EXAMINATION OF RESPIRATORY SYSTEM INSPECTION PALPATION AUSCULTATION PERCUSSION


















































- Slides: 60
EXAMINATION OF RESPIRATORY SYSTEM
§ § INSPECTION PALPATION AUSCULTATION PERCUSSION
GENERAL EXAMINATION CYANOSIS § Central § Peripheral causes § COPD § Type 2 resp. failure § Pulmonary fibrosis § B. asthma § Congenital cyanotic heart disease § Pulmonary embolism
OEDEMA Right ventricular failure—cor pulmonale FACE § Pink puffers § Blue bloaters § Congested neck veins § Rashes
EYES § Horner, s syndrome---ca. bronchus § Chemosis---SVC obstruction ---COPD NECK Lymph nodes----TB ---lymphoma --sarcoidosis ---malignancy
SKIN § Rashes—herpes zoster § Scars---previous operation, burns , biopsies § Pigmentation—haemochromotosis § Dilated veins---SVC obstruction
HANDS § Cyanosis § Clubbing---ca. bronchus ---TB ---empyema ---abcess ---fibrosing alveolitis ---bronchiectasis § Wasting of small muscles of hand ---pancoast tumour
PULSE § Tachycardia---> 120/min—infections ---P. E --B. asthma --COPD exacerbation § Small volume
§ Collapsing pulse—large volume bounding pulse , carbon dioxide retention --type 2 resp. failure PULSES PARADOXUS § Status asthmaticus § Massive pulmonary embolism § Tension pneumothorax
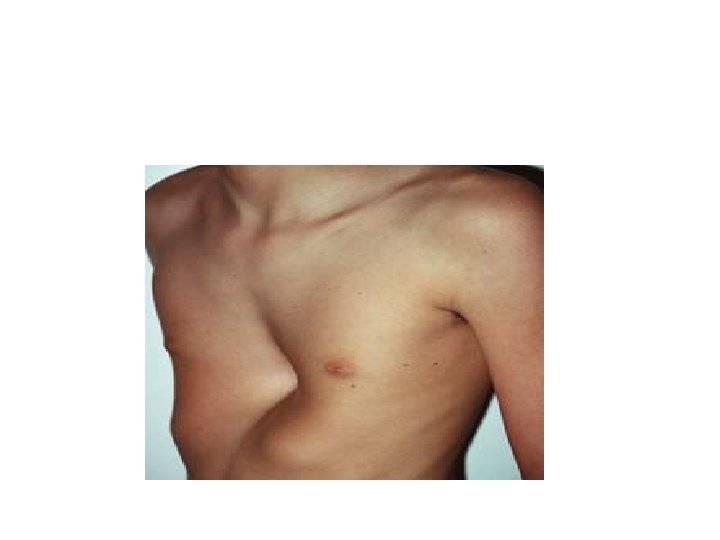
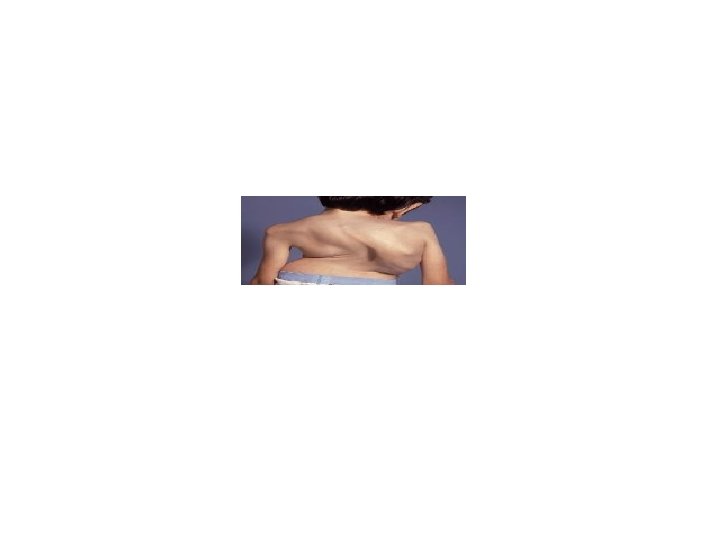
EXAMINATION OF THE CHEST Inspection § A-P diameter --pectus excavatum---funnel chest --pectus carinatum---pigeon chest § kyphoscoliosis § respiratory movements---resp. rate-{14 -18/min} i: e –hyperventillation—DKA, PE ---hypoventillation—type 2 resp. failure
§ Chyne stokes breathing---cyclical variation in the depth of respiration with period of apnoea. § Use of accessory muscles---status asthmaticus § Tenderness—fractured ribs, metastasis , neuralgia
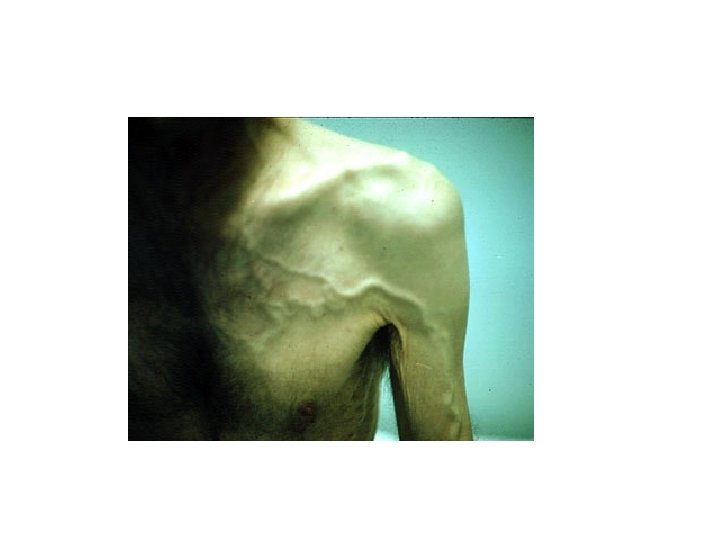
v. SHAPE OF THE CHEST v. Pectus excavetum v. Pectus carinatum DILATED VEINS v. SVC obstruction---Ca lung
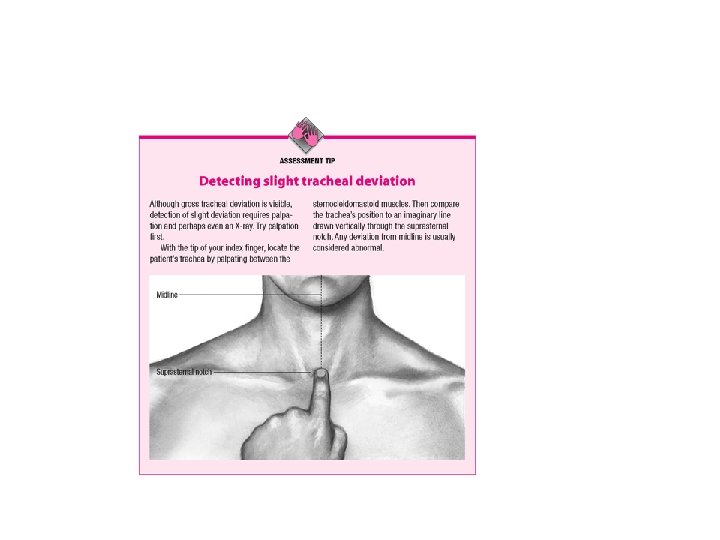
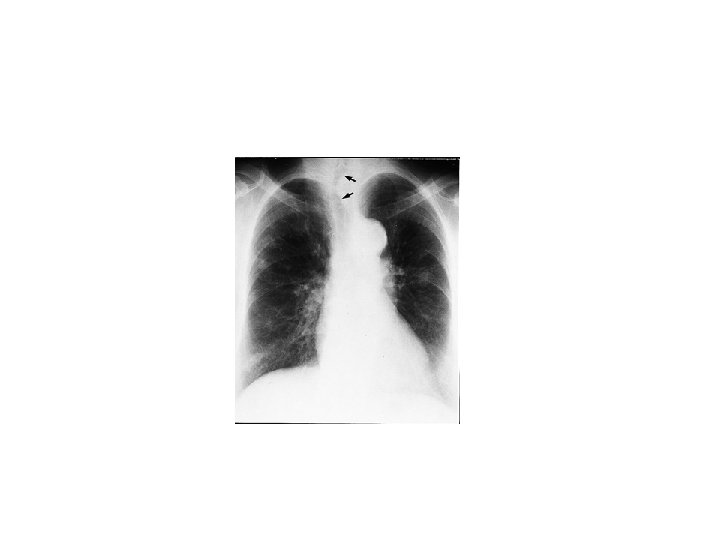
Palpation Trachea 4 -5 cm of the upper trachea can be felt in the neck between the cricoid cartilage and the sternal notch. § Pushed –pneumothorax -pleural effusion § Pulled—fibrosis --collapse
§ Chest expansion– normal up to 5 cm -abnormal < 2 cm § Apex beat § Tactile fremitus --Ask the patient to say 99 --you should feel the vibration transmitted through the airways to the lung.
§ Increased in---pneumothorax --emphysema § Decreased---pleural effusion Auscultation Breath sounds— § Vesicular—normal --insp. twice that of expiration --no pause § Bronchial –inspiration is shorter than expiration ---gap between insp. and exp.
Vesicular bronchial
§ Increased---consolidation ---large cavity near the surface § Decreased---COPD ---Pleural effusion --pneumothorax
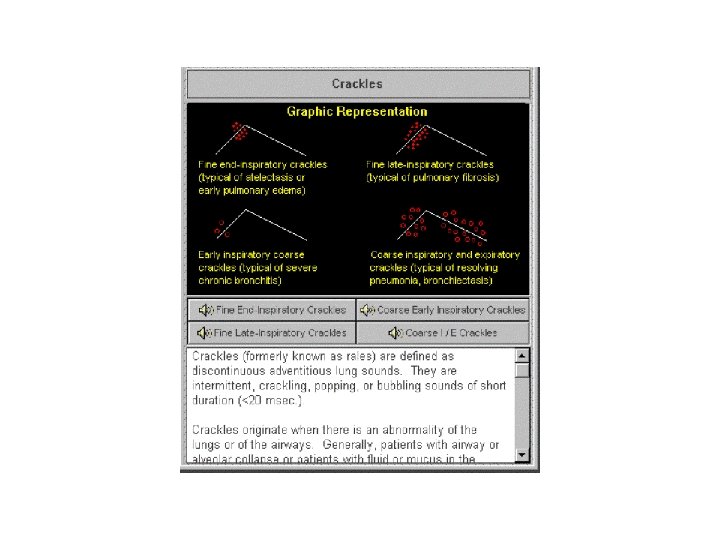
Added sounds § Crepitations---fine ---heart failure --fibrosing alveolitis ---coarse—bronchiectasis --infections § Wheezes or rhonchi---COPD --bronchial asthma
• Pleural rub • Whispering pectroloquy---consolidation --ask the patient to whisper 99 --you should hear only faint sounds or nothing----if you hear the sound clearly then this is referred as whispering pectroloquy.
§ Egophany --ask the patient to say “ ee “ continously --you should hear muffled ‘’ee ‘’---if you hear an ‘’ ay ‘’ then it is egophany.
Percussion § The percussion note loses its normal resonance when ever aerated lung tissue is separated from the chest wall by fluid or pleural thickening. OR § When lung tissue is separated from chest wall by collapse or consolidation or fibrosis