EVALUATION OF SYSTOLIC FUNCTION OF LEFT VENTRICLE BY

EVALUATION OF SYSTOLIC FUNCTION OF LEFT VENTRICLE BY ECHOCARDIOGRAPHY DR SANDEEP. R SR CARDIO

Basic Principle Systole The period of the cardiac cycle from the closure of the mitral valve to the closure of the aortic valve

EJECTION FRACTION • Ejection fraction-percentage of LV diastolic volume that is ejected with systole • EF=STROKE VOLUME/EDV=EDV-ESV/EDV NORMAL MILD LV DYSFUNCTION MODERATE LV DYSFUNCTION SEVERE LV DYSFUNCTION EF >55% 45 – 54% 30 – 44 % <30%

IDEAL METHOD FOR EF CALCULATION • Accurate • Quick • Reproducible • Simple • Relatively independent of LV geometry

M-Mode Quantification • Use Parasternal Short-Axis or Long. Axis views to measure LVEDD and LVESD • Measurement is taken perpendicular to the ventricle at the level of tip of mitral leaflet • Assumes that no significant regional wall motion abnormalities are present
 7, 79 108")
TECHNICAL ASPECTS Recommendations for chamber quantification*Eur J Echocardiography (2006) 7, 79 108

LV MEASUREMENT - TTE 1. PLAX 2. PSAX AT PAPILARY MUSCLE
 2 D METHOD • Useful for assessing patients with CAD")
LV MEASUREMENT -TTE 3) 2 D METHOD • Useful for assessing patients with CAD • LV internal dimensions (LVIDd and LVIDs & wall thicknesses be measured at mitral chordae level • 2 D minor-axis dimensions smaller than M-mode measurements Recommendations for chamber quantification*Eur J Echocardiography (2006) 7, 79 108
 ME-LAX b)TG-LAX c) TG –SAX preferred view Recommendations for")
LV MEASUREMENTS - TEE a) ME-LAX b)TG-LAX c) TG –SAX preferred view Recommendations for chamber quantification*Eur J Echocardiography (2006) 7, 79 108
 7, 79 108")
LV MEASUREMENTS Recommendations for chamber quantification*Eur J Echocardiography (2006) 7, 79 108
 7, 79 108")
LV MEASUREMENTS Recommendations for chamber quantification*Eur J Echocardiography (2006) 7, 79 108
 – Assumes symmetric contraction • Ejection fraction")
Global Myocardial Function • Fractional shortening (FS) – Assumes symmetric contraction • Ejection fraction (EF) EF=EDV-ESV/EDV

EJECTION FRACTION

TEICHOLZ /CUBED FORMULA • LV Volume calculation is based on assumption that the LV is a prolate ellipse LV VOLUME= 4/3 x. Pi x D 1/2 x 2 D 1/2 = Pi/3 x D cube =1. 047 x D cube = D cube This structure has two minor axis D 1 & D 2 and a major axis L V=4/3 Pi X D 1/2 X D 2/2 X L/2 • Basic assumptions – LV dilates along the minor axis – LV internal diameter is equal to one of the minor axis of the ellipse D 1 – Both minor axisof ellipse D 1, D 2 are equal

TEICHOLZ

MODIFIED TECHOLZ • As LV becomes more spherical as it dilates the relation between major and minor axis changes. • Therefore a regression formula was devised to correct for this change in shape • LVV=( 7. 0/2. 4+D) x Dcube

MODIFIED QUINONES METHOD • Measure LVIDd &LVIDs • Calculate radial EF • If significant RWMA average EF measurement from basal & mid LV levels • Add factor for longitudinal shortening

SIMPSON’S METHOD • In the presence of RWMA all the above methods will be less accurate, since inclusion of RWMA- causes volume overestimation • The apical biplane methods are more robust in this setting, using summation of a series of disks from apex to base (often called Simpson’s Rule). • The ASE (American Society of Echocardiography) recommends use of biplane apical views with a modified Simpson’s rule approach

SIMPSON’S METHOD

BIPLANE SIMPSONS

Simpson’s method

Simpson’s Rule – the biplane method of disks LV-ED LV-ES • Volume left ventricle - manual tracings in systole and diastole - area divided into series of disks LV-ED LV-ES A 4 C - volume of each disc(πr 2 x h ) summed = ventricular volume • Preferred method of choice A 2 C

SIMPSONS RULE RULE OF DISC

AREA - LENGTH METHOD Hemi-cylindrical Hemi-ellipsoid Model Assumes: Base of ventricle = cylinder Apex of ventricle = ellipsoid Volume is calculated using a long axis length L and crosssectional area Am of an orthogonal short-axis view at the midpapillary muscle. V = (Am) VOLUME=5 (Area )(length)/6 L/2 + 2/3 (Am) L/2 V = 5/6 AL (Bullet Formula)

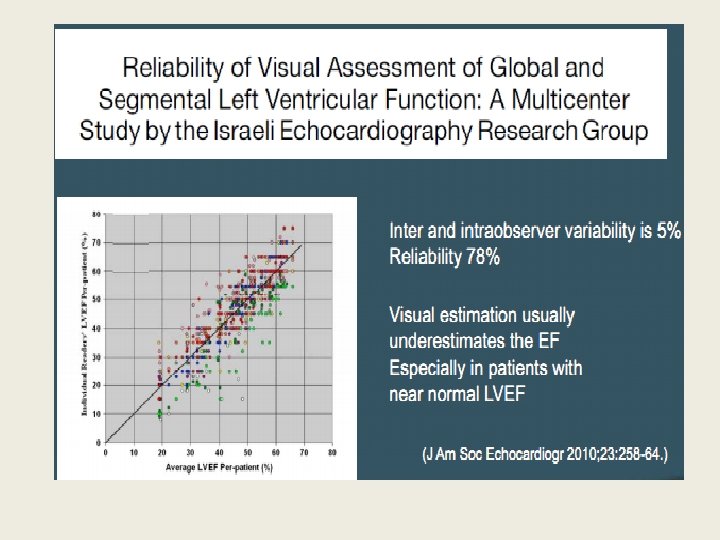
VISUAL EF Echocardiographic assessment of global left ventricular systolic function is usually performed subjectively • • Experienced echocardiographers - estimate EF by looking at the overall size and contractility as well as the inward movement and thickening of the various segments of the LV walls without actually taking measurements Correlate fairly well with angiographic assessment of the EF Limitations: Irregular rhythm Very large or very small LV Extremes of heart rate

LV QUANTIFICATION METHODS

COMPARISION OF VARIOUS ECHO METHODS WITH CINE ANGIO & RADIONUCLIDE VENTRICULOGRAPHY ESV & EDV CORRELATION EF CORRELATION • Modified simpson’s rule showed maximum correlation with cine angio & RVG

LV MASS ASSESMENT

Evaluation of LV Mass This is done by tracing the epicardial to calculate the total ventricular volume and the endocardial border to calculate chamber volume. LV mass = 1. 05 (total volume – chamber volume)

LV Total Area LV Cavitary Area Length

Evaluation of LV Mass Total volume= Total area x length Chamber volume = Chamber area x Length Myocardial volume = Total volume – Chamber volume LV mass = Myocardial volume x density LV mass = Myocardial volume x 1. 05

Evaluation of LV Mass

LV MASS

LV Mass Quantification • 2 D M-Mode method using parasternal short axis view or parasternal long axis view • Assumes that LV is ellipsoid (2: 1 long/short axis ratio) • Measurements made at end diastole • ASE approved cube formula: • LV mass (g) = 1. 04 [(LVID + PWT + IVST)3 - (LVID)3] X 0. 8 + 0. 6 LV mass index (g/m 2) = LV mass / BSA • Small errors in M-Mode cause large errors in mass values. Can have off axis/tangential cuts due to motion.

LV MASS ASSESMENT

LV MASS-TEE • TEE evaluation of LV mass highly accurate, but has minor systematic differences in LV PWT • LV mass derived from TEE wall-thickness measurements is higher by an average of 6 g/m 2.

LV MASS RELATIVE WALL thickness= 2 XPW/LVIDd

OTHER M-Mode METHODS OF LV FUNCTION ASSESMENT

EPSS NORMAL ≤ 6 mm EF<50% >7 mm EF≤ 35% ≥ 13 mm SENSITIVITY SPECIFICITY 87% 75% 87% 84% LIMITATIONS-INACCURATE 1) AR 2) MS 3) IWMI Lew W et al , American journal of cardiology 41: 836 -845, 1978 Ahmadpour, H et al , American heart journal 106: 21 -28, 1983:

B- notch • Delayed closure of mitral leaflets between the A and C (leaflet coaptation) points, determining a "notch" known as B-bump (small arrows) • Indicates increased left ventricular end-diastolic pressure ( > 20 mmhg) • LIMITATIONS • 1) Low sensitivity • 2)false positive with first degree AV block & LBBB-due to prolonged AC interval Ambrose J A et al Circulation 60: 510 -519 1979

MITRAL ANNULAR PLANE EXCURSION • M-mode tracings in systole • The magnitude of systolic motion is proportional to the longitudinal shortening of the LV • Normal mitral annular systolic motion is > 8 mm (average 12 +/- 2 on apical 4 or apical 2 views) • If motion is < 8 mm, the EF is likely < 50% • If <8 mm -98% sensitive & 82% specific for EF <50%

GRADUAL CLOSURE OF AORTIC VALVE Decreased LV forward flow causes gradual reduction in forward flow in late systole This results in rounded appearance of aortic valve closure in late systole

DOPPLER EVALUVATION OF GLOBAL LVF

Doppler Stroke Volume Calculation CARDIAC OUTPUT= STROKE VOLUME X HEART RATE

Doppler Stroke Volume Calculation Assumption used for measuring SV using Doppler are: 1. Accurate cross-sectional flow area measurement. 2. Laminar Flow. 3. Parallel intercept angle between Doppler beam and direction of blood flow. 4. Velocity and diameter measurements are made at the same anatomic site.

SITE CSA MEASUREMENT VTI MEASUREMENT ECHO VIEW PW SAMPLE VOLUME POSN. Ascending aorta ECHO VIEW PHASE PLAX ( at or above ST jn. ) Early systole Suprasternal view Ascending aorta at 3. 5 cm toward ascending aorta Aortic annulus PLAX Early systole Apical 4 /5 -C LVOT (just below aortic valve) Mitral inflow Apical 4 -C Mid diastole Apical 4 -C Mitral annulus Tricuspid inflow Apical 4 -C Mid diastole Apical 4 -C Tricuspid annulus Pulmonary annulus PLAX (Rvot) PSAX( RVOT) Early systole PLAX(RVOT) PSAX(RVOT) RVOT (Prox. To Pulm. Valve) Pulmonary artery PLAX(RVOT) PSAX(RVOT) Early systole PLAX(RVOT) PSAX(RVOT) Distal to Pulm. Valve ( same level as diameter measurement)

DOPPLER EVALUATION OF LV FUNCTION

Problems in this technique 1. Apical 3 -chamber view can be tried if Apical 5 -c is difficult to obtain of velocities. 2. Underestimation of flow velocities- LVOT may not be aligned with the direction of the PWD an apical 3 -chamber view may sometimes offer better alignment. 3. When the parasternal long axis view is not obtainable, a LVOT diameter of 2 cms for males and 1. 75 cms for females can be assumed. 4. Variations in VTI with respiration Movement of entire cardia with respiration –difficult to obtain uniform velocities with PWD at LVOT

Pitfalls in Echo Calculation of CO • Accurate measurement of CSA – Weakest link in the calculation – VTI very good for assessing change in cardiac output with therapy, by following changes in VTI, since CSA is largely invariant in an individual • Measures forward flow only – Regurgitant fraction not considered – May over-estimate systemic cardiac output • Echocardiographic window in mechanically ventilated patients may be poor

Myocardial Performance Index • Applied to either the left or right ventricle. • Ejection time (ET), isovolumic contraction time (IVCT) and the isovolumic relaxation time (IVRT). • MPI = ( IVCT + IVRT ) / ET Systolic dysfunction is associated with a prolongation of IVCT and a shortening of the ET Normal range is 0. 39 ± 0. 05, and values > 0. 50 are considered abnormal
 • When Mitral regurgitation is present the CW")
RATE OF VENTRICULAR PRESSURE RISE (dp/dt) • When Mitral regurgitation is present the CW Doppler velocity curve indicates the instantaneous pressure difference between the left ventricle and left atrium • The slope of the MR jet velocity can be quantitated as the rate of change in pressure over time (d. P/dt) by measuring the time interval between the MR jet velocity at 1 and 3 m/s

DP/DT-Lv function assesment dt 1 m/s, 4 mm. Hg d. P 3 m/s, 36 mm. Hg

Evaluation of LV Systolic Function At each velocity, the corresponding pressure gradient is 4 v squared per Bernoulli. d. P/dt = [ 4 (3) – 4 (1)] = 32 mm. Hg Time interval Thus a longer time interval indicates a depressed d. P/dt and thus a decreased LV systolic function.

CW doppler to measure rate of rise of MR jet may correlate to LVEF A slow rate of rise may indicate poor systolic function Must have MR present, and good doppler study present (more difficult with eccentric jets)

Limitations: This method is only useful in patients with enough MR to obtain a well-defined velocity curve. LA should be compliant. Click artifact (caused by valve closure) can obscure the descending limb of the CWD envelope, which makes measurements difficult. Eccentric MR jets may not reflect true velocity and will result in underestimation of dp/dt unless careful colour Doppler examination of the jet is made to minimize CWD error. A normal dp/dt maybe present in hypertension and aortic stenosis even with impaired LV function.

Evaluation of LV Systolic Function The other Doppler measurements that can be used to measure LV systole function are 1. Peak velocity 2. Mean acceleration 3. Acceleration Time 4. Deceleration Time 5. Ejection time 6. Mean deceleration

Evaluation of LV Systolic Function Ejection Time Acceleration Time Mean Acceleration Peak velocity Deceleration Time
 <0. 35 24% 100% EF<55% >0.")
SYSTOLIC TIME INTERVALS LVPEP/LVET SENSITIVITY SPECIFICITY NORMAL (EF>55%) <0. 35 24% 100% EF<55% >0. 35 100% 72% EF<30% >0. 65 89% LVPre ejection period(LVPEP)- measured from Q wave on ECG to onset of aortic valve opening LV Ejection time(LVET)- aortic valve opening to aortic valve closure LVPEP/LVET independent of Heart Rate Lv dysfunction causes increase in LVPEP & shortening of LVET 1)Weissler, A. M et al Systolic time intervals in heart failure in man Circulation 37: 149 -159, 196 2)Garrard et al , circulation 42 : 455 -462, 1970

REGIONAL LV FUNCTION

REGIONAL LV FUNCTION

REGIONAL LV FUNCTION

REGIONAL LV FUNCTION

NONISCHEMIC RWMA

DIFF ISCHEMIC VS NONISCHEMIC

LBBB

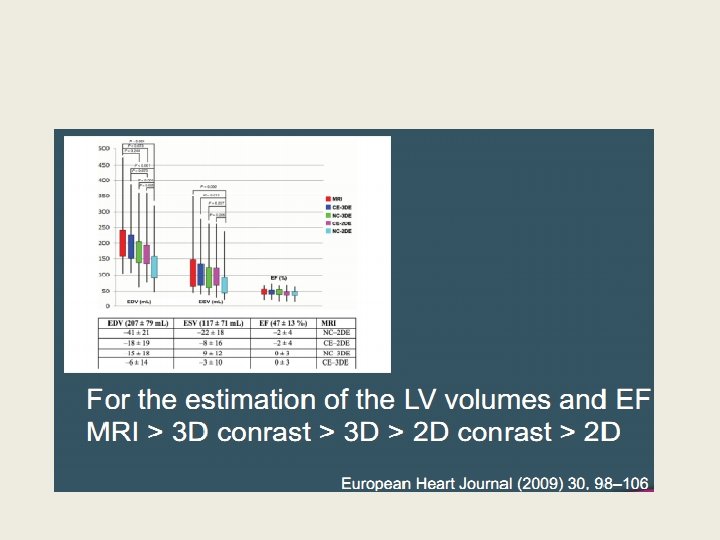
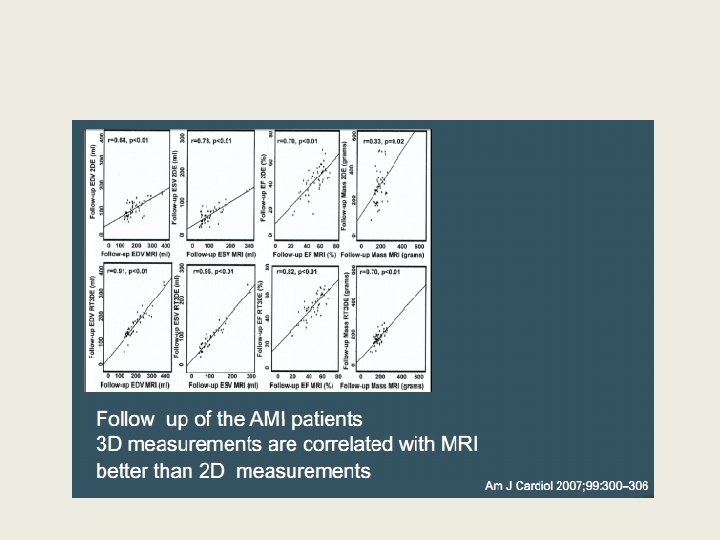
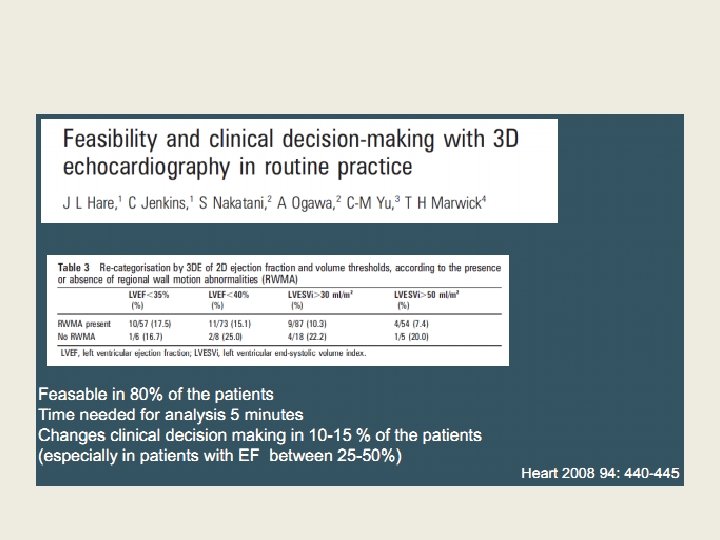
3 D ECHO • Provides detailed anatomic relationship • Accurate quantitation • Faster acquisition and may reduce interobserver variability • 3 d quantitation of LV function avoids geometric assumptions and is more accurate & reproducible

3 D echo

TISSUE DOPPLER IMAGING • The annular velocity in systole has shown a good correlation with the LVEF • Can detect impaired longitudinal systolic function (Sm < 4. 4 m/s) • SEPTAL ANNULAR TDI

NEWER METHODS OF EVALUATION OF LV FUNCTION

STRAIN RATE IMAGING & SPECKLE TRACKING

COLOUR KINESIS

CENTRAL LINE METHOD

THANK YOU

BIBILOGRAPHY LANGE ET AL; Recommendations for Chamber Quantification: A Report from the American Society of Echocardiography’s Guidelines and Standards Committee and the Chamber Quantification Writing Group, Developed in Conjunction with the European Association of Echocardiography, a Branch of the European Society of Cardiology; J Am Soc Echocardiogr 2005; 18: 1440 -1463 • Assessmentof. Left Ventricular Systolic Function by Echocardiography. CARDIOLOGY CLINICS • Reliability of reporting left ventricular systolic function by echocardiography: A systematic review of 3 methods. American Heart Journal Volume 146, Number 3 • Techniques for comprehensive two dimensional echocardiographic assessment of left ventricular systolic function • TEXTBOOK OF CLINICAL ECHOCARDIOGRAPHY FIFTH EDITION •

MCQ • 1. WHICH IS THE METHOD RECOMMENDED BY American Society of Echocardiography For EF ESTIMATION? • 1) TECHOLZ • 2) QUINONES • 3) AREA LENGTH • 4) SIMPSON’S BIPLANE • ans 4

• 2. Pt. presumed to have a EF < 35% if the EPSS is 1)4 2) 8 3)15 4)10 Ans 3
 TEICHOLZ •")
3. Preferred choice for Ef estimation in patients with RWMA • 1) TEICHOLZ • 2) QUINONES • 3) SIMPSONS • 4) AREA LENGTH • Ans 3
 5 • 2)8")
4. MITRAL ANNULAR PLANE EXCURSION SUGGESTIVE OF LV DYSFUNCTION • 1) 5 • 2)8 • 3)10 • 4)12 • Ans 1
 1 • b)2 •")
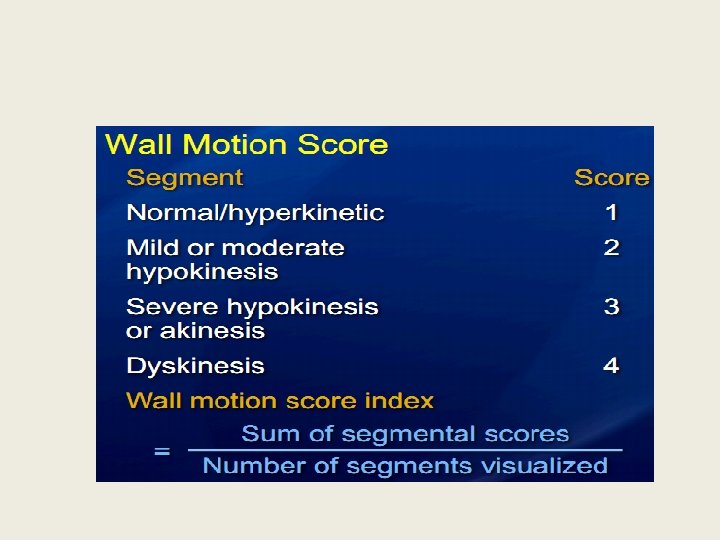
5. WHAT IS WALL MOTION SCORE FOR DYSKINESIS • a) 1 • b)2 • c)3 • d)4 • Ans D
2 • B)4 •")
6. What is the normal wall motion score index? • a)2 • B)4 • C)1 • D)3 • Ans c
 QUINONES •")
8. Which method is known as the D cube method • 1) QUINONES • 2) SIMPSONS • 3) AREA LENGTH METHOD • 4) TEICHOLZ • Ans 4
 MILD LV")
9. DP/DT OF MR JET IS 1400 THE PT HAS • 1) MILD LV DYSFN. • 2) SEVERE LV DYSFUNCTION • 3) NORMAL LV FUNCTION • 4) MODERATE LV DYSFUNCTION • ans 3

10. IF RWT >0. 42 AND LV MASS IS NORMAL, THE PATIENT HAS • 1) CONC LVH • 2) CONSCENTRIC REMODELLING • 3) ECCENTRIC LVH • 4)NORMAL • Ans 2
 Anterior wall myocardial infarction")
11. All of the following can cause RWMA except 1) Anterior wall myocardial infarction 2) LBBB 3) Preexcitation (WPW syndrome) 4) Acute Pericarditis Ans 4
 EPSS >")
12 All of these indirectly denote LV dysfunction EXCEPT ? • A) EPSS > 15 • B) MAPSE < 8 • C) DP/dt< 800 • D) Myocardial performance index < 0. 5 • Ans d
Cardiac index 2) Myocardial performance index 3)")
13. Which is known as TEI index? 1)Cardiac index 2) Myocardial performance index 3) LV preejection time/ LV ejection time 4)DP/DT of MR jet Ans 2
 RCA • B)")
14. Inferolateral segment is supplied by which arterial territory • A) RCA • B) LAD • C) RAMUS • D) LCX • Ans d
 LV dysfunction causes shortening of ejection")
15. Which is the true statement • A) LV dysfunction causes shortening of ejection time • B) LV dysfunction causes shortening of preejection period • C) LV dysfunction causes Lvpreejection period/LV ejection period < 0. 35 • D) LV dysfunction causes prolongation of ejection time and shortening of preejection period • Ans a

16. If the MR velocity is 1 m/s at 1 sec and if it accelerates to 4 m/s at 4 sec then what is the DP /dt? 1) 10 2) 15 3) 20 4) 25 Ans 3

• 17. If the relative wall thickness is 0. 39 and LV mass increased then the patient has • 1) conc. LVH • 2) NORMAL • 3) ECCENTRIC LVH • 4) CONSCENTRIC REMODELLING • Ans 3

• 18. In which formula for LV function assesment is the assumption of prolate ellipse considered • 1) QUINONE’S • 2) TEICHOLZ • 3) AREA LENGTH • 4) SIMPSON’S • Ans
 presence of B notch")
• • • 19. identify the false statement 1) presence of B notch denotes LV dysfunction 2) EPSS is not accurate if patient has AR 3) EPSS > 15 denotes severe LV dysfunction 4) MPI < 0. 5 denotes LV dysfunction • Ans 4

• 20. In which method of LV function assesment is the apical contraction considered for EF calculation? • 1) TEICHOLZ • 2) MODIFIED QUINONES • 3) SIMPSONS • 4) AREA LENGTH • Ans 2

• 21. A patient is found to have a calculated EF of 42%. He is said to have 1) Normal LV fn. 2) Mild LV dysfunction 3) Moderate LV dysfunction 4) Severe LV dysfunction Ans 3
 Dilated cardiomyopathy")
• • • 22. EPSS on echo is increased in A) Dilated cardiomyopathy B) Hypertrophic cardiomyopathy C) Aortic stenosis D) Pulmonary stenosis • Ans a
 Assesing")
• 23. Transthoracic echo is superior to transesophageal echo in • A) Assesing prosthetic valve function • B) Assess LA clot • C) Diagnosisof infective endocarditis • D) Assesment of LV systolic function • Ans: D
")
• 24. Assumption of LV used in calculation of simpsons formula • 1) Prolate ellipse • 2) Cone • 3) Circle • 4) Disc • Ans 4)
 onset of P wave")
• • • 25. LVEDD is measured at 1) onset of P wave 2) R wave 3) peak of T wave 4) U wave • Ans 2)
 Q wave 2)")
• • • 26. LVESD measurement is done during 1) Q wave 2) R wave 3)T wave 4) U wave • Ans 3
 increase of systolic wall")
27. Akinesis of a segment is defined • 1) increase of systolic wall thickness < 10% • 2) Increase in systolic wall thickness >50 % • 3)increase in systolic wall thickness <40% • 4) outward movement of wall during systole with associated systolic wall thinning • Ans 1
1 B) 2 C)")
• • • 28. Wallmotion score for akinesis is A)1 B) 2 C) 3 D)4 E)5 • Ans C
 increase of systolic wall")
• • • 29. Hypokinesia is defined as 1) increase of systolic wall thickness < 10% 2) Increase in systolic wall thickness >50 % 3)increase in systolic wall thickness <40% 4) outward movement of wall during systole with associated systolic wall thinning • Ans 3
 30 -50 2) 50 –")
• • • Normal stroke volume is 1) 30 -50 2) 50 – 70 3) 70 – 90 4)>100 • Ans 3
- Slides: 109