EXAMINATION OF ULCER BY Dr Abdelrahman Khairy Assistant

EXAMINATION OF ULCER BY Dr. Abdelrahman Khairy Assistant lecturer of plastic surgery

Examination of ulcer: Definition of an ulcer: An ulcer is defined as a break in the continuity of surface epithelium with superadded infection.

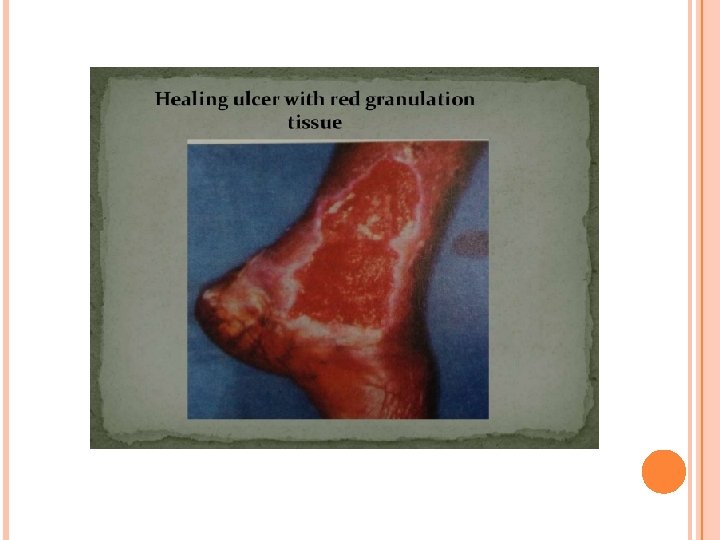
CLASSIFICATION OF ULCER Clinical Classification of Ulcer: — Spreading- with surrounding inflammation — Healing – Slopping edge with red granulation tissue —Callous- Ulcer with no tendency to heal-with pale granulation tissue. Pathological Classification of Ulcer: — Specific- Tuberculous, Syphylitic, Actinomycotic —Non specific- Traumatic( Mechanical, Physical, Chemical) Cryopathic, Arterial, Venous, Neurogenic, Trophic, Tropical, Bazin’s, Martorell’s, Meleney’s ulcer —Malignant- Squamous cell carcinoma, Basal Cell Carcinoma, Melanom



INSPECTION: • • • Size and shape: Tuberculosis ulcers are enerally oval in shape but their coalescence may give an irregular crescentic border. The size of an ulcer is important in deciding the time which will be required for healing. Abigger ulcer will definitely take longer time to heal than smaller ulcer. To record exactly the size and shape of an ulcer sterile gauze may be pressed on to the ulcer to get measurement.

Number: • Tuberculosis, gummatous, varicose and soft chancre may be more than one in number.

Position: • It is very important and often gives clue to the diagnosis. Rodent ulcer are usuall confined to the upper part of the face above a line joining the angle of the mouth to the lobule of the ear, occuring frequentlynear the inner canthus of the eye. Malignant ulcers are more commonly seen on the lips, tongue, breast and penis. •
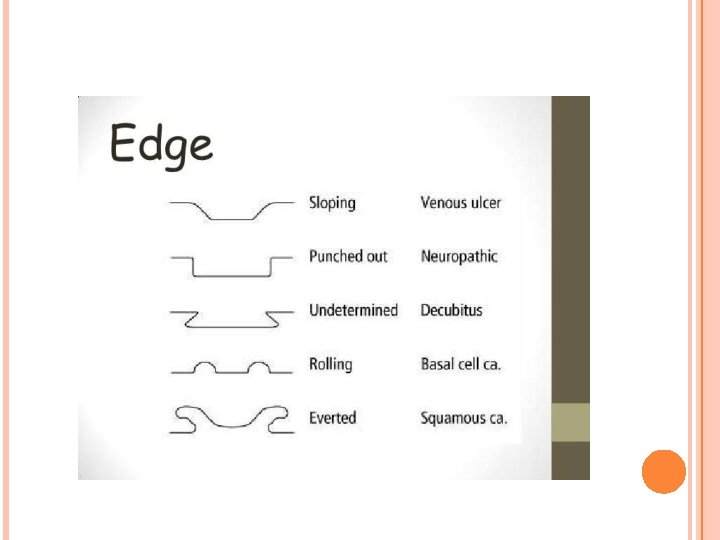

Edge: • In spreading ulcer the edges are inflammed and edematous whereas in a healing ulcer the edges, if traced from the red granulation tissue in the centre towards periphery, will show blue zone (due to thin growing epithelium) and a white zone (due to fibrosis of scar). Undermined edge – it is mostly seen in tuberculosis. The disease causing the ulcer spreads in an d destroys the subcutaneous tissue faster than it destroys the skin. The overhanging skin is thin friable, reddish blue and unhealthy. Punched out edges – it is mostly seen in gummatous ulcer or in a deep trophic ulcer. The edges drop down at right angle to the skin surface as if it has been cut out a punch. It is seen in diseases in which activity is limited to the ulcer itself and does not tend to spread to the surrounding tissues. • •

• • • Sloping edge – it is seen mostly in healing traumatic or venous ulcer. Every healing ulcer has a sloping egde, which is reddish purple in color and consists of new healthy epithelium. Raised and pearly white beaded edge – it is a feature of rodent ulcer which develpos in invasive cellular diseases and becomes necrotic at the centre. Rolled (everted)edge – it is characteristic feature of squamous cell carcinoma or an ulcerated adeno - carcinoma. This ulcer is caused by fast growing cellular disease, growing portion at the edge of the ulcer heaps up and spills over the normal skin to produce an everted edge.

Floor: • This is the exposed surface of the ulcer. One must be very careful to note what isthere at the floor of an ulcer. When floor is covered with red granulation tissue, the ulcer seems to be healthy and healing. Pale and smooth granulation tissue indicates a healing ulcer. Wash leather slough on the floor of ulcer is pathognomonic of gummatous ulcer. A black mass at the floor sugggests malignant melanoma. • •

Discharge: • The character of the discharge should be noted, its amount and smell. A healing ulcer will show scanty serous discharge, but the spreading and inflamed ulcer will show purulent discahrge. Serosanguineous discharge is often seen in a tuberculoses ulcer or a malignant ulcer. • •

Surrounding area: • If the surrounding area of an ulcer is glossy, red and edematous, the ulcer is acutely inflamed. Very often the surrounding skin of varicose ulcer is eczematous and pigmented. A scar or wrikling in surrounding a skin of an ulcer may well indicate an old case of tuberculosis. • •

PALPATION Tenderness: • An acutely inflamed ulcer is always exquisitely tender. Chronic ulcer are slightly tender. Neoplastic ulcers are never tender. • •

Base: • The student must understand the difference between the floor( exposed surface within the ulcer)and base(on which ulcer rests and it is better felt than seen) If an attempt is made to pick up the ulcer between thumb and the index finger, the base will be felt. Marked induration of the base is an important feature of squamous cell carcinoma and chancre. • •

Depth: • You should make assessment regarding depth of the ulcer. It can be recorded in the examination sheet in millimeters.

Bleeding: • Whether the ulcer bleeds on touch should be checked as it is a common feature of malignant ulcer.

Relation with deeper structures: • The ulcer is made to move over the deeper structures to know whether it is fixed to any of these structures. A gummatous ulcer over a subcutaneous tissue or bone is often fixed to it. Malignant ulcer will be fixed to any of the deeper structure by infiltration. •

THANK YOU
- Slides: 21