Evaluation of syncope DR HICHAM AL MAWLA EMJ





















 • Unmasks VVS susceptibility • Reproduces symptoms • Patient learns")
 DG Benditt, UM Cardiac Arrhythmia Center")



















- Slides: 70
Evaluation of syncope DR HICHAM AL MAWLA EMJ LEBANON
Syncope Definition • Collapse, Blackout • A sudden, transient loss of consciousness and postural tone, with spontaneous recovery
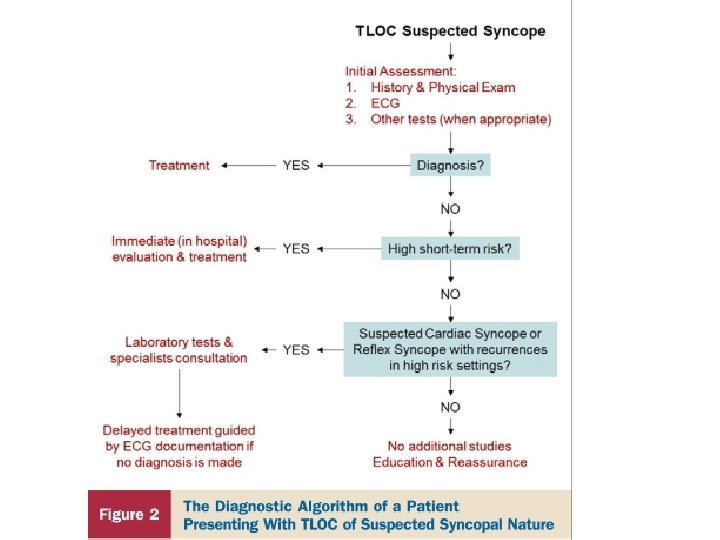
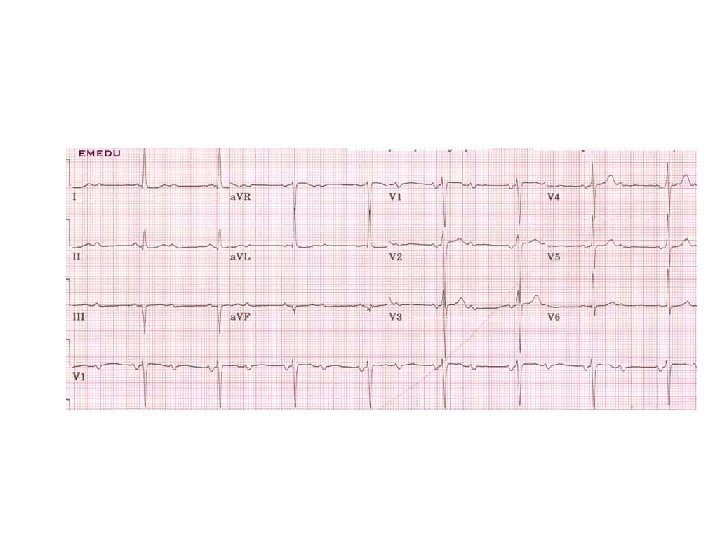
Initial Evaluation 12 leads ECG
The ECG • Up to 50% of patients with syncope have abnormal EKG • Only 2 -10% will have diagnostic abnormality
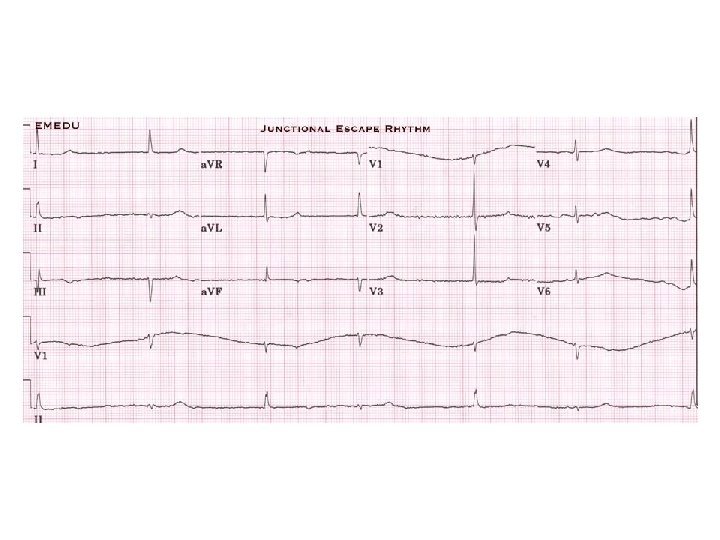
Syncope: Torsades From the files of DG Benditt, UM Cardiac Arrhythmia Center
Sinus Arrest
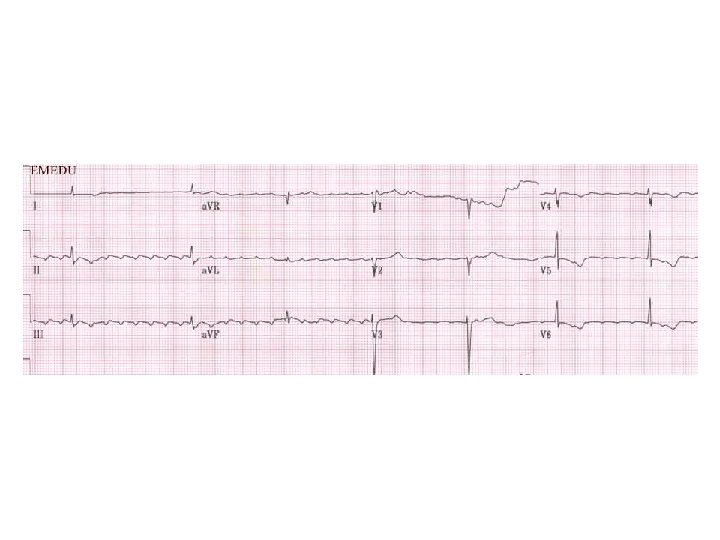
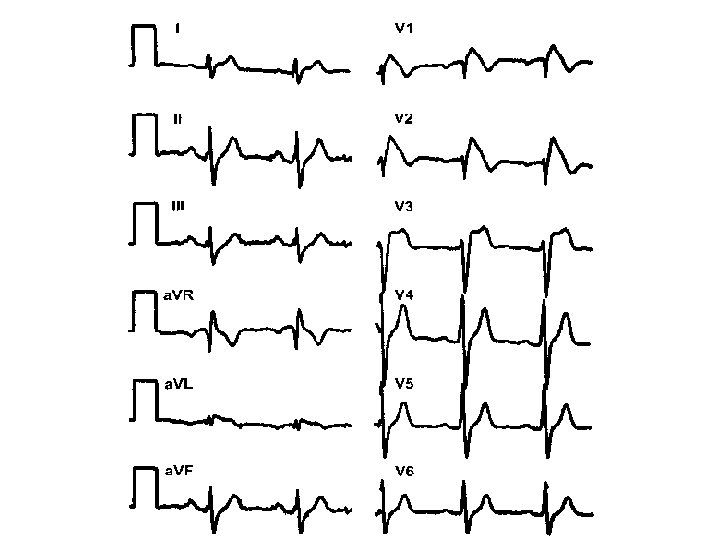
n Epsilon wave
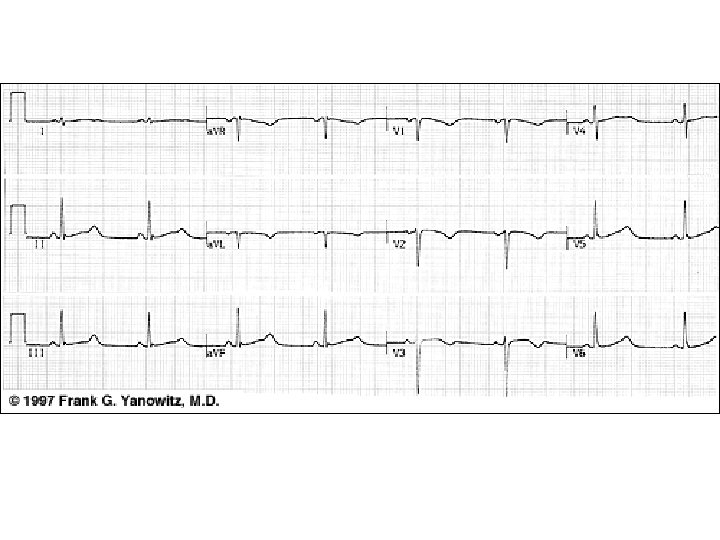
Arrhythmogenic right ventricular dysplasia Deep T wave inversions in V 2 to V 4, compatible with right ventricular disease, and epsilon waves just after the QRS complex (arrows).
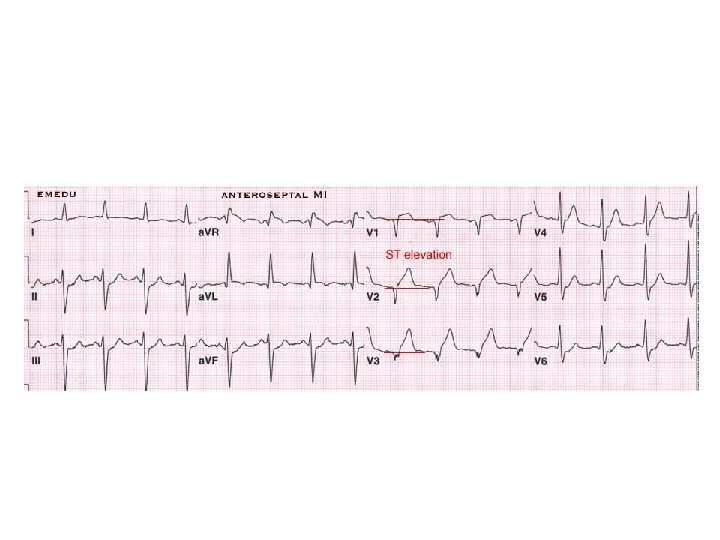
Reasons for hospital admission… • Acute myocardial infarction, pulmonary embolism, • Other cardiac diseases diagnosed as causing syncope – – Known coronary artery disease, CHF Valvular or congenital heart disease History of ventricular arrhythmias • Symptoms suggestive of arrhythmias or ischemia • Associated with palpitations • Chest pain suggestive of coronary disease • Exertional syncope • Physical findings of heart disease (e. g. , findings of aortic stenosis)
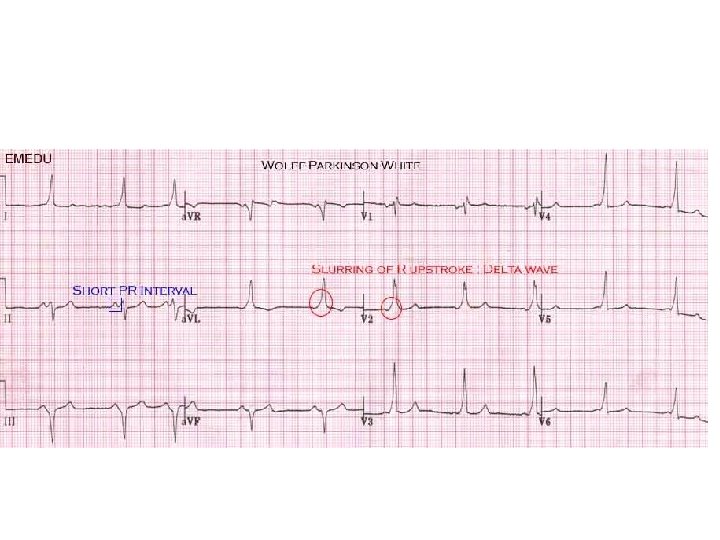
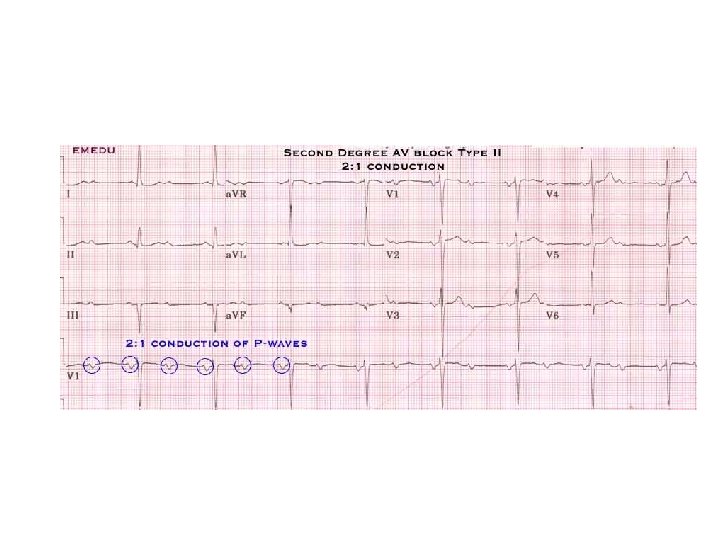
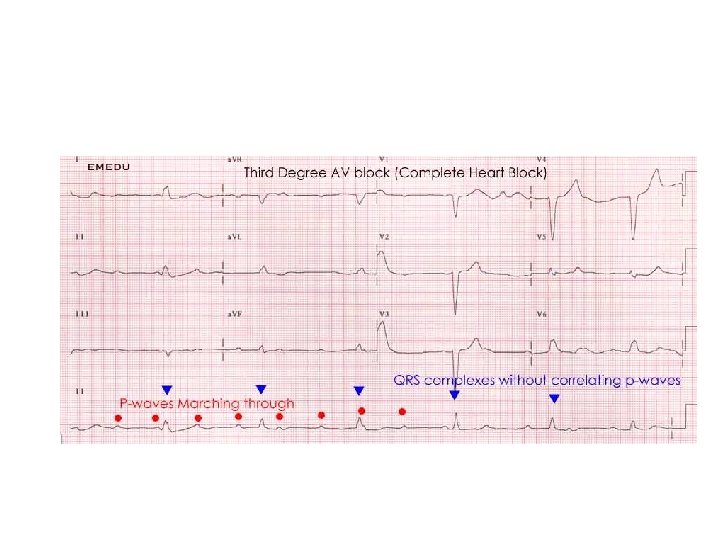
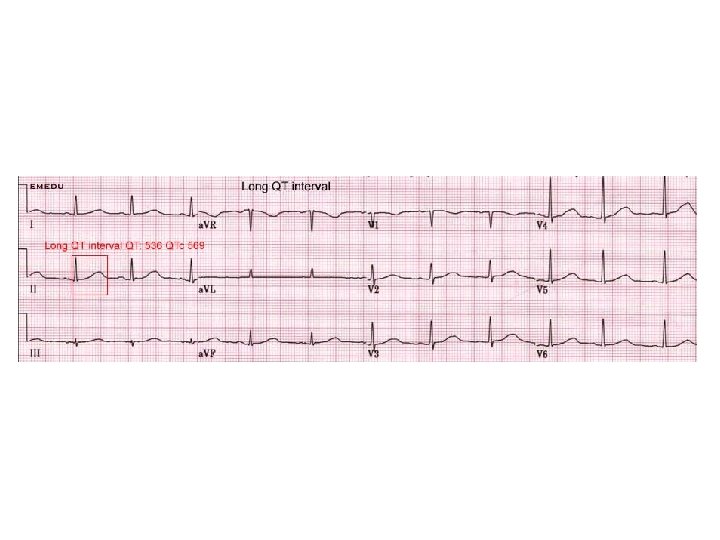
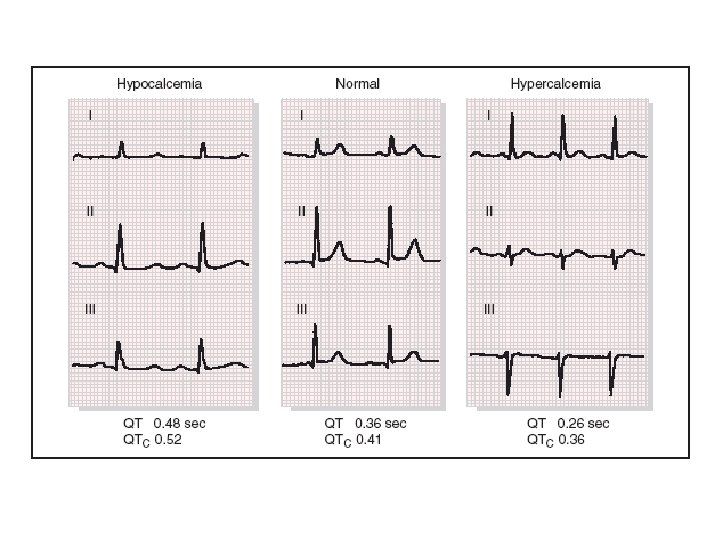
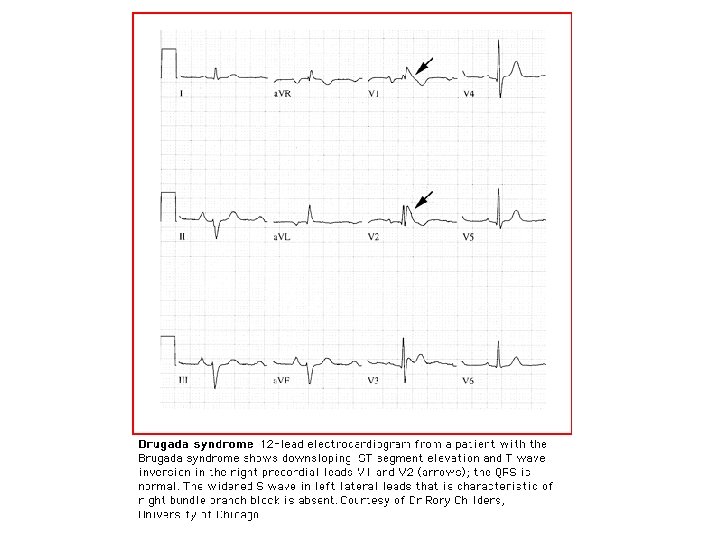
Reasons for hospital admission…. . • Electrocardiographic abnormalities – Prolonged corrected QT interval – Right bundle branch block with ST elevation in V 1 -V 3 Brugada pattern – Epsilon waves (arrhythmogenic right ventricular dysplasia) – Preexcitation syndrome (Wolff Parkinson White) – Short corrected QT interval ( 0. 30 sec) – Conduction delay or atrioventricular block – Signs of myocardial injury – Non sinus rhythm – Ventricular hypertrophy or strain patterns – Unsustained ventricular or supraventricular tachycardia – Pacemaker malfunction
Reasons for hospital admission • Acute severe volume loss (e. g. , dehydration, gastrointestinal bleeding) • Orthostatic hypotension • Moderate to severe chronic orthostatic hypotension • Treatment of multiple coexisting abnormalities • Discontinuation or dose modification of offending drug • Drugs causing torsades de pointes and long QT • Drug reaction such as anaphylaxis, orthostasis, bradyarrhythmias
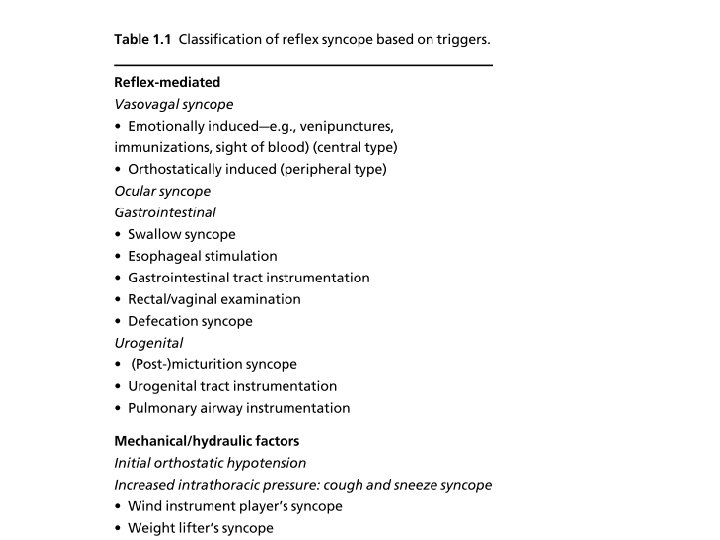
Case • A 14 -year-old boy was referred analysis of an unexplained episode of transient loss of consciousness. • History-taking revealed two episodes of transient loss of consciousness • One occurred while he had been standing still on a warm day during a vacation with his parents in Paris while a street artist was making a drawing of him. • The other episode occurred when he was standing motionless while a friend of his mother was giving him a haircut. • During these episodes, he was reported to be pale and sweating. Nausea was present during one of the episodes.
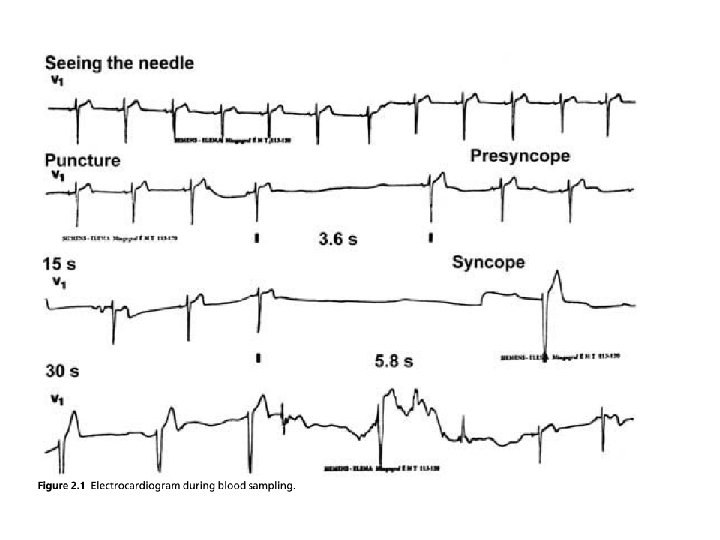
Case • A 27 -year-old man attended the outpatient clinic due to a history of recurrent episodes of syncope and pre syncope since the age of 7. • All of the episodes had been triggered by seeing blood or by being given an injection. • The patient had a normal physical examination and a normal electrocardiogram (ECG). • The patient’s ECG was monitored continuously while venous blood was being taken while he was in the recumbent position. • A syncopal episode developed during the blood sampling, and the sequence of electrocardiographic events was as follows
Mechanism Blood pools in venous capacitance vessels Reduced venous return and cardiac output Baroreceptor mediated increased sympathetic activity>>>>>> Mild increase in BP and HR Paradoxical stimulation of ventricular mechanoreceptors(Usually stimulated by vigorous contraction)
Mechanism Afferent pathways activated via Vagal C fibres Vasomotor center stimulated Stimulation of parasympathetic actvity Withdrawl of sympathetic activity BP and HR fall Reduced cerebral perfusion - syncope
Case • A 28 -year-old male firefighter in excellent general condition lost consciousness transiently after completing a routine checkup exercise test [1]. • The episode occurred while he was sitting motionless on the bicycle ergometer after the test and his skinfold thickness was being measured.
syncope occurring after exercise • The majority of cases fall into two related categories: – firstly, an exaggerated form of the normal postexercise hypotension response; and – secondly, neurally mediated syncope (i. e. , vasovagal reactions). – It is probable that the former triggers the latter
Case • A 62 -year-old woman presented with a fall resulting in a head wound. • On the day of the fall, she was up early and was having breakfast standing in the kitchen. The next thing she could remember was that she was on the floor bleeding from a head wound. • She knew where she was and was able to stand up easily. However, in the standing position she passed out again. • On regaining consciousness, she contacted her general practitioner and was transported by ambulance to the hospital. • ER/hospital – No obvious explanation for the loss of consciousness could be found. – PE and ECG were normal – Echocardiography, a 24 -h Holter monitoring and stress test were normal. – EEG showed irregularities over the temporal lobe. Phenytoin was started.
Case • Previous recurrent fainting: Hx of repeated • Tilt table test positive>>>>vasovagal syncope
Tilt testing
Tilt testing • Upright posture leads to pooling of blood in legs resulting in decreased venous return • Normal compensatory response to standing up-right is reflex tachycardia, more forceful contraction of the ventricles, and vasoconstriction • In individuals susceptible to vasovagal syncope, this forceful ventricular contraction in the setting of a relatively empty ventricle may excessively stimulate the cardiac sensory nerves (mechanoreceptors) • Afferent impulses are relayed to the medulla, resulting in a decrease in sympathetic and increase in parasympathetic tone
Head-up Tilt Test (HUT) • Unmasks VVS susceptibility • Reproduces symptoms • Patient learns VVS warning symptoms • Physician is better able to give prognostic / treatment advice
Head-Up Tilt Test (HUT) DG Benditt, UM Cardiac Arrhythmia Center
Case • • • A 35 -year-old otherwise healthy engineer was referred to the syncope unit for analysis of an episode of loss of consciousness, which had occurred during a return flight from a week-long holiday in Turkey. Before boarding the airplane at midnight, the patient felt tired and was continuously yawning without any other specific complaints. Once seated in the aircraft, he fell asleep almost immediately. After approximately 30 min of sleep, he retrieved an item from the over-head compartment without problems and quickly fell asleep again. About 1 h later, he woke up feeling weak and extremely thirsty, and decided to have a soft drink. The patient’s partner, a cardiology resident, was woken by the sound of the drink can falling to the floor. She saw a tonic posture with the arms extended and the head and neck held backwards. The posture resembled the one people assume during stretching. After this, his arms jerked for about a minute, and he then became completely flaccid. His pulse was very slow and weak and he was breathing superficially. Before he could be transferred from his chair to the aisle, he regained consciousness.
Pattern of convulsion Uncoordinated myoclonic jerks & twitches after LOC. GTC movementscoincidence with LOC Forced conjugate deviation of eyes Absent Common
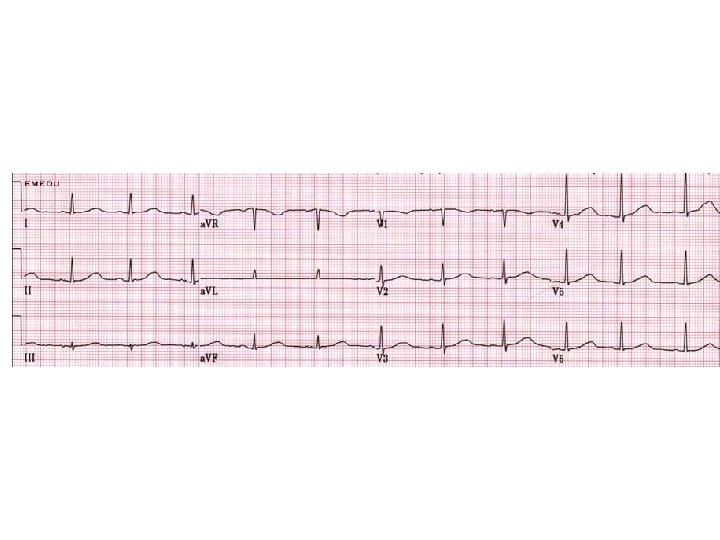
Case I • A 23 -year-old male with no known medical history suddenly collapsed while playing a vigorous game. His friends immediately started CPR and called 911. The paramedics arrived within 5 minutes and found him in VF. • He was defibrillated successfully with one shock with return of spontaneous circulation. • He was transported to the hospital for subsequent care. The following ECG was obtained upon arrival to the hospital:
Case I
What is the most likely diagnosis? a. Short QT syndrome b. Long QT syndrome c. Brugada syndrome d. Catecholaminergic polymorphic VT
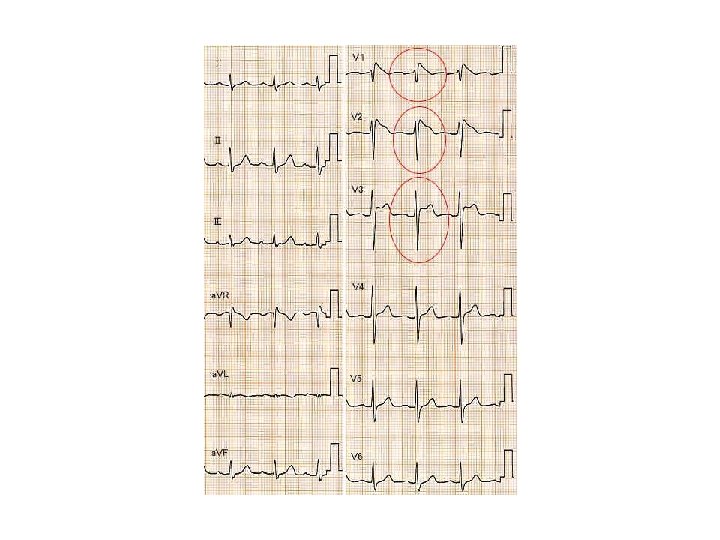
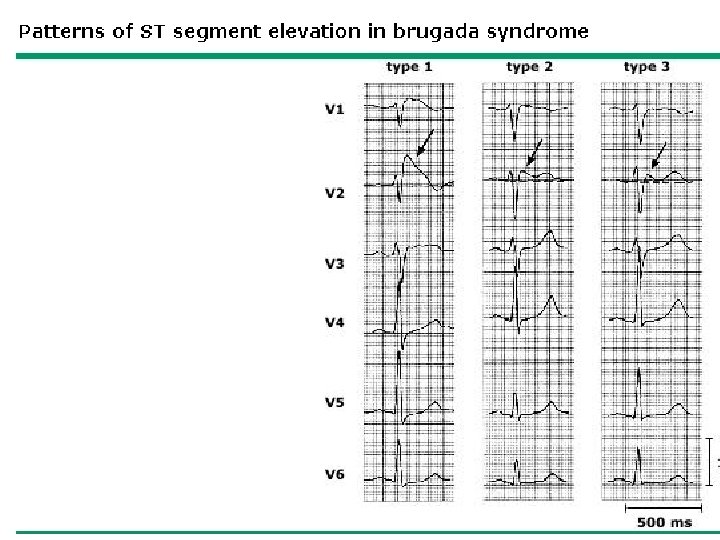
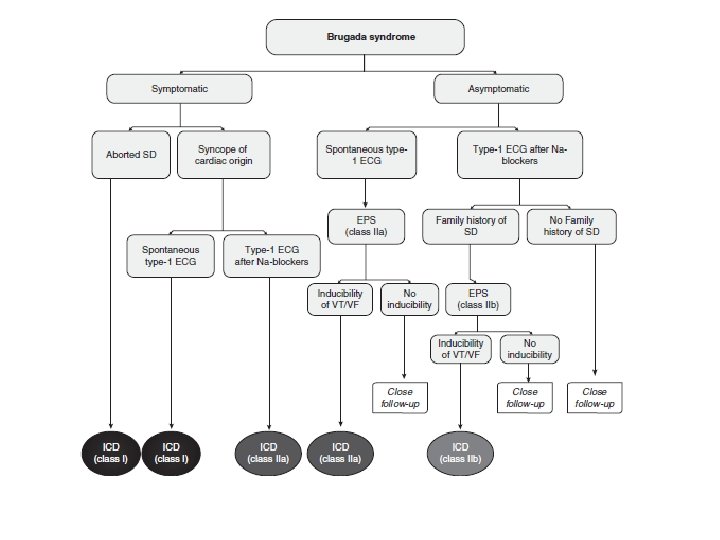
Type I- is diagnostic when combined with the right clinical picture. • V 1 -V 3 (as least two leads) ST segment elevation >2 mm, “coved” shape, inverted Twave. • Coupled with – Documented VFib – Polymorphic VT – FH of sudden cardiac death <45 yo – Type I EKG in family members – VT inducable in EP lab – Syncope – Nocturnal agonal respiration
Types II and III- Suggestive • Types II and III • raise suspicion for Brugada • only diagnostic if they can be converted to Type I during challenge with a sodium channel blocker.
Brugada Type I: coved ST segment in V 1 -V 3, >2 mm elevation, inverted T wave.
BRUGADA SYNDROME PROGNOSIS • Prevalence – Japan: 1%. – USA: 0. 4% • High mortality rate. 10% /yr • Sudden cardiac arrest often the first symptom. – More common at night, esp when sleeping. • Mean age of sudden death 41 +/- 15 years. • Prior History of SCA: 70% recurrence within 5 years. • Syncope. 6 fold higher risk of SCD.
BRUGADA SYNDROME • A sodium channel abnormality>>>> sudden cardiac death. • Autosomal dominant trait. 50% of cases are familial. • 20 -30% of cases have abnormal SCN 5 A gene. • Male/female : 8: 1 • ECG: – Type III
Case II • A 16 -year-old female was admitted to the coronary care unit after an aborted sudden cardiac death. The patient was awakened to answer a telephone call and suddenly collapsed. The fall was witnessed and a rapid 911 call allowed the paramedics to arrive within 5 minutes. • The patient was in VF and was successfully defibrillated with one shock. She remained comatose and was intubated and transported to the hospital. • Her past medical history is remarkable for 3 brief fainting episodes. • Her family history is notable for a sister who died suddenly at the age of 20.
Case II What is the most likely diagnosis at this time? a. HCM b. Brugada syndrome c. Idiopathic VF d. RVOT tachycardia e. Long QT syndrome
Syncope: Torsades From the files of DG Benditt, UM Cardiac Arrhythmia Center
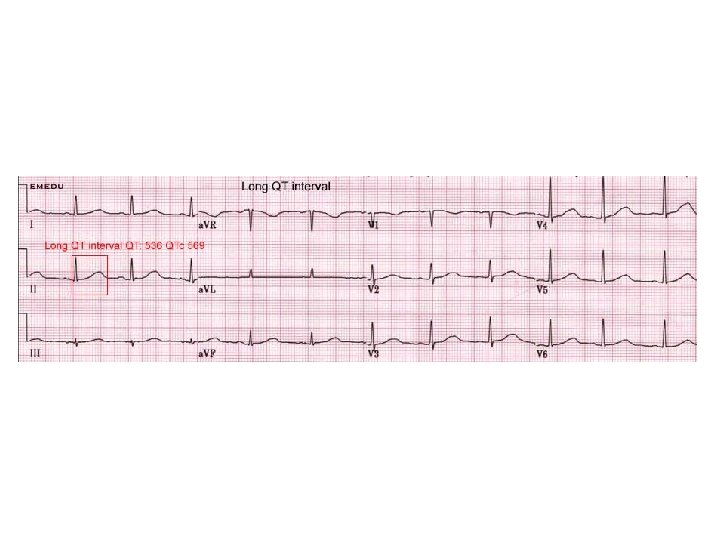
Drug-Induced QT Prolongation • Antiarrhythmics – Class IA. . . Quinidine, Procainamide, Disopyramide – Class III…Sotalol, Ibutilide, Dofetilide, Amiodarone, (NAPA) • Psychoactive Agents – Phenothiazines, Amitriptyline, Imipramine, Ziprasidone • Antibiotics – Erythromycin, Pentamidine, Fluconazole • Nonsedating antihistamines – (Terfenadine), Astemizole • Others – (Cisapride), Droperidol
Torsades de pointes • Treatments of drug-induced prolongation of QT interval and torsades de pointes include all of the following except: • • • a. Withdrawal of the offending agent b. Correction of electrolyte and acid-base disturbance c. IV magnesium d. IV isoproterenol infusion or temporary pacing e. IV beta blocker
LQT Case CONTINUED • Within the first 24 hours of hospitalization the patient recovers quickly until there are no apparent neurologic deficits. She provides no additional history and reports no symptoms prior to the cardiac arrest. What is the next step in her management? • • • a. Left cardiac sympathetic denervation b. Dual-chamber permanent pacemaker c. Amiodarone d. Single-chamber ICD e. Atenolol
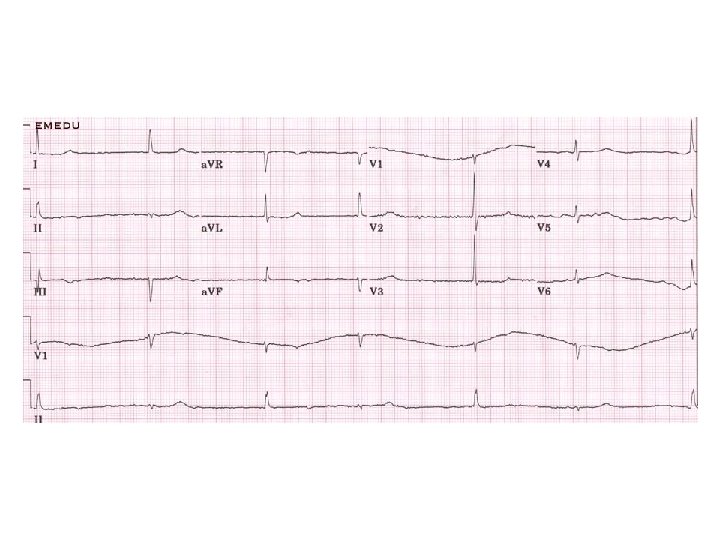
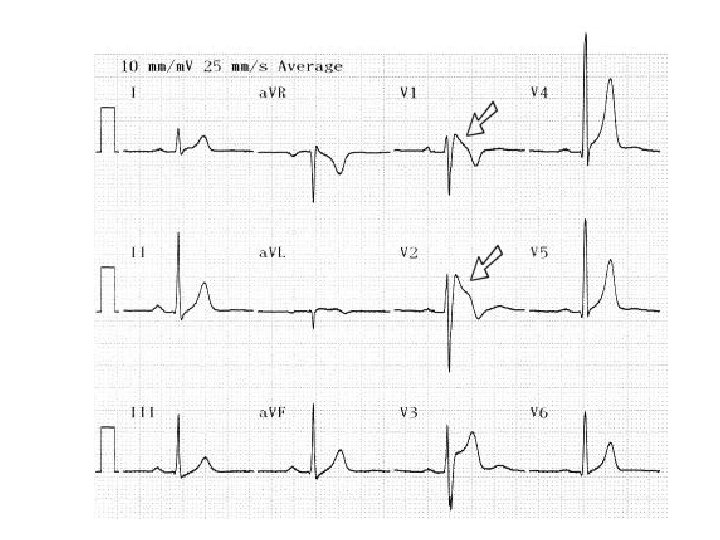
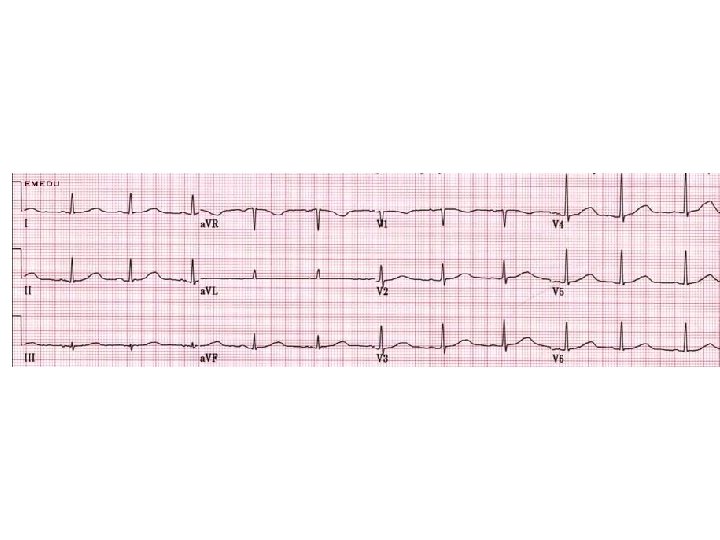
Case III • A 32 -year-old male is referred to you by his primary care provider after an episode of syncope. The patient was briskly walking with friends when he suddenly passed out with recovery after falling to the ground. The patient takes no medication and does not use illicit drugs. • A family history is notable for a father who died suddenly while shoveling snow at the age of 45. The physical examination is consistent with a healthy male with no distinct abnormalities. • His ECG is displayed on the next page. • An echocardiogram shows mild-to-moderate RV enlargement with a mild reduction in systolic function
Case III
Case III • The history, examination, and tests are most suggestive of what disease process? a. Arrhythmogenic RV dysplasia b. RVOT tachycardia c. HCM d. Long QT syndrome e. Vasovagal syncope