Exercise Induced Paradoxical Vocal Cord Dysfunction EIPVCD Dale
 Dale R. Gregore M. S. , CCC-SLP")
 ABduct allowing air to flow")




 The cord function is reversed in that the vocal")

 – Most common term Munchausen’s Stridor Emotional Laryngeal Wheezing")


 during respiration instead of abducting (opening) Laryngeal instability")

 – Food/ liquid/ acid refluxes from the stomach up")




 Asthma-associated laryngeal dysfunction Brainstem dysfunction CVA or injury Chronic laryngeal instability,")









 NORMAL VCD")

 – How soon after exercise starts do your symptoms begin? –")
 – Do symptoms ever occur during sleep? – Do you routinely")






 Asthma Exercise, extreme temperatures, airway temperatures, irritants, emotional airway")






 Resistance and focus on")













. Vocal cord dysfunction. Medical/Scientific Update.")


- Slides: 63
Exercise Induced Paradoxical Vocal Cord Dysfunction (EI-PVCD) Dale R. Gregore M. S. , CCC-SLP Speech Language Pathologist Clinical Rehabilitation Specialist - Voice
NORMAL Respiration 101 On inhalation, the vocal cords (folds) ABduct allowing air to flow into the trachea, bronchial tubes, lungs On exhalation, the vocal folds may close slightly, however should and do remain ABducted
Normal Larynx
Vocal fold ABDUCTION occurs during respiration
Vocal fold ADDUCTION Occurs during swallowing, coughing, etc…
Strobe exam
Paradoxical Vocal Fold Movement (PVFM) The cord function is reversed in that the vocal folds ADDuct on inspiration versus ABduct Leads to tightness or spasm in the larynx Inspiratory wheeze evident
Definition of EI-VCD “Inappropriate closure of the vocal folds upon inspiration resulting in stridor, dyspnea and shortness of breath (SOB) during strenuous activity” – Matthers-Schmidt, 2001; Sandage et al, 2004
Pseudonyms Vocal Cord Dysfunction (VCD) – Most common term Munchausen’s Stridor Emotional Laryngeal Wheezing Pseudo-asthma Fictitious Asthma Episodic Laryngeal Dyskinesia
Patient description of VCD episodes – “in the top of my throat I see a Mc. Donalds straw surrounded by darkness. The straw ends in a pool of thick, sticky liquid that is encased by a wall of rubber bands and outside of the rubber bands is air that I can’t access”. – “The top part of my throat is complete darkness, at the back part of the darkness there are cotton balls. These are holding my fear”.
PVFM Visualized Anterior portion of the vocal folds are ADDucted Only a small area of opening at the Posterior aspect of the vocal folds Diamond shaped ‘CHINK’ May be evident on both inhalation and exhalation
Essential Features Vocal fold adduct (close) during respiration instead of abducting (opening) Laryngeal instability while patient is asymptomatic – Treole, K. et. al. 1999 Episodic respiratory distress
Symptoms Stridor Difficulty with inspiratory phase Throat tightening > bronchial/ chest Dysphonia during/following an attack Abrupt onset and resolution Little or NO response to medical treatment (inhalers, bronchodilators)
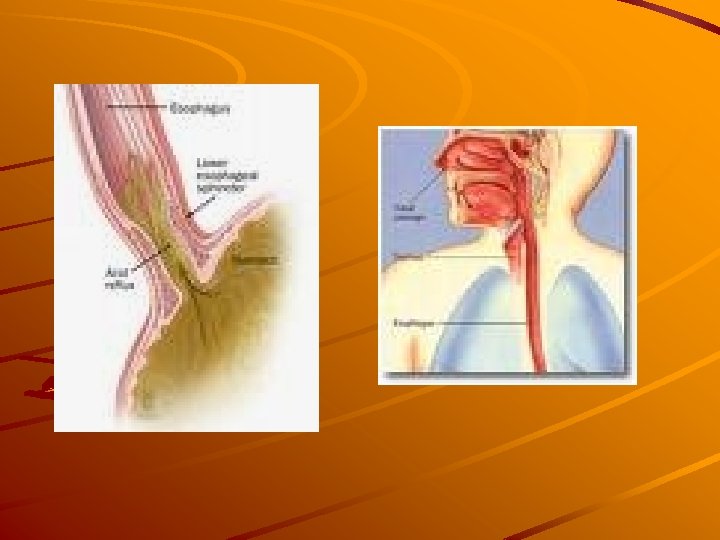
Various Etiologies Laryngo-Pharyngeal Reflux (LPR) – Food/ liquid/ acid refluxes from the stomach up the esophagus into the pharynx (throat) – Can spill over and into the larynx – causes coughing, choking, breathing and voice changes, swelling, irritation, – Can be SILENT or sensed when it happens – WATERBRASH
LPR, continued Clinical characteristics can be observed using videolaryngoscopic or stroboscopic visualization of the larynx Ideally, diagnosed by a 24 hour p. H. Probe or EGD
LPR and Athletes Well documented occurrence in weight lifting Can be aggravated by bending, pushing/ resisting (tackling, etc…), tight clothing, even drinking water during a game/ meet/ match Timing of meals before exercise is important Type of foods/ liquids should be monitored
Laryngopharyngeal Reflux: Clinical Signs Interarytenoid Edema Lx Erythema Vocal Fold Edema
Other potential causes of Paradoxical Vocal Cord Dysfunction Allergic rhinitis or reaction Conversion disorder Anxiety Respiratory-type or druginduced laryngeal dystonia
Etiologies (cont. ) Asthma-associated laryngeal dysfunction Brainstem dysfunction CVA or injury Chronic laryngeal instability, sensitivity & tension
Athlete Profile for EI-VCD Onset between 11 -18 Females have a greater incidence (generally 3: 1) High achieving “Type A” personalities High personal standards and/or social pressures Intolerant to personal failure
Athlete Profile, cont… Competitive Self demanding Perceives family pressure to achieve a high level of success “Choke” under pressure May have recently graduated to higher level of competition within their sport (JV to Varsity: Rep to Travel team; college level sports, etc)
EI-VCD versus Asthma Recalcitrant to asthma medications i. e. does not respond to Individuals with “asthma” after long term steroid use might not truly have asthma, but VCD Individuals with significant anxiety: is it LIVE OR MEMOREX? Which causes which?
Differential Diagnosis of EI-VCD Includes a detailed Case History Pulmonary function Studies Lab Test ENT/ Pulmonary/ Allergy evaluations Flexible Laryngoscopy/ videostroboscopy Speech-language pathology evaluation Supplemental as needed: Psychological evaluation
Differential Diagnosis of VCD Team Must Rule Out: – Mass Obstruction – Bilateral vocal fold paralysis – Anaphylactic laryngeal edema – Extrinsic airway compression – Foreign body aspiration – Infectious croup – Laryngomalacia – Exercise Induced Asthma/ Asthma
Diagnosis of EI-VCD Often mistaken for asthma Diagnosis of EI-PVCD is by exclusion = when patient fails to respond to asthma or allergy medication, then VCD is finally considered
EI-VCD and Asthma Can exist independently Can also coexist – Patient may experience LPR which causes Asthma flare-up and then laryngospasm (VCD) from coughing – May experience chest (asthma) and/or laryngeal (VCD) tightness
EI-PVCD versus Exercise Induced Asthma
Typical Spirometry Findings for PVCD Asymptomatic – Flow-volume loops are normal Symptomatic: – Blunted inspiratory curve – Inspiratory curves highly varied – Expiratory portion may be blunted – Ratio of forced expiratory to inspiratory flow at 50% VC can be greater than 1. 0
Inspiratory cut-off, flattening of the inspiratory limb (curve) NORMAL VCD
Case History Questions – Do you have more trouble breathing in than out? – Do you experience throat tightness? – Do you have a sensation of choking or suffocation? – Do you have hoarseness? – Do you make a breathing-in noise (stridor) when you are having symptoms?
Questions (cont. ) – How soon after exercise starts do your symptoms begin? – How quickly do symptoms subside? – Do symptoms recur to the same degree when you resume exercise? – Do inhaled bronchodilators prevent or abort attacks? – Do you experience numbness and/or tingling in your hands or feet or around your mouth with attacks
Questions (cont. ) – Do symptoms ever occur during sleep? – Do you routinely experience nasal symptoms (postnasal drip, nasal congestion, runny nose, sneezing)? – Do you experience reflux symptoms?
Videostroboscopic Examination Instrumentation – Flexible fiberoptic laryngeal endoscope with stroboscopic capability Observations – Movement of arytenoids during respiration at rest: Complete closure; Posterior diamond – Signs of laryngopharyngeal reflux disorder (LPR) – Degree of laryngeal instability
Laryngeal Supraglottic Hyperfunction arytenoid compression ventricular compression Limited airway for phonation
VCD appearance on direct examination Laryngeal Supraglottic Hyperfunction Abnormal ventricular compression during speech
Laryngeal Supraglottic Hyperfunction Sphincteric contraction of the supraglottis during speech production
PVCM Visualized Posterior ‘chink’ Rounded arytenoids, but normal abduction
Diagnostic Features PVFM Asthma Flow-volume loop Inspiratory cut-off, Reduced expiratory perhaps some expiratory limb only limb reduction * Bronchial provocation test Negative Laryngoscopic observations Inspiratory adduction of anterior 2/3 of vocal folds; posterior diamondshaped chink; perhaps medialization of ventricular folds; inspiratory adduction may carry over to expiration Positive Vocal folds may adduct during exhalation
Diagnostic Features PVFM Precipitators (triggers) Asthma Exercise, extreme temperatures, airway temperatures, irritants, emotional airway irritants, stressors emotional stressors, allergens Number of triggers Usually one Usually multiple Breathing obstruction location Laryngeal area Chest area Timing of breathing noises Stridor on inspiration Wheezing on exhalation
Pattern of dyspneic event Sudden onset and relatively rapid cessation Nocturnal awakening with symptoms Rarely Response to bronchodilators and/or systemic corticosteroids No response More gradual onset longer recovery period Almost always Good response
Acute Management of EI-VCD in the field Approach to the patient is important It is generally agreed that patients do not consciously manipulate or control their upper airway obstruction
Acute Management of EI-VCD During an episode, they usually feel helpless and terrified Implying that it is “in their head” is incorrect and counterproductive to their recovery Coach them through, help them out Be positive
Acute Management of Attacks – Offer reassurance and empathy – Eliminate activity and people from environment – Prompt for EASY BREATHING – Elicit controlled ‘Panting’ Relaxed jaw Tongue on floor of mouth behind bottom teeth
Acute Management in the Game Visualize WIDE OPEN AIRWAY 6 lane highway with no roadblocks Air goes in and circles around, goes out Shoulders relaxed Standing w/ open chest, hands on hips, or bent over/ hands on knees…. which position works best?
Quick Sniff Technique – Sniff then Blow…. talk the athlete through this – Sniff in with focal emphasis at the tip of the nose Sniff = ABduction – Then exhale with pursed lips on “ssssss” “shhhhhh” “ffff” “whhhh” = Back pressure respiration
ACUTE treatment, cont… – Breathing against pressure (hand on abdomen) Resistance and focus on pressure against / in another body part – Heliox Administered by Paramedics or ER MDs – Sedatives and psychotropic medications Last resort Calming effect Eliminates tension/ constriction
Treatment: Speech Therapy Patient counseling, education Respiratory retraining Focal and whole body relaxation Phonatory retraining Monitor reflux Sx or anxiety Develop / outline a ‘Game Plan’ = practice when asymptomatic; implement at the onset of sx
Therapeutic goals and methods Goal – Ability to overcome fear and helplessness – Reduced tension in- extrinsic laryngeal muscles – Diversion of attention from larynx Method – Mastery of breathing techniques – Open throat breathing; resonant voice technique – Diaphragmatic breathing and active exhalation
Therapeutic goals and methods Goal – Reduced tension in neck, shoulders and chest – Ability to use techniques to reduce severity and frequency of attacks Method – Movement, stretching, progressive relaxation – Increase awareness of early warning symptoms; Rehearse action plan
Speech Therapy Patient Counseling & Education – Description of laryngeal events – Viewing of laryngoscopy tape – Relate parallels to other stress induced disorders: migraine, irritable colon, muscle tension dysphonia, GEReflux – Flexible endoscopic biofeedback – Sensory biofeedback (s. EMG)
Speech Therapy Respiratory training – Low “diaphragmatic” breathing versus “high” clavicular thoracic – Rhythmic respiratory cycles – Use resistance exhale (draw attention away from larynx and extend exhale) – Prevention and coping strategies during episodes = Action Plan
Back Pressure Breathing Nasal Sniff = OPEN cords Prolonged exhalation /w/, /f/, /sh/, /s/ Shoulders relaxed Throat open Implement when laying, sitting, standing, walking, jogging, running, playing sports, etc
Relaxation Training Goal – Teach the patient to relax focal areas then the entire body during an episode of respiratory distress Methods – Use progressive relaxation with guided imagery – Explore the patient’s visual concept of their disorder and alter
ST Duration: The CCHS Approach 2 -8 sessions Average 4 sessions Followed by clinical observation during sport/ game Followup phone / email contact: tell me how it is going? Re-evaluation as necessary, if symptoms reoccur (rarely)
CASE DISCUSSION 14 year old female Sports: field hockey, soccer Travel soccer U-17 team/ midfiled Initial symptoms: ‘throat closes’ ~5 minutes in to game; hand on throat; signals coach; pulled from game; 20 minute recovery: lying on sideline
Therapy Focus and Outcome 5 sessions Breathing 101 Training from static to active movement/ running Full coaching then observation of strategy implemetation in therapy and during game Outcome: (-) sx during mile run; cool down routine implemented; 20 -30 minute game play/ no EI-VCD w/ ‘game plan’
Case Discussion #2 14 year old female Sports: cross country; basketball Initial Symptoms: ‘throat closed’ during CC trials; had to ‘drop out’ Secondary Symptoms: inspiratory stridor when wearing mouth guard/ basketball; felt ‘faint’
Therapy Focus and Outcome 5 sessions Goals: establish ‘low’ AD breathing/ eliminate shoulder elevation and CT respiration pattern; train in back pressure breathing w/ and w/out mouthguard during activities of progressive effort including walk; jog; stairs, treadmill; suicide drills; BB drills; sprints, etc
Outcome Successful resolution of PVFM during 20 minute runs and when playing BB Increased awareness of AD versus CT respiration Habituated alternate use of sniff/ pant – blow, etc. Increased perceived ‘control’ over breathing and performance Spring Sport pending: soccer
REFERENCES Brugman, S. M. , & Newman, K. (1993). Vocal cord dysfunction. Medical/Scientific Update. 11. 5. 1 -5. Christopher, K. L. , Wood. II, R. P. , Eckert, R. C. , Blager, F. B. , Raney, R. A. , & Souhrada, J. F. (1983). Vocalcord dysfunction presenting as asthma. The New England Journal of Medicine. 308. 1556 -1570. Gavin, L. A. , Wamboldt, M. , Brugman, S. , Roesler, T. A. , & Wamboldt, F. (1998). Psychological and family characteristics of adolescents with vocal cord dysfunction. Journal of Asthma. 35. 409 -417. Martin, R. J. , Blager, F. B. , Gay, M. L. , & Wood. II, R. P. (1987). Paradoxic vocal cord motion in presumed asthmatics. Seminars in Respiratory Medicine. 8. 332 -337.
Matthers-Schmidt B. A Paradoxical Vocal Fold Motion: A Tutorial on a Complex Disorder and the Speech Language Pathologist’s Role. American Journal of Speech-Language Pathology 2001; 10: 111 -25. Sandage et. al. Paradoxical vocal fold motion in children and adolescents. Lang. Speech Hear. Serv. Sch. 2004: 35 (4) 353 -62 Vlahakis NE, Patel AM, Maragos NE, Beck KC. Diagnosis of Vocal Cord Dysfunction: The Utility of Spirometry and Plethysmography. Chest 2002; 122: 22462249. Nastasi, K. J. , Howard, D. A. , Raby, R. B. , Lew, D. B. , & Blaiss, M. S. (1997). Airway fluoroscopic diagnosis of vocal cord dysfunction syndrome. Annals of Allergy, Asthma, Immunology. 78. 586 -588.
Powell DM, Karanfilov BI, Beechler KB, Treole K, Trudeau MD, Forrest L. Paradoxical vocal cord dysfunction in Juveniles. Arch. Otolaryngol Head Neck Surg. 2000 Jan; 126 (1): 29 -34 Morris MJ, Deal LE, Bean DR, Grbach VX, Morgan JA. Vocal Cord Dysfunction in Patients with Exertional Dyspnea. Chest 1999; 116: 1676 -1682.