Exercise stress electrocardiography Physiology and Protocol Indications and


 ↓peripheral resistance ↑SBP, MBP,")
 • Early phase- SV+HR • Late phase-HR")




 also rises in exercise • systolic pressure (SBP) goes up to")
 Blood")










 M/hr Slope 1 0 1. 7 10% 2 3")



 High-risk")




,")











-- 0.")















 Elevation (Q wave lead)")


 of a 12")
 • Abnormal response – J ↑ ≥ 0. 10 m. V(1 mm)")








, should")
, should")



")

 x (0. 1 +")


 prognosis excellent")
, patients with 3 -vessel disease,")
")



 < 12 bpm")


 Stress Test with angina 5%/yr. •")





- Slides: 97
Exercise stress electrocardiography • Physiology and Protocol, • Indications and Contraindications • Frijo Jose A
Exercise physiology • Sympathetic activation • Parasympathetic withdrawal • Vasoconstriction, exept– Exercising muscles – Cerebral circulation – Coronary circulation • ↑norepinephrine and renin
Exercise physiology • • ↑ventri contractility ↑O 2 extraction(upto 3) ↓peripheral resistance ↑SBP, MBP, PP DBP –no significant change Pulm vasc bed can accommodate 6 fold CO CO - ↑ 4 -6 times
Exercise physiology • Isotonic exercise(cardiac output) • Early phase- SV+HR • Late phase-HR
↑ exercise work à ↑ O 2 usage à Person’s max. O 2 consumption (VO 2 max) reached V 02 peak Oxygen consumption (liters/min) Work rate (watts)
• The peak oxygen consumption is influenced by the age, sex, and training level of the person performing the exercise V 02 peak (VO 2 max) Oxygen consumption (liters/min) • The plateau in peak oxygen consumption, reached during exercise rate involving a sufficiently large muscle mass, represents. Work the maximal (watts) oxygen consumption • Maximal oxygen consumption is limited by the ability to deliver O 2 to skeletal muscles and muscle oxidative capacity (mucle mass and mitochondirial enzymes activity).
The ability to deliver O 2 to muscles and muscle’s oxidative capacity limit a person’s VO 2 max. Training à ↑ VO 2 max V 02 peak (trained) 70% V 02 max (trained) V 02 peak (untrained) Oxygen consumption (liters/min) 100% V 02 max (untrained) 175 Work rate (watts)
Respiration during exercise • during dynamic exercise of increasing intensity, ventilation increases linearly over the mild to moderate range, then more rapidly in intense exercise • the workload at which rapid ventilation occures is called the ventilatory breakpoint (together with lactate threshold) Lactate acidifies the blood, driving off CO 2 and increasing ventilatory
Blood Pressure (BP) also rises in exercise • systolic pressure (SBP) goes up to 150 -170 mm Hg during dynamic exercise; diastolic scarcely alters • in isometric (heavy static) exercise, SBP may exceed 250 mm. Hg, and diastolic (DBP) can itself reach 180
Intense exercise à Glycolysis>aerobic metabolism à ↑ blood lactate (other organs use some) Blood lactic acid (m. M) Relative work rate (% V 02 max) Lactate threshold; endurance estimation
Maximum HR • HR=220 - age in years
Post exercise phase • Vagal reactivation • Imp cardiac deceleration mech • ↑in well trained athletes • Blunted in CCF
MET • Metabolic Equivalent Term • 1 MET = "Basal" aerobic oxygen consumption to stay alive = 3. 5 ml O 2 /Kg/min • Differs with thyroid status, post exercise, obesity, disease states
Key MET Values • 1 MET = "Basal" = 3. 5 ml O 2 /Kg/min • 2 METs = 2 mph on level • 4 METs = 4 mph on level • < 5 METs = Poor prognosis if < 65; • 10 METs = same progn with medical thpy as CABG • 13 METs = Excell prognosis, • regardless of othr exercise responses
Key MET Values • 3 -5 METs: • raking leaves, light carpentry, golf, 3 -4 mph • 5 -7 METs: • exterior carpentry, singles tennis • >9 METs: • heavy labour, hand ball, squash, running 6 -7 mph
Estimated Energy Requirements for Various Activities
Estimated Energy Requirements for Various Activities
Calculation of METs on the Treadmill • METs = Speed x [0. 1 + (Grade x 1. 8)] + 3. 5 • Calculated automatically by Device! • • • Note: Speed in meters/minute conversion = MPH x 26. 8 Grade expressed as a fraction
Treadmill protocol • • • Bruce protocol Naughton protocol Weber protocol ACIP(asymptomatic cardiac ischemia pilot) Modified ACIP
The Bruce protocol • Developed in 1949 by Robert A. Bruce, considered the “father of exercise physiology”. • Published as a standardized protocol in 1963. • Remains the gold-standard for detection of myocardial ischemia when risk stratification is necessary.
Protocol description Stage Time (min) M/hr Slope 1 0 1. 7 10% 2 3 2. 5 12% 3 6 3. 4 14% 4 9 4. 2 16% 5 12 5. 0 18% 6 15 5. 5 20%
Calculation of METs on the Treadmill • METs = Speed x [0. 1 + (Grade x 1. 8)] + 3. 5 • Calculated automatically by Device! • • • Note: Speed in meters/minute conversion = MPH x 26. 8 Grade expressed as a fraction
Procedure • Standard 12 lead ECG- leads distally • Torso ECG + BP – Supine and Sitting / standing • HR , BP , ECG – Before, after, stage end – Onset of ischemic response – Each minute recovery(5 -10 mints)
Procedure- Lead systems • Mason-Liker modification – RAD – ↑inf lead voltage – Loss of inf lead q – New Q in AVL
Contraindications to Exercise Testing • • • Absolute Acute MI (< 2 d) High-risk unstable angina Uncontrolled cardiac arrhythmias causing symptoms or hemodynamic compromise Symptomatic severe AS Uncontrolled symptomatic CCF Acute pulmonary embolus or pulmonary infarction Acute myocarditis or pericarditis Acute Ao dissection
Contraindications to Exercise Testing • • Relative LMCA stenosis Moderate stenotic valvular heart disease Electrolyte abnormalities Severe HTN Tachyarrhythmias or bradyarrhythmias HOCM and other forms of outflow tract obstruction Mental or physical impairment leading to inability to exercise adequately • High-degree AV block
• Both MI and deaths have been reported and can be expected to occur at a rate of up to 1 per 2500 tests
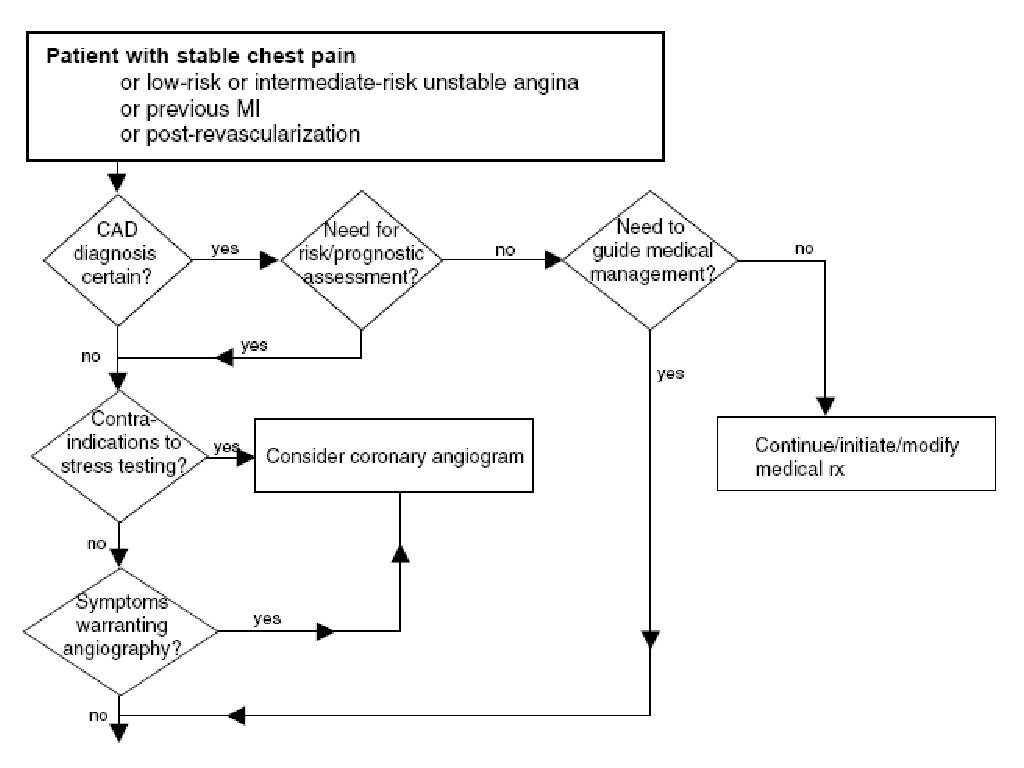
Bayes' theorem A theory of probability ‘The post test probability is proportional to the pretest probability’
Classification of chest pain • Typical angina 1. Substernal chest discomfort with characterstic quality and duration 2. Provoked by exertion or emotional stress 3. Relieved by rest or NTG • Atypical angina Meets 2 of the above characteristics • Noncardiac chest pain Meets one or none of the typical characteristics
Pretest Probability • Based on the patient's history ( age, gender, chest pain ), physical examination and initial testing, and the clinician's experience. • Typical or definite angina →pretest probability high - test result does not dramatically change the probability. • Diagnostic testing is most valuable in intermediate pretest probability category
Pre Test Probability of Coronary Disease by Symptoms, Gender and Age
Pre-test Probability of CAD by Age, Gender, and Symptoms • Typical/Definite Angina Pectoris • Age 30 -39 – Men – Women Intermediate (10 -90%) Intermediate • Age 40 -49 – Men – Women High (>90%) Intermediate • Age 50 -59 – Men – Women High Intermediate • Age 60 -69 – Men – Women High
Pre-test Probability of CAD by Age, Gender, and Symptoms • Atypical/Possible Angina Pectoris: • Age 30 -39 – Men – Women Intermediate Very Low (<5%) • Age 40 -49 – Men – Women Intermediate Low (<10%) • Age 50 -50 – Men – Women Intermediate • Age 60 -69 – Men – Women Intermediate
Pre-test Probability of CAD by Age, Gender, and Symptoms • Nonanginal Chest Pain: – Age 30 -39 • Men Low • Women Very Low – Age 40 -49 • Men Intermediate • Women Very Low – Age 50 -59 • Men Intermediate • Women Low – Age 60 -69 • Men Intermediate • Women Intermediate •
Pre-test Probability of CAD by Age, Gender, and Symptoms • Asymptomatic: – Age 30 -39 • Men Very Low • Women Very Low – Age 40 -49 • Men • Women Low Very Low – Age 50 -59 • Men • Women Low Very Low – Age 60 -69 • Men • Women Low
EXERCISE TESTING TO DIAGNOSE OBSTRUCTIVE CAD • Class I • Adult patients (including RBBB or <1 mm of resting ST↓) with intermediate pretest probability of CAD • Class IIa • Patients with vasospastic angina.
EXERCISE TESTING TO DIAGNOSE OBSTRUCTIVE CAD • Class IIb • 1. Patients with a high pretest probability of CAD • 2. Patients with a low pretest probability of CAD • 3. Patients with <1 mm of baseline ST ↓and on digoxin. • 4. Patients with LVH and <1 mm baseline ST ↓. • Class III 1. Patients with the following baseline ECG abnormalities: • • Pre-excitation syndrome • • Electronically paced ventricular rhythm • • >1 mm of resting ST depression • • Complete LBBB
Exercise Testing in Asymptomatic Persons Without Known CAD • Class I • None. • Class IIa • Evaluation of asymptomatic T 2 DM pts who plan to start vigorous exercise ( C) • Class IIb • 1. Evaluation of pts with multiple risk factors as a guide to riskreduction therapy. • 2. Evaluation of asymptomatic men > 45 yrs and women >55 yrs: • • Plan to start vigorous exercise • • Involved in occupations which impact public safety • • High risk for CAD(e. g. , PVOD and CRF) • Class III • Routine screening of asymptomatic
RISK ASSESSMENT AND PROGNOSIS IN PATIENTS WITH SYMPTOMS OR A PRIOR HISTORY OF CAD • Class I • 1. Initial evaluation with susp/known CAD, including. RBBB or <1 mm of resting ST Depression • 2. Susp/ known CAD, previously evaluated, now significant change in clinical status. • 3. Low-risk UA pts >8 to 12 hrs & free of active ischemia/CCF • 4. Intermed-risk UApts > 2 to 3 days & no active ischemia/ CCF • Class IIa • Intermed-risk UA pts – initial markers (N), rpt ECG –no signi change, and markers >6 -12 hrs (N) & no other evidence of ischemia during observation.
AFTER MYOCARDIAL INFARCTION • Class I • 1. Before discharge (submaximal --4 to 6 days). • 2. Early after discharge if the predischarge exercise test was not done (symptom limited -14 to 21 days). • 3. Late after discharge if the early exercise test was submaximal (symptom limited --3 to 6 weeks). • Class IIa • After discharge as part of cardiac rehabilitation in patients who have undergone coronary revascularization.
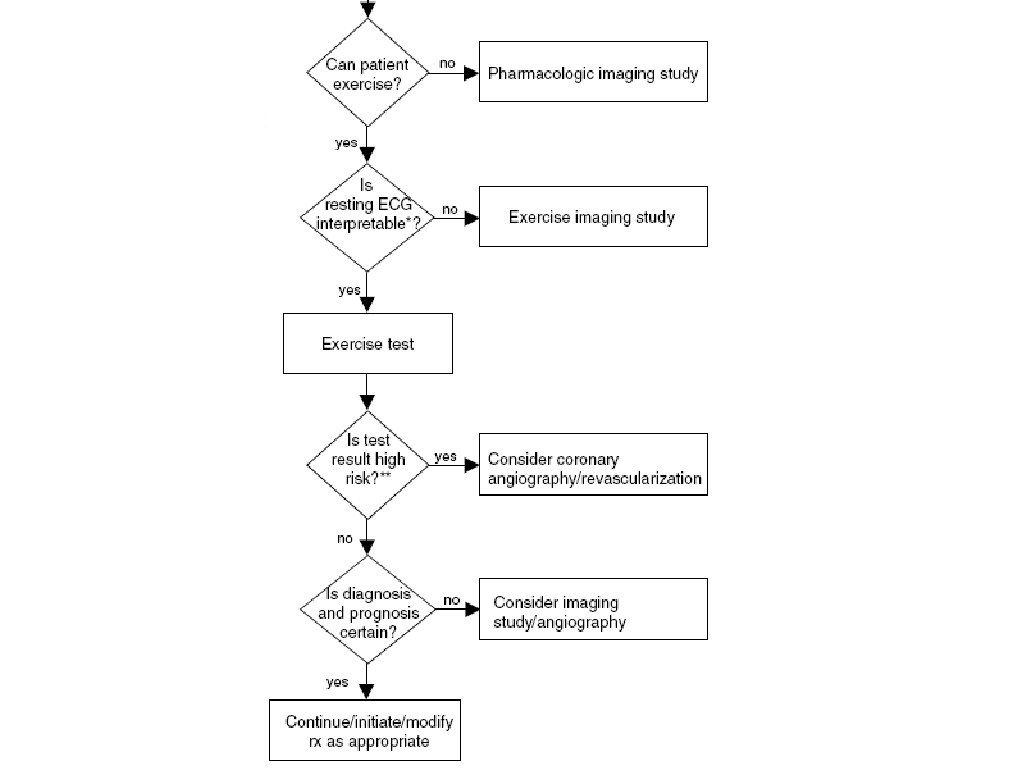
• Submaximal protocols • predetermined end point, often a peak HR 120 bpm, or 70% predicted max HR or peak MET - 5 • Symptom-limited tests • to continue till signs or symptoms necessitating termination (i. e. , angina, fatigue, ≥ 2 mm of ST↓, ventricular arrhythmias, or ≥ 10 -mm Hg drop in SBP from the resting blood pressure)
• The incidence of fatal cardiac events(inclu fatal MI & cardiac rupture)-- 0. 03% • Nonfatal MI and successfully resuscitated cardiac arrest -- 0. 09% • Complex arrhythmias, including VT --1. 4%. • Symptom-limited protocols have an event rate that is 1. 9 times that of submaximal tests
AFTER MYOCARDIAL INFARCTION • Class IIb • 1. Patients with the following ECG abnormalities: • • Complete LBBB • • Pre-excitation syndrome • • LVH • • Digoxin therapy • • >1 mm of resting ST-segment depression • • Electronically paced ventricular rhythm • 2. Periodic monitoring in patients who continue to participate in exercise training or cardiac rehabilitation. • Class III • 1. Severe comorbidity likely to limit life expectancy and/or candidacy for revascularization. • 2. At any time to evaluate pts with AMI with uncompensated CCF, arrhythmia, or noncardiac exercise limiting conditions. • 3. Before discharge to evaluate pts who have already been selected for, or have undergone, cardiac cath. • Although a stress test may be useful before or after cath to evaluate or identify ischemia in the distribution of a coronary lesion of borderline severity, stress imaging tests are recommended.
Clinical indications of high risk at pre-discharge Strategy 3
Clinical indications of high risk at pre-discharge Cardiac cath
Exercise Testing Before and After Revascularization • Class I • 1. Demonstration of ischemia before revascularization. • 2. Evaluating recurrent symps suggesting ischemia aft revascularization. • Class IIa • Aft discharge for activity counseling and/or exercise training as part of rehabilitation in pts aft revascularization. • Class IIb • 1. Detection of restenosis in selected, high-risk asymptomatic pts < first 12 months aft PCI. • 2. Periodic monitoring of selected, high-risk asymptomatic ps for restenosis, graft occlusion, incomplete coronary revascularization, or disease progression. • Class III • 1. Localization of ischemia for determining the site of intervention. • 2. Routine, periodic monitoring of asymptomatic pts after PCI or CABG without specific indications.
Stress Testing Modality Exercise test Sensitivity Specificity 68% 77% Nuclear Imaging 87 -92% 80 -85% Stress Echo 80 -85% 88 -95%
Investigation of Heart Rhythm Disorders • Class I • 1. Identification of appropriate settings in pts with rate-adaptive pacemakers. • 2. Evaluation of cong CHB in pts considering ↑activity/competitive sports. (C) • Class IIa • 1. Evaluating known or suspected exerciseinduced arrhythmias. • 2. Evaluation of medical, surgical, or ablative therapy in exercise-induced arrhythmias
Investigation of Heart Rhythm Disorders • Class IIb • 1. Isolated VPC in middle-aged pts without other evidence of CAD. • 2. Prolonged 1˚AV block or type I-2˚AV block , LBBB, RBBB, or VPC in young pts considering competitive sports. (C) • Class III • Routine investigation of isolated VPC in young pts.
• Interpreting TMT
Normal ECG changes during exercise • • ↓ PR, QRS, QT ↑ P amplitude Progressive downsloping PR in inf leads j point depression
The Exercise ECG 1 = Iso-electric 2 = J point 3 = J + 80 msec
Criteria for Reading ST-Segment Changes on the Exercise ECG • ST DEPRESSION: • Measurements made on 3 consecutive ECG complexes • ST level is measured relative to the P-Q junction • When J-point is depressed relative to P-Q junction at baseline: –Net difference from the J junction determines the amount of deviation • When the J-point is elevated relative to P-Q junction at baseline and becomes depressed with exercise: –Magnitude of ST depression is determined from the P-Q junction and not the resting J point
Upsloping J point depression of 2 to 3 mm in leads V 4 to V 6 with rapid upsloping ST segments depressed approximately 1 mm 80 msec after the J point. The ST segment slope in leads V 4 and V 5 is 3. 0 m. V/sec. This response should not be considered abnormal.
• ST 60 -- HR > 130/min • ST 80 -- HR ≤ 130/min
Criteria for Abnormal and Borderline STSegment Depression on the Exercise ECG • ABNORMAL: – 1. 0 mm or greater horizontal or downsloping ST depression at 80 msec after J point on 3 consecutive ECG complexes • BORDERLINE: – 0. 5 to 1. 0 mm horizontal or downsloping ST depression at 80 msec after J point on 3 consecutive ECG complexes – 2. 0 mm or greater upsloping ST depression at 80 msec after J point on 3 consecutive ECG complexes
Normal Rapid Upsloping Minor ST Depression Slow Upsloping
Horizontal Downsloping Elevation (non Q lead) Elevation (Q wave lead)
• In lead V 4 , the exercise ECG result is abnormal early in the test, reaching 0. 3 m. V (3 mm) of horizontal ST segment depression at the end of exercise. • Consistent with a severe ischemic response.
• The J point at peak exertion is depressed 2. 5 mm, the ST segment slope is 1. 5 m. V/sec, and the ST segment level at 80 msec after the J point is depressed 1. 6 mm. • This “slow upsloping” ST segment at peak exercise indicates an ischemic pattern in patients with a high coronary disease prevalence pretest. • A typical ischemic pattern is seen at 3 minutes of the recovery phase when the ST segment is horizontal and 5 minutes after exertion when the ST segment is downsloping.
• Becomes abnormal at 9: 30 minutes (horizontal arrow right) of a 12 -minute exercise test and resolves in the immediate recovery phase. • This ECG pattern in which the ST segment becomes abnormal only at high exercise workloads and returns to baseline in the immediate recovery phase may indicate a false -positive result in an asymptomatic individual without atherosclerotic risk factors.
ST Elevation(localising) • Abnormal response – J ↑ ≥ 0. 10 m. V(1 mm) – ST 60 ≥ 0. 10 m. V(1 mm) – Three consecutive beats • Q wave lead (Past MI) • Severe RWMA, ↓EF, ↓Prognosis • Non Q wave lead (Past MI) • Severe ischemic response • Non Q wave lead (No past MI)-1% • Transmural reversible myocardial ischemia----vasospasm, ↑coronary narrowing
• A 48 -year-old man with several atherosclerotic risk factors and a normal rest ECG result developed marked ST segment elevation (4 mm [arrows]) in leads V 2 and V 3 with lesser degrees of ST segment elevation in leads V 1 and V 4 and J point depression with upsloping ST segments in lead II, associated with angina. • This type of ECG pattern is usually associated with a full-thickness, reversible myocardial perfusion defect in the corresponding left ventricular myocardial segments and high-grade intraluminal narrowing at coronary angiography. Rarely, coronary vasospasm produces this result in the absence of significant intraluminal atherosclerotic narrowing. (
ECG Patterns Indicative of Myocardial Ischaemia ECG Patterns Not Indicative of Myocardial Ischaemia
ECG changes during stress test
ST Heart Rate Slope • Maximal change in ST with heart rate calculated at the end of each stage • Heart rate adjustment of ST segment depression - improve the sensitivity • Calculation of the maximal ST/heart rate slope in m. V/beats/min - linear regression • An ST/heart rate slope • >2. 4 m. V/beats/min - abnormal • >6 m. V/beats/min - three-vessel CAD.
The ST/heart rate index • Average change of ST segment depression with heart rate throughout the course of the exercise test. • >1. 6 - abnormal
Confounders of Exercise Treadmill Test Interpretation • Digoxin – Produces an abnormal ST-segment response to exercise. This abnormal ST depression occurs in 25% to 40% of healthy subjects studied and is directly related to age. • Left Ventricular Hypertrophy – Decreased specificity of exercise testing, but sensitivity is unaffected. Therefore, a standard exercise test may still be the first test, with referrals for additional tests only indicated in patients with an abnormal test result. • Resting ST Depression – Resting ST-segment depression has been identified as a marker for adverse cardiac events in patients with and without known CAD. • Left Bundle-Branch Block – Exercise-induced ST depression usually occurs with left bundle-branch block and has no association with ischemia. Even up to 1 cm of ST depression can occur in healthy normal subjects. There is no level of ST-segment depression that confers diagnostic significance in left bundle-branch block. • Right Bundle-Branch Block – The presence of right bundle-branch block does not appear to reduce the sensitivity, specificity, or predictive value of the stress ECG for the diagnosis of ischemia. • Beta Blocker Therapy – For routine exercise testing, it appears unnecessary for physicians to accept the risk of stopping beta-blockers before testing when a patient exhibits possible symptoms of ischemia or has hypertension. However, exercise testing in patients taking betablockers may have reduced diagnostic or prognostic value because of inadequate heart rate response.
Early repolarization and resting ST↑ • Return to the PQ junction is normal • Hence ST↓ determined from PQ junction • Not from the elevated J point before exercise
Duke Treadmill Score • Treadmill Score=Exercise time • -5 X (amount of ST-seg. deviation in mm) - 4 X exercise angina index • (0 -no angina, 1 angina, 2 if angina stops test). • High Risk= -11, mortality >5% annually. • Low Risk= +5, mortality 0. 5% annually. • Ann Intern Med 1987; 106: 793.
ACC/AHA Guidelines: • “Patients with a high-risk exercise test result (mortality ≥ 4%/yr), should be referred for cardiac catheterization. ”
ACC/AHA Guidelines: • “Pts. with an intermediate-risk result (mortality of 2% to 3%/yr), should be referred for additional testing, either cardiac catheterization, or an exercise imaging study. ”
Pseudo normalization pattern • No prior MI • Nondiagnostic finding • Prior MI • Suggests Reversible myocardial ischemia • Needs substantiation by rev myo perfusion defect
R Wave amplitude • LVH Voltage criteria • ST seg – less reliable to ∆ CAD even in the absence of LV strain pattern • Loss of R wave (MI) • ↓Sensitivity of ST response in that lead
U inversion • Occasionally in precordial leads at HR<120 • Relatively nonsensitive • Relatively specific
Abnormal BP Response • Failure to ↑SBP >120 mm. Hg • Sustained ↓(15 secs) >10 mm. Hg • ↓SBP below resting BP during progressive exe • Inadequate ↑ of CO • 3 VD, LMCA-d, cardiomyopathy, arrhythmias, • vasovagal, LVOTobs, hypovolemia, • prolonged vigorous exe • Normal responses: – Increase in SBP (> 20 -30 mm. Hg) – No change or fall in DBP
Maximum work capacity • Important prognostic measurement • Work performed in METs • Not the no: of minutes of exercise
Exercise Capacity • VO max = (mph x 26. 8) x (0. 1 + [% grade X 1. 8] + 3. 5 2 • 1 MET (metabolic equivalent) = 3. 5 ml 02 /kg/min • Stage 1 = 5 METS • Stage 2 = 6 - 8 METS • Stage 3 = 8 -10 METS
Exercise Capacity “The strongest predictor of the risk of death among both normal subjects, and those with cardiovascular disease”. “Each 1 -MET increase in exercise capacity conferred a 12% improvement in survival”. NEJM 2002; 346: 793 -801.
For each 1 -MET increase in exercise capacity, the survival improved by 12 percent N Engl J Med 2002
Exercise Capacity • In pts. with CAD > 13 METS (Stage IV) prognosis excellent regardless of whether medical or surgical therapy is selected. * • Documented CAD, ≥ 2 mm ST-segment depression. Stage IV had a 100% 5 -year survival rate. ** • *Circ 1984; 70: 226. • **Circ 1982; 65: 482.
Exercise Capacity In the Coronary Artery Surgery Study (CASS), patients with 3 -vessel disease, and high exercise capacity (≥ 10 METS), showed no benefit from surgery. JACC 1986; 8: 741 -748.
Heart rate response • Inappropriate ↑ at low work load • Anxiety (<1 minute-transient) • Persisting several minutes • AF, physically deconditioned, hypovolemic, • anemic, marginal LV function
Heart rate response • Chronotropic incompetence • Inability to attain THR OR • Abnormal HR Reserve(<80%) • {%HR Reserve=(HRpeak-HRrest)/(220 -age. HRrest)} • Autonomic dysfunction, SN dysfuntion, • drugs, myocardial ischemia • ↑long term mortality (not on β blockers)
Chronotropic Incompetence Circ 1996; 93: 1520. Framingham Heart
Heart Rate Recovery • During exercise, HR increases due to withdrawal of vagal tone, and increase of sympathetic tone. • During recovery, there is a rapid reactivation of vagal tone leading to a decrease in heart rate.
Heart Rate Recovery • Abnormal: • 1 minute • TMT (upright) < 12 bpm • TMT (supine) < 18 bpm • An upright value <22 bpm at 2 minutes is abnormal • Poor prognosis independent of other factors •
Heart Rate Recovery After Exercise Testing Predicts Outcome in CAD
Exercise induced Chest discomfort • • • Usually after ischemic ST changes May be associated with DBP In some, only chest discomfort In CSA, CP less freq than ST↓ Angina with no ST ↓- MPI useful to assess ischemic severity.
Angina during Stress Test • Mortality • (+) Stress Test with angina 5%/yr. • (+) Stress Test, no angina Circ 1984; 70: 547551. 2. 5%/yr.
Markedly Positive Stress Test 1. ECG changes in the first three minutes. 2. ECG changes that last through recovery. 3. Hypotensive response.
Adverse prognosis & multivessel CAD • Symptom limiting exercise < 5 METs • Abnormal BP response • ST↓≥ 2 mm or downsloping ST↓ • <5 METs, ≥ 5 leads, persisting ≥ 5 mins into reco • ST↑ • Angina at low exercise work loads • Reproducible sustained/symptomatic VT
Indications for Terminating Exercise Testing • Absolute indications • Drop in systolic BP >10 mm Hg from baseline when accompanied by other evidence of ischemia • Moderate to severe angina • ↑ CNS sympts (ataxia, dizziness, or near-syncope) • Signs of poor perfusion (cyanosis or pallor) • Technical difficulties in monitoring ECG or systolic BP • Subject’s desire to stop • Sustained VT • ST ↑ (≥ 1. 0 mm) in leads without Q-waves (other than V 1 or a. VR)
Indications for Terminating Exercise Testing • Relative indications • ↓ in systolic BP (≥ 10 mm Hg) in the absence of other evidence of ischemia • ST or QRS changes such as excessive ST↓ (>2 mm of horizontal or downsloping ST↓ ) or marked axis shift • Arrhythmias other than sustained VT, including multifocal PVCs, triplets of PVCs, SVT, heart block, or bradyarrhythmias • Fatigue, shortness of breath, wheezing, leg cramps, or claudication • Development of BBB or IVCD that cannot be distinguished from VT • Increasing chest pain • Hypertensive response
THANK YOU