 2013; 93: 597 -610

Kine. Coach project Prevalence of T 2 DM is rapidly rising T 2 DM is associated with many co-morbidities Exercise intervention is highly effective GP’s, cardiologists and endocrinologists often promote a healthy lifestyle to their patients • But where can these patients follow medically safe and clinically effective exercise interventions? • •

Kine. Coach project Hansen D, et al. Phys Ther 2013; 93: 597 -610

Kine. Coach project Hansen D, et al. Vlaams Tijdschr Diabetol 2013; 1: 10 -12

Kine. Coach project Hansen D, et al. Phys Ther 2013; 93: 597 -610

Kine. Coach project Hansen D, et al. Phys Ther 2013; 93: 597 -610

Kine. Coach project Hansen D, et al. Phys Ther 2013; 93: 597 -610

Contact: Dominique. hansen@uhasselt. be
- Slides: 73