Evaluation of the bleeding patient V Kinsella M

Evaluation of the bleeding patient V. Kinsella M. D. January, 27 2006

MILD bleeding 1. Platelets secretion disorders 2. v. W deficiency 3. Platelets dense granules deficiency 4. Unknown

Hemostasis and thrombosis n Dependent on 3 factors: Vascular endothelium 2. Platelets 3. Coagulation system 1.

1. Clinical aspects of bleeding

1. Clinical aspects of bleeding Evaluation of patients with bleeding is a multi-step process: n Complete n Detailed history physical exam n Laboratory evaluation

history 1. Is there a personal or family history of bleeding after surgical procedures, dental procedures, childbirth, or trauma? 2. When the bleeding episode started? 3. Has the patient received medications that can cause or make worse a bleeding problem?

history Many drugs can contribute to bleeding; semisynthetic penicillins cephalosporins calcium channel blocker dipyridamole thiazides alcohol quinine, quinidine chlorpromazine, sulfonamides INH, rifampin methyldopa phenytoin, barbiturates, warfarin, heparin, thrombolytic agents NSAIDs, ASA allopurinol TMP/SMX
 2. Look for hepatosplenomegaly")
physical exam 1. Assess volume status (correct shock if present) 2. Look for hepatosplenomegaly 3. Do a rectal exam for evidence of GI bleeding 4. Examine oropharynx for evidence of petechiae

Clinical aspects of bleeding

physical exam 5. Look for physical signs and symptoms of diseases related to capillary fragility: n Cushing’s syndrome, Marfan syndrome or exogenous steroids n "senile purpura” n Petechiae secondary to coughing, sneezing, Valsalva maneuver, blood pressure measurement n vasculitis ("palpable purpura") n Telangiectasias (Osler-Weber-Rendu syndrome) (HHT)
 Do not blanch with pressure (angiomas) Not palpable (vasculitis)")
petechiae (typical of platelet disorders) Do not blanch with pressure (angiomas) Not palpable (vasculitis)
")
vasculitis (palpable rash)

2. Hematologic disorders causing bleeding – Platelet disorders – Coagulation factor disorders

Clinical differentiation Platelets x Coagulation Defects

Platelets Defects • Generally have immediate onset of bleeding after trauma • Bleeding is predominantly in skin, mucous membranes, nose, GI tract, and urinary tract • Bleeding may be observed as petechiae (<3 mm) or ecchymoses (>3 mm

Clinical aspects of bleeding
 is")
Coagulation Defects n "Deep" bleeding (in the joint spaces, muscles, and retroperitoneal spaces) is common. Observed on exam as hematomas and hemarthroses.
")
Hematoma (typical of coagulation factor disorders)
")
Hemarthrosis (acute)

Laboratory Evaluation of Bleeding CBC and smear Platelet count Thrombocytopenia RBC and platelet morphology TTP, DIC, etc. Coagulation defects PT extrinsic/common pathways PTT Intrinsic/common pathways Coag. factor assays Specific factor 50: 50 mix Inhibitors (e. g. , antibodies) Fibrinogen assay Decreased fibrinogen Thrombin time Qualitative/quantitative fibrinogen D-dimer Fibrinolysis (DIC) deficiencies

Laboratory Evaluation of Bleeding Platelet function von Willebrand factor v. WD Bleeding time In vivo test (non-specific) Platelet function analyzer (PFA) Qualitative platelet disorders
 Prothrombin time (PT) Surface")
Laboratory Evaluation of the Coagulation Pathways Partial thromboplastin time (PTT) Prothrombin time (PT) Surface activating agent (Ellagic acid, kaolin) Phospholipid Calcium Thromboplastin Tissue factor Phospholipid Calcium Intrinsic pathway Extrinsic pathway Thrombin time Common pathway Thrombin Fibrin clot
 XII Extrinsic system (tissue damage) XIIa Tissue factor")
Coagulation cascade Intrinsic system (surface contact) XII Extrinsic system (tissue damage) XIIa Tissue factor XIa XI IX IXa VIII VIIa VIIIa X Vitamin K dependant factors VII Xa V Va II Fibrinogen IIa (Thrombin) Fibrin

Initial Evaluation of a Bleeding Patient Normal PTT Consider evaluating for: Platelet disorder Mild factor deficiency Factor XIII Monoclonal gammopathy Abnormal fibrinolysis a 2 anti-plasmin deficiency Vascular disorders Dysfibrinogenemia

Initial Evaluation of a Bleeding Patient Elevated PT Normal PTT Repeat with 50: 50 mix is abnormal Test for inhibitor activity: 1. Specific: Factor VII (rare) 2. Non-specific: Anti-phospholipid 50: 50 mix is normal Test for factor deficiency: 1. Multiple factor deficiencies (common) (Liver disease, vitamin K deficiency, warfarin, DIC) 2. Deficiency of factor VII (rare)

Initial Evaluation of a Bleeding Patient Normal PT Abnormal PTT Repeat with 50: 50 mix is abnormal Test for inhibitor activity: Specific factors: VIII, IX, XI Non-specific (anti-phospholipid) 50: 50 mix is normal Test for factor deficiency: Isolated deficiency in intrinsic pathway (factors VIII, IX, XI) Multiple factor deficiencies (rare)

Initial Evaluation of a Bleeding Patient Abnormal PTT Repeat with 50: 50 mix is abnormal Test for inhibitor activity: Specific : Factors V, X, prothrombin, fibrinogen (rare) Non-specific: anti-phospholipid (common) 50: 50 mix is normal Test for factor deficiency: Isolated deficiency in common pathway: Factors V, X, Prothrombin, Fibrinogen Multiple factor deficiencies (common) (Liver disease, vitamin K deficiency, warfarin, DIC)

Bleeding time n 5 -10% of patients hospitalized patients have a prolonged bleeding time n Most of the prolonged bleeding times are due to aspirin or drug ingestion n Prolonged bleeding time does not predict excess surgical blood loss n Not recommended for routine testing in preoperative patients

Thrombin Time n Measures rate of fibrinogen conversion to fibrin n Procedure: – Add thrombin with patient plasma – Measure time to clot n Variables: – Source and quantity of thrombin

Causes of prolonged Thrombin Time n n n Heparin Hypofibrinogenemia Dysfibrinogenemia Paraprotein Thrombin inhibitors (Hirudin) Thrombin antibodies

PLATELETS

Approach to the thrombocytopenic patient n History 1. Is the patient bleeding? 2. Are there symptoms of a secondary illness? (neoplasm, infection, autoimmune disease) 3. Is there a history of medications, alcohol use, or recent transfusion?

Approach to the thrombocytopenic patient n History 4. Are there risk factors for viral infection? 5. Is there a family history of thrombocytopenia? 6. Do the sites of bleeding suggest a platelet defect?

Approach to the thrombocytopenic patient n Assess the number and function of platelets – CBC with peripheral smear – Bleeding time – Platelet aggregation study – PFA

Classification of platelet disorders n Quantitative disorders – Abnormal distribution – Dilution effect – Decreased production – Increased destruction
 – Acquired disorders")
Classification of platelet disorders n Qualitative disorders – Inherited disorders (rare) – Acquired disorders § § § Immune Medications Chronic renal failure Cardiopulmonary bypass Liver disease

Inherited platelet disorders Rare congenital abnormalities on synthesis or release of secretory granules

Inherited platelet disorders n Gray platelets syndrome: No alpha granules

Inherited platelet disorders n May-Hegglin: Thrombocytopenia Large platelets Neutrophils – Dohle bodies

Inherited platelet disorders n Glazmann’s thrombasthenia: Congenital deficiency or abnormality of GP IIb-IIIa n Bernard-Solier syndrome: Congenital deficiency or abnormality of GP Ib

Acquired platelet disorders n Decreased production: Ineffective thrombopoiesis - MDS n Increased destruction: Immune Non-immune n Poor aggregation

Increased platelets destruction 1. Immune-mediated Idiopathic - ITP Drug-induced Collagen vascular disease Lymphoproliferative disease Sarcoidosis 2. Non-immune mediated DIC Microangiopathic hemolytic anemia

ITP is a diagnosis of exclusion !

Initial Treatment of ITP Platelet count Symptoms >50, 000 None 20 -50, 000 Not bleeding None Bleeding Glucocorticoids IVIG Not bleeding Glucocorticoids Bleeding Glucocorticoids IVIG Hospitalization Rituximab <20, 000 Treatment

COAGULATION FACTOR DEFECTS
")
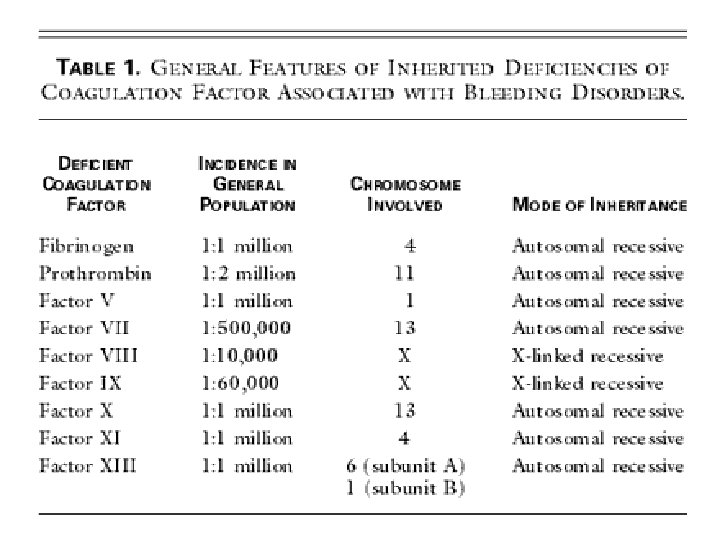
Inherited Coagulation factor bleeding disorders – von. Willebrand’s disease – Hemophilia (A and B)

von. Willebrand disease – Most common hereditary coagulation disorder – Autossomal dominant – Incidence 1: 1000 Erik A. von. Willenbrand M. D. (1870 -1949)

von. Willebrand factor – Synthesis in endothelium and megakaryocytes – Forms large multimers – Carrier of factor VIII – Anchors platelets to subendothelium – Bridge between platelets
 causes decreased")
von. Willebrand disease n Abnormal synthesis of von Willebrand factor (v. WF) causes decreased platelet adhesion and decreased serum levels of factor VIII
 Partial quantitative deficiency – Type 2")
von. Willebrand disease Classification – Type 1 (“decreased”) Partial quantitative deficiency – Type 2 (“abnormal”) Qualitative deficiency – Type 3 (“absent”) Total quantitative deficiency

von. Willebrand disease Laboratory evaluation: von. Willebrand type Assay 1 2 3 v. WF antigen ß Normal ßß v. WF activity ß ß ßß Normal Absent Multimer analysis Normal
 – plasma VWF levels")
Treatment of von Willebrand Disease n DDAVP (deamino-8 -arginine vasopressin) – plasma VWF levels by stimulating secretion from endothelium – Duration of response is variable – Not generally used in type 2 disease – Dosage 0. 3 µg/kg q 12 hr IV

Treatment of von Willebrand Disease n Cryoprecipitate – Source of fibrinogen, factor VIII and VWF – Only plasma fraction that consistently contains VWF multimers Factor VIII concentrate (Intermediate purity) – Virally inactivated product – Humate-P or Koate-HS
 1. Prolonged bleeding after surgery")
Hemophilia Clinical manifestations (hemophilia A & B are indistinguishable) 1. Prolonged bleeding after surgery or dental extractions 2. Hemarthrosis (most common) 3. Soft tissue hematomas 4. Other sites of bleeding Urinary tract CNS, neck (may be life-threatening)

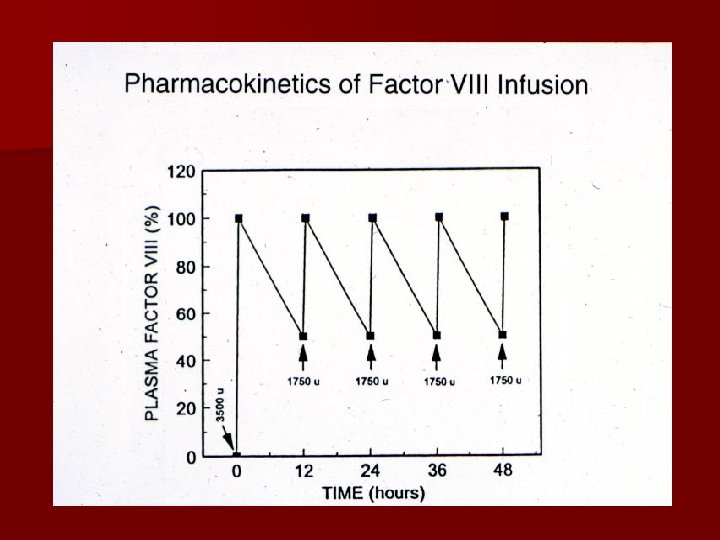
Dosing guidelines for hemophilia A n Mild bleeding: Hemarthrosis, oropharyngeal or dental, epistaxis, hematuria Target: 30% dosing q 8 -12 h; 1 -2 days (15 U/kg) n Major bleeding – – CNS trauma, hemorrhage, lumbar puncture Surgery Retroperitoneal hemorrhage GI bleeding Target: 80 -100% q 8 -12 h; 7 -14 days (50 U/kg) n Adjunctive therapy – -aminocaproic acid (Amicar) or DDAVP (for mild disease only)

Treatment of hemophilia B n Agent – High purity factor IX – Recombinant human factor IX n Dose – Initial dose: 100 U/kg – Subsequent: 50 U/kg every 24 hours

Acquired bleeding disorders: 1. Vitamin K deficiency 2. Liver disease 3. Warfarin overdose 4. DIC 5. Inhibitors to CF

Vitamin K deficiency

Vitamin K deficiency n Source of vitamin K : Green vegetables Synthesized by intestinal flora n Required for synthesis Factors II, VII, IX , X Protein C and S n Causes of deficiency : Malnutrition Billiary obstruction Malabsorption Antibiotic therapy

Vitamin K deficiency n Treatment: Vitamin K replacement Fresh frozen plasma

DIC

Disseminated Intravascular Coagulation Activation of both coagulation and fibrinolysis Triggered by n Sepsis n Trauma – Head injury – Fat embolism n Malignancy n Obstetrical complications – Amniotic fluid embolism – Abruptio placentae n Vascular disorders n Reaction to toxin (e. g. snake venom, drugs) n Immunologic disorders – Severe allergic reaction – Transplant rejection
 Mechanism Systemic activation of coagulation Intravascular deposition of fibrin Activation")
Disseminated Intravascular Coagulation (DIC) Mechanism Systemic activation of coagulation Intravascular deposition of fibrin Activation of fibrinolysis Thrombosis of small and midsize vessels tissue hypoxia and organ failure Depletion of platelets and coagulation factors Bleeding

Pathogenesis of DIC Release of thromboplastic material into circulation Coagulation Fibrinolysis Fibrinogen Plasmin Thrombin Fibrin Monomers Fibrin Clot (intravascular) Consumption of coagulation factors; presence of FDPs a. PTT PT TT Fibrinogen Presence of plasmin D-dimer Fibrin(ogen) Degradation Products Plasmin Intravascular clot Platelets Schistocytes

Disseminated Intravascular Coagulation Treatment approaches n Treatment of underlying disorder n Anticoagulation with heparin n Platelet transfusion n Fresh frozen plasma n Coagulation inhibitor concentrate (ATIII)

Hemostasis in liver disease

Liver Disease and Hemostasis 1. Decreased synthesis of II, VII, IX, X, XI, and fibrinogen 2. Dietary Vitamin K deficiency (Inadequate intake or malabsortion) 3. Dysfibrinogenemia 4. Enhanced fibrinolysis (Decreased alpha 2 -antiplasmin) 5. DIC 6. Thrombocytopenia due to hypersplenism

Management of Hemostatic Defects in Liver Disease §Treatment for prolonged PT/PTT § Vitamin K 10 mg SQ x 3 days - usually ineffective § Fresh-frozen plasma infusion: 25 -30% of plasma volume (1200 -1500 ml) (immediate but temporary effect) Treatment for low fibrinogen § Cryoprecipitate (1 unit/10 kg body

Warfarin Toxicity

Warfarin overdose Managing high INR values Clinical situation Guidelines INR therapeutic-5 Lower or omit next dose; Resume therapy when INR is therapeutic INR 5 -9; no bleeding Lower or omit next one or two dose; Resume therapy when INR is therapeutic Omit dose and give vitamin K ( 1 -2 mg po) Rapid reversal: vitamin K 2 -4 mg po (repeat) INR >9; no bleeding Omit dose; vitamin K 10 mg po; repeat as necessary Resume therapy at lower dose when INR therapeutic Chest 2004: 126; 213 S (supplement)

Warfarin overdose Managing high INR values in bleeding patients Clinical situation Serious bleeding at Any elevation INR Guidelines Omit warfarin Vitamin K 10 mg slow IV infusion Omit warfarin Repeat vitamin K injections every 12 hrs FFP, PCC or Factor VIIa (depending on urgency) Any life-threatening Vitamin K 10 mg slow IV infusion PCC ( or recombinant human factor VIIa) Repeat vitamin K injections every 12 hrs Chest 2004: 126; 213 S (supplement)

Approach to Post-operative bleeding 1. Is the bleeding local or due to a hemostatic failure? § Local: Single site of bleeding usually rapid with minimal coagulation test abnormalities § Hemostatic failure: Multiple site or unusual pattern with abnormal coagulation tests

Approach to Post-operative bleeding 2. 3. Evaluate for causes of peri-operative hemostatic failure § Preexisting abnormality § Special cases (e. g. Cardiopulmonmary bypass) Diagnosis of hemostatic failure § Review pre-operative testing § Obtain updated testing

Approach to bleeding disorders Summary n Identify and correct any specific defect of hemostasis – Laboratory testing is always needed to establish the cause of bleeding – Screening tests (PT, PTT, platelet count) will often allow placement into one of the broad categories – Specialized testing is usually necessary to establish a specific diagnosis n Use non-transfusional drugs whenever possible n RBC transfusions for surgical procedures or large blood loss

THANK YOU!
 n Mechanism – Direct activation of common")
Recombinant human factor VIIa (rh. VIIa; Novoseven) n Mechanism – Direct activation of common pathway n Use – – Factor VIII inhibitors Bleeding with other clotting disorders Warfarin overdose with bleeding CNS bleeding with or without warfarin – Dose – 90 µg/kg IV q 2 hr – “Adjust as clinically indicated” n Cost (70 kg person) - $1 per µg – ~$5, 000/dose or $60, 000/day

Drugs and blood products used for bleeding

Treatment Approaches to the Bleeding Patient n n n n Red blood cells Platelet transfusions Fresh frozen plasma Cryoprecipitate Amicar DDAVP Recombinant Human factor VIIa

RBC transfusion therapy Indications n Improve oxygen carrying capacity of blood – Bleeding – Chronic anemia that is symptomatic – Peri-operative management

Red blood cell transfusions Special preparation CMV-negative patients Prevent CMV transmission Irradiated RBCs Immune deficient recipient or direct donor Prevent GVHD Leukopoor Previous non-hemolytic transfusion reaction CMV negative patients Prevents reaction PNH patients Ig. A deficient recipient Prevents hemolysis Prevents anaphylaxis Washed RBC Prevents transmission

Transfusion-transmitted disease Infectious agent Risk HIV Hepatitis C Hepatitis B Hepatitis A HTLV I/II CMV Bacteria Creutzfeld-Jakob disease Others 1/500, 000 1/600, 000 1/500, 000 <1/1, 000 1/640, 000 50% donors are sero-positive 1/250 in platelet transfusions Unknown
 – Pheresis platelets (Single donor)")
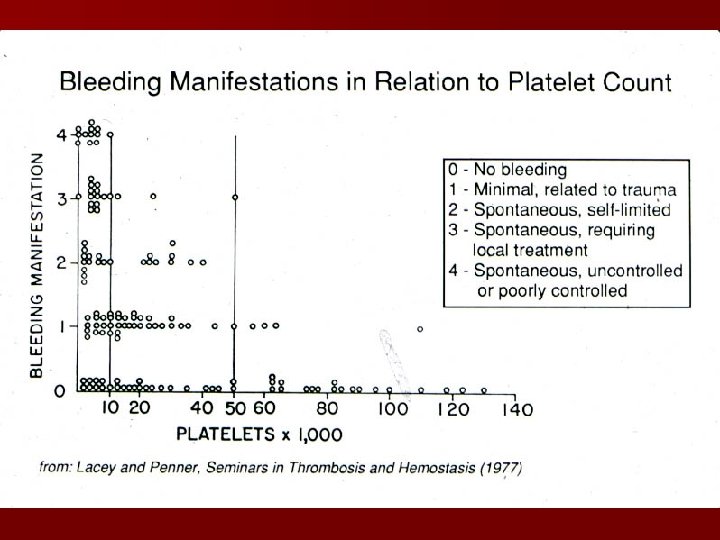
Platelet transfusions n Source – Platelet concentrate (Random donor) – Pheresis platelets (Single donor) n Target level – Bone marrow suppressed patient (>10 -20, 000/µl) – Bleeding/surgical patient (>50, 000/µl)
 n Indications n")
Fresh frozen plasma Content - plasma (decreased factor V and VIII) n Indications n – – n Multiple coagulation deficiencies (liver disease, trauma) DIC Warfarin reversal Coagulation deficiency (factor XI or VII) Dose (225 ml/unit) – 10 -15 ml/kg n Note – Viral screened product – ABO compatible

Cryoprecipitate Prepared from FFP n Content n – Factor VIII, von Willebrand factor, fibrinogen n Indications – – – n Fibrinogen deficiency Uremia von Willebrand disease Dose (1 unit = 1 bag) – 1 -2 units/10 kg body weight
 n Mechanism – Prevent activation plaminogen -> plasmin n")
Hemostatic drugs Aminocaproic acid (Amicar) n Mechanism – Prevent activation plaminogen -> plasmin n Dose – 50 mg/kg po or IV q 4 hr n Uses – – n Primary menorrhagia Oral bleeding Bleeding in patients with thrombocytopenia Blood loss during cardiac surgery Side effects – GI toxicity – Thrombi formation
 n Mechanism – Prevent activation plaminogen -> plasmin n")
Hemostatic drugs Aminocaproic acid (Amicar) n Mechanism – Prevent activation plaminogen -> plasmin n Dose – 50 mg/kg po or IV q 4 hr n Uses – – n Primary menorrhagia Oral bleeding Bleeding in patients with thrombocytopenia Blood loss during cardiac surgery Side effects – GI toxicity – Thrombi formation
 n Mechanism – Increased release of VWF from endothelium n")
Hemostatic drugs Desmopressin (DDAVP) n Mechanism – Increased release of VWF from endothelium n Dose – 0. 3µg/kg IV q 12 hrs – 150 mg intranasal q 12 hrs n Uses – Most patients with von Willebrand disease – Mild hemophilia A n Side effects – Facial flushing and headache – Water retention and hyponatremia

Overview 1. Clinical aspects of bleeding 2. Hematologic disorders causing bleeding Coagulation factor disorders Platelet disorders Approach to laboratory abnormalities Diagnosis and management of thrombocytopenia 3. 4. Approach to acquired bleeding disorders Hemostasis in liver disease Surgical patients Warfarin toxicity 5. Drugs and blood products used for bleeding

Clinical Features of Bleeding Disorders Platelet disorders Coagulation factor disorders Site of bleeding Skin Mucous membranes (epistaxis, gum, vaginal, GI tract) Deep in soft tissues (joints, muscles) Petechiae Yes No Ecchymoses (“bruises”) Small, superficial Large, deep Hemarthrosis / muscle bleeding Extremely rare Common Bleeding after cuts & scratches Yes No Bleeding after surgery or trauma Immediate, usually mild Delayed (1 -2 days), often severe

Pre-analytic errors n Problems with blue-top tube n – Hct ≥ 55 or ≤ 15 – Lipemia, hyperbilirubinemia, hemolysis – Partial fill tubes – Vacuum leak and citrate evaporation n Problems with phlebotomy – – – Heparin contamination Wrong label Slow fill Underfill Vigorous shaking Biological effects n Laboratory errors – Delay in testing – Prolonged incubation at 37°C – Freeze/thaw deterioration

Coagulation factor deficiencies Sex-linked recessive Factors VIII and IX deficiencies cause bleeding Prolonged PTT; PT normal Autosomal recessive (rare) Factors II, V, VII, X, XI Fibrinogen deficiencies cause bleeding Prolonged PT and/or PTT Factor XIII deficiency is associated with bleeding and impaired wound healing PT/ PTT normal; clot solubility abnormal Factor XII, prekallikrein, HMWK deficiencies do not cause bleeding
 thrombocytopenic purpura –")
Classification of platelet disorders n Associated with bleeding – Immune-mediated (Idiopathic) thrombocytopenic purpura – Most others

Classification of platelet disorders n Associated with thrombosis – Thrombotic thrombocytopenic purpura – Heparin-induced thrombocytopenia – Trousseau’s syndrome – DIC

Hemophilia A and B Coagulation factor deficiency Inheritance Incidence Severity Complications Hemophilia A Hemophilia B Factor VIII Factor IX X-linked recessive 1/10, 000 males 1/60, 000 males Related to factor level <1% - Severe - spontaneous bleeding 1 -5% - Moderate - bleeding with mild injury 5 -25% - Mild - bleeding with surgery or trauma Soft tissue bleeding

Treatment of hemophilia A n Intermediate purity plasma products – Virucidally treated – May contain von Willebrand factor n High purity (monoclonal) plasma products – Virucidally treated – No functional von Willebrand factor n Recombinant factor VIII – Virus free/No apparent risk – No functional von Willebrand factor
 – 10 -15% of severe hemophilia")
Complications of therapy n Formation of inhibitors (antibodies) – 10 -15% of severe hemophilia A patients – 1 -2% of severe hemophilia B patients n Viral infections – Hepatitis B – Hepatitis C – HIV Human parvovirus Hepatitis A Other

Features of Acute and Chronic ITP Features Acute Chronic Peak age Children (2 -6 yrs) Adults (20 -40 yrs) Female: male 1: 1 3: 1 Antecedent infection Common Rare Onset of symptoms Abrupt indolent Platelet count at presentation <20, 000 <50, 000 Duration 2 -6 weeks Long-term Spontaneous remission Common Uncommon
- Slides: 101