EvidenceBased Smoking Cessation Counseling for HIVInfected Patients Julia

Evidence-Based Smoking Cessation Counseling for HIV-Infected Patients Julia H. Arnsten, MD, MPH Chief, Division of General Internal Medicine Associate Professor of Medicine, Epidemiology, and Psychiatry Albert Einstein College of Medicine Montefiore Medical Center Submitted by the NY/NJ AETC

Background • More than 50% of HIV-infected patients smoke • Smoking poses unique health risks to HIVinfected patients – pulmonary infections – oropharyngeal lesions – AIDS-defining and non-AIDS-defining malignancies. • “Graying” of HIV-infected population necessitates screening for and prevention of chronic disease – Coronary heart disease – Diabetes – Obesity

Prevalence of Current Smoking in HIVInfected Persons in 5 Cross-Sectional Studies 2001 – 2005 PCHIS = SF, LA, IL, NJ, NY, MI; HCSUS = 8 metropolitan areas

Prevalence of smoking among HIVinfected patients in NYC Burkhaler et al, Tobacco use and readiness to quit smoking in low-income HIVinfected persons, Nicotine Tob Res, 2005; 7(4): 511 -22. • 428 HIV+ Medicaid recipients, NYC – – Age: 22 -75 59% males 53% African Americans, 30% Latinos HS education or less : 87% • 67% current smokers (mean = 16 cig/day) • 19% former smokers, 16% never smokers • Current smokers – Greater use of illicit substances (ever and current) – Lower perceived health risk of continued smoking

Adult smoking rates NYC 2003 21. 5% 2004 18. 9% USA 2003 21. 6% 2004 20. 7%

HIV Patients are Living Longer
 Source: SPARCS (Statewide Planning and")
Distribution of HIV/AIDS Discharges by Age-group, 1994 -2002 (NYS) Source: SPARCS (Statewide Planning and Research Cooperative System)
 Source: NYS")
Distribution of Medicaid recipients with HIV/AIDS by age group, 1993 -2001 (NYS) Source: NYS Medicaid Claims Database

Living Longer = Changing Morbidity and Mortality Cancer Lung disease Cardiovascular disease

Cancer rates before and after HAART
 Before and After HAART Cases per 1000 pat-years")
AIDS-Defining and Non AIDS-Defining Malignancies (non-ADM) Before and After HAART Cases per 1000 pat-years Bedimo, R et al. Trends in AIDS-defining and non-AIDS-defining malignancies among HIV-infected patients: 1989 -2002. Clin Inf Dis 2004; 39: 1380 -1384

Cancers of the larynx and oropharynx HAART

Cancers of the lung/trachea Source: SPARCS

Lung disease

Chronic Bronchitis and Emphysema Source: SPARCS database, NYSDOH

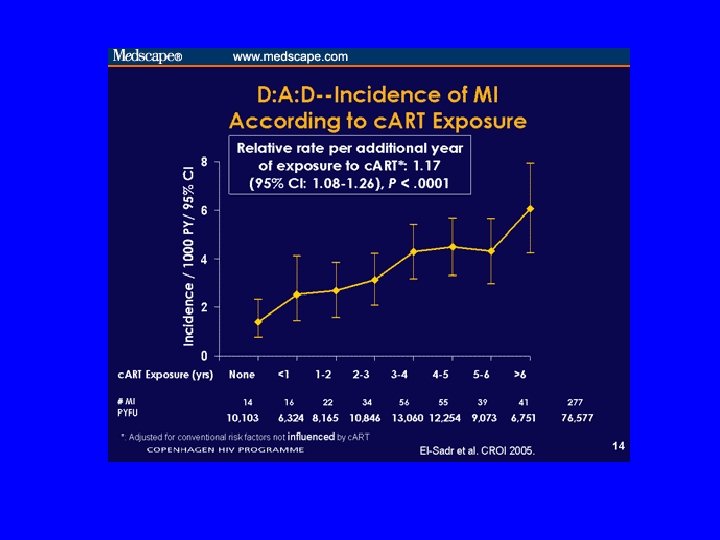
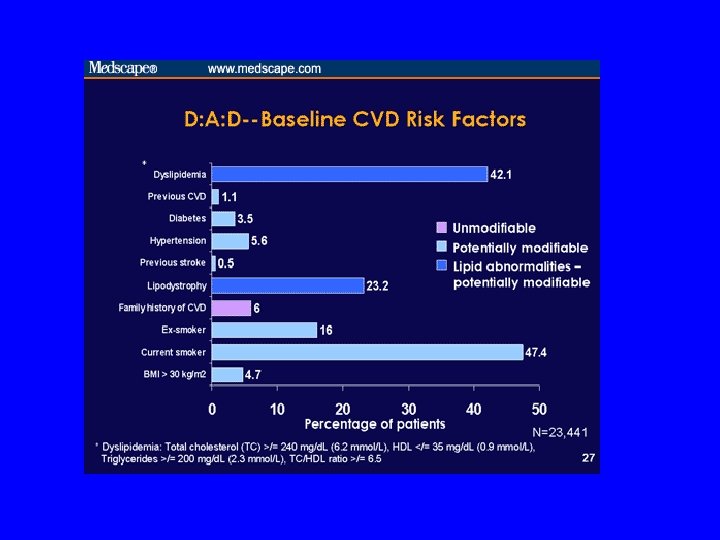
Cardiovascular disease

Myocardial infarction Holmberg et al. Trends in rates of Myocardial infarction among patients with HIV N Engl J Med 2004; 350: 730 -731

Acute Myocardial Infarction Source: SPARCS database, NYSDOH

Risk Factors Are Additive The total severity of multiple low-level risk factors often exceeds that of a single severely elevated risk factor. Mean Absolute Risk (%) 27% 19% 13% 8% BP 165/95 mm Hg Age 56 years LDL-C 155 mg/d. L Grundy SM et al. J Am Coll Cardiol 1999; 34: 1348 -1359. BP 165/95 mm Hg Age 56 years LDL-C 155 mg/d. L Smoker

Are physicians intervening in tobacco use? Ellerbeck, Ahluwalia, et al. Direct observation of smoking cessation activities in primary care practice. J Fam Pract. 2001; 50: 688 -693 In 38 primary care practices: Tobacco was discussed in 21% of encounters. Discussion was: – more common in those practices (58%) with standard forms for recording smoking status – more common during new patient visits – less common with older patients – less common with physicians in practice more than 10 years

Barriers to treating tobacco dependence “Not enough time. ” “Patients don’t want to hear about it. ” “I can’t help patients stop. ”

“Not enough time” “Minimal interventions lasting less than 3 minutes increase overall tobacco abstinence rates. ” The PHS Guideline (Strength of Evidence = A)

“Patients don’t want to hear about it” • In several studies, smoking cessation interventions during physician visits were associated with increased patient satisfaction with care among smokers • 1, 898 patients who reported that they had been asked about tobacco use or advised to quit during the latest visit had 10% greater satisfaction rating and 5% less dissatisfaction than those not reporting such discussions Mayo Clin Proc. 2001; 76: 138 -143

Proportion of Patients Reporting Positive Changes in Health Promoting Behavior Following Diagnosis with HIV Collins et al, Health Psychology 2001; 20(5): 351 -360

Proportion of Patients Interested in Quitting Smoking Mamary et al, Cigarette smoking and the desire to quit among individuals living with HIV, AIDS Patients Care and STDs 2002; 16(1): 39 -42

“I can’t help patients stop” Effective clinical interventions exist The Public Health Service Clinical Practice Guideline Treating Tobacco Use and Dependence was published in June, 2000 and offers effective treatments for tobacco dependence.

Summary Algorithm for Treating Tobacco Dependence

The 5 A’s For Patients Willing To Quit • ASK about tobacco use at every visit. • ADVISE to quit with a clear, strong, personalized message. • ASSESS willingness to make a quit attempt within the next 30 days. • ASSIST in quit attempt with a brief (3 -5 min) counseling intervention. • ARRANGE for follow-up (ANTICIPATE relapse).

ASK EVERY patient at EVERY visit

ADVISE • Once tobacco use status has been identified and documented, advise all tobacco users to quit • Even brief advice to quit results in greater quit rates • Advice should be: - clear - strong - personalized “As your health care provider, I must tell you that the most important thing you can do to improve your health is to stop smoking. ”

ASSESS After providing a clear, strong, and personalized message to quit, you must determine whether the patient is willing to quit at this time “Are you willing to try to quit at this time? I can help you. ”

ASSIST • Help develop a quit plan • Provide practical counseling – Identify events, internal states, or activities that increase the risk of smoking or relapse (e. g. drinking, other smokers). – Identify and practice coping or problem-solving skills. – Provide basic information about smoking and successful quitting. • Provide intra-treatment social support – Encourage the patient in the quit attempt. – Communicate caring and concern. – Encourage the patient to talk about the quitting process • Help patient obtain extra-treatment social support • Recommend pharmacotherapy (ex. special circumstances) • Provide supplementary materials

Developing a quit plan • Set a quit date • Review past quit attempts • Anticipate challenges • Remove tobacco products • Avoid – Alcohol use – Exposure to tobacco

Counsel your patients to quit “Minimal interventions lasting less than 3 minutes increase overall tobacco abstinence rates” The PHS Guideline (Strength of Evidence = A) “There is a strong dose-response relation between the session length of person-to-person contact and successful treatment outcomes. Intensive interventions are more effective than less intensive interventions and should be used whenever possible” The PHS Guideline (Strength of Evidence = A)

Brief Intervention • 5 -15 minute counseling session • Four components – State your concern about your patient’s behaviors (smoking, use of alcohol/drugs, diet) – Make explicit recommendation for change in behavior – Discuss patient’s reaction – Review treatment options; negotiate plan

ARRANGE and ANTICIPATE • Schedule a follow-up contact within one week after the quit date – Telephone contact – Quit lines • The majority of relapse occurs in the first two weeks after quitting

Relapse • Preventing Relapse – Congratulate success – Encourage continued abstinence – Discuss with your patient: • benefits of quitting • barriers “How has stopping tobacco use helped you? . ” • If your patient has used tobacco, remind him or her that the relapse should be viewed as a learning experience • Relapse is consistent with the chronic nature of tobacco dependence; not a sign of failure

Cell Phone Intervention Pilot Study: Houston, Texas Lazev et al, Increasing access to smoking cessation treatment in a low-income, HIV-positive population: The feasibility of cellular telephones. Nicotine & Tobacco Research, 2004; 6(2): 281 -286. • Pilot study of a proactive cell phone smoking cessation intervention (n=20) • Thomas St. Clinic – 4000 medically indigent patients (mostly Black and Hispanic) • Six scheduled cell-phone delivered counseling sessions delivered over two weeks (1 d prior to quit date, on quit date, and 2, 4, 7, and 14 d post) – average 5 min • 24 hr/7 d/week quit line, patient info also provided • Highly successful: 95% made a quit attempt and 75% were abstinent at 1 and 2 weeks post quit date

A Nurse-Managed, Peer-Led Cessation Intervention for HIV-Positive Smokers Wewers et al, Jour Assn of Nurses in AIDS Care 2000; 11(6): 37 -44 • Randomized trial of 15 participants • Intervention = weekly counseling sessions plus NRT • Control group = written materials • Follow-up: 8 weeks, 8 months • Outcomes = point abstinence and continuous abstinence

Treating patients who are not ready to make a quit attempt with Motivational Interviewing (a Form of Brief Intervention) • RELEVANCE: Tailor advice and discussion to each patient, avoid argument! • RISKS: Outline specific risks of smoking. • REWARDS: Outline the benefits of quitting. • ROADBLOCKS: Identify barriers to quitting. • REPETITION: Reinforce the motivational message at every visit, avoid argument!

Motivational Interviewing Motivational interviewing is a directive, client-centered counseling style for eliciting behavior change by helping clients to explore and resolve ambivalence. Stephen Rollnick, William R. Miller, 1995 Rollnick, S. , & Miller, W. R. What is motivational interviewing? Behavioural and Cognitive Psychotherapy. 1995; 23: 325 -334.

Readiness to Change Model

Stages of Change in Two Populations of HIV-Infected Smokers, Compared to General Population NY: Burkhaler et al, Tobacco use and readiness to quit smoking in low-income HIVinfected persons, Nicotine Tob Res, 2005; 7(4): 511 -22. Houston: Gritz et al, Smoking behavior in a low-income multiethnic HIV/AIDS population, Nicotine Tob Res, 2004; 6(1): 71 -77.

Precontemplation àGoal is to raise doubt, increase perception/ consciousness of problem àexpress concern àstate the problem non-judgmentally àagree to disagree àadvise a trial of abstinence or cutting down àimportance of follow-up (even if still smoking/using drug & alcohol ) àless intensity is better Samet, JH, Rollnick S, Barnes H. Arch Intern Med. 1996; 156: 2287 -93.

Contemplation àGoal is to tip the balance àelicit positive and negative aspects of smoking or drug & alcohol use àelicit positive and negative aspects of not smoking or using drugs & alcohols àsummarize (patient could write these down) àdemonstrate discrepancies between values and actions àadvise a trial of abstinence or cutting down

Preparation àGoal is to help determine the best course of action àworking on motivation is not helpful àsupporting self-efficacy is (remind of strengths--i. e. previous quits, periods of sobriety, coming to doctor) àhelp decide on achievable goals àcaution re: difficult road ahead àrelapse won’t disrupt relationship

Action àGoal is to help patient take steps to change àsupport and encouragement àacknowledge discomfort (losses, withdrawal) àreinforce importance of recovery
 àrecognize the ongoing")
Maintenance àGoal is to help prevent relapse àanticipate difficult situations (triggers) àrecognize the ongoing struggle àsupport the patient’s resolve àreiterate that relapse won’t disrupt your relationship

Relapse àGoal is to renew the process of contemplation àexplore what can be learned from the relapse àexpress concern àemphasize the positive aspects of prior abstinence and of current efforts to quit smoking or drug & alcohol use àsupport self-efficacy
 àFEEDBACK of personal risk or impairment ài. e.")
Ingredients of Effective Brief Interventions (FRAMES) àFEEDBACK of personal risk or impairment ài. e. CHD, lung disease, state consequences or risks àemphasis on personal RESPONSIBILITY for change à“…it’s up to you to decide…” àclear ADVICE to change àidentify the problem, explain why change is important, advocate specific change
 àa MENU of alternatives àa range of options")
Ingredients of Effective Brief Interventions (FRAMES) àa MENU of alternatives àa range of options àEMPATHIC counseling style àunderstanding and reflective àenhancement of SELF-EFFICACY àreinforce it, state your belief they can do it
")
Physician’s Treatment Goals • Maintain awareness of smoking (and other drug & alcohol issues) • Ask, assess and advise about smoking • Consider smoking (and drug & alcohol problems) as a mainstream medical issues • Counsel patients about behavior change at every visit

SMOKING CESSATION FOR THE SECONDARY PREVENTION OF CORONARY HEART DISEASE Critchley, J. Capewell, S. Cochrane Heart Group Cochrane Database of Systematic Reviews. 1, 2006

BACKGROUND • Smoking is an established risk factor for coronary heart disease • The impact of smoking cessation on risk for coronary heart disease is less well established

METHODS • Meta-analysis to estimate the magnitude of risk reduction when a patient with CHD stops smoking • Search: – Cochrane Register of Controlled Trials (CENTRAL), MEDLINE, EMBASE, Science Citation Index, CINAHL, Psych. Lit, Dissertation Abstracts, BIDSISI Index to Scientific and Technical Proceedings, UK National Research Register

METHODS • Selection: – Prospective cohort studies of patients with a diagnosis of CHD, which include all-cause mortality as an outcome measure – Smoking status measured at least twice to ascertain which smokers have quit – Subjects followed-up for at least two years
 of mortality for")
RESULTS • Twenty studies • Reduction in crude relative risk (RR) of mortality for those who quit smoking compared with those who continued to smoke – RR 0. 64, 95% confidence interval 0. 58 to 0. 71 • Reduction in non-fatal myocardial infarctions – RR 0. 68, 95% confidence interval 0. 57 to 0. 82

RESULTS SIX HIGHEST QUALITY STUDIES

CONCLUSION • Smoking cessation is associated with a substantial reduction in the risk of all-cause mortality among patients with CHD • Risk reduction comparable with other secondary preventive therapies such as cholesterol lowering • The risk reduction associated with smoking cessation consistent regardless of differences between the studies in terms of index cardiac events, age, sex, country, and time period
- Slides: 65