Evaluation of Macrocytosis Rachana Amberker PGY 2 Internal

Evaluation of Macrocytosis Rachana Amberker PGY 2 Internal medicine

Objectives • Relevant history • Mechanisms of macrocytosis • Causes • Clinical features • Diagnostic work up

Case scenario • A 78 year old Caucasian female presents to PCP after routine CBC showed macrocytosis • She was noted to have gradual increase in mean corpuscular volume (MCV) from 95 fl to 104 fl over the last few years • The patient complains of feeling tired during the day and sleeping for longer durations in the night

Medical and surgical history • Hypertension – well controlled on HCTZ • Bleeding gastric ulcer s/p partial gastrectomy Social History • Retired office worker • Quit smoking 30 years ago and drinks alcohol (1 glass of wine or beer once a week) Family History • No history of cancer, heart disease or stroke

Additional history
, a blood disorder characterized by the inability of the")
Ethnicity? • Pernicious anemia (PA), a blood disorder characterized by the inability of the body to properly absorb vitamin B 12, results in a macrocytic form of anemia • PA is the most common cause of vitamin B 12 deficiency anemia, and is more common in patients of northern European heritage and in African Americans • Patient response: My grandparents immigrated from Germany and Ireland.

Any h/o exposure to chemicals or radiation? • There is some relationship between exposure to chemicals or radiation in a group of myelodysplastic syndrome patients • Patient response: No, not to her knowledge Are you taking medications or nutritional supplements? • Certain medications can result in macrocytosis. These include chemotherapeutic drugs (methotrexate, hydroxyurea, azathioprine, etc. ), as well as phenytoin and trimethoprim-sulfamethoxazole • Patient response: No

Diet • A pure vegetable diet is deficient in vitamin B 12, but rich in folate; pure vegans may develop a vitamin B 12 deficiency from a lack of animal products in their diet • A folate deficiency could be indicated if the patient does not eat vegetables Patient response: I eat a normal diet consisting of meat, eggs, and vegetables

Do you drink alcohol? If so, how much? • Alcohol, when abused, is a common cause of poor diet. This commonly results in a deficiency of folate in alcoholics • Alcohol is also a cause of macrocytosis, even when the patient is not folate deficient Patient response: I drink socially once a week - at most a glass of wine or beer

Do you have any problems walking, especially in the dark? • Neurologic abnormalities associated with vitamin B 12 deficiency may include symmetrical weakness and paresthesias of hands and feet and loss of vibratory sense in the lower extremities • These are caused by degeneration of the posterior and lateral columns of the spinal cord with areas of demyelinization and loss of sensory fibers Patient response: No, I do not.

Physical exam • Afebrile, HR- 69 bpm, RR - 16 breaths per min, BP 127/62 mm Hg, saturating at 97% on room air • Constitutional - No acute distress, cervical lymphadenopathy • Eyes - Mild pallor, No icterus • Lungs - Good bilateral air entry, no wheeze, rales or rhonchi • Heart - Irregularly irregular, Normal S 1, S 2, no murmurs, rubs or gallops • Abdomen - No tenderness or distension and no hepatosplenomegaly • Neurological - No focal neurological deficit, cranial nerves 2 -12 are intact

In summary • We have a 75 yr old female presenting with c/o generalized fatigue and was found to have macrocytosis of 104. • She has a significant surgical h/o partial gastrectomy • Largely unremarkable physical exam Differential diagnosis: Megaloblastic anemia preferably Vitamin b 12 deficiency However other non megaloblastic causes cannot be ruled out at this point of evaluation.
 • Normal physiologic response to anemia •")
Mechanisms for macrocytosis. Reticulocytosis (MCV 103 -126) • Normal physiologic response to anemia • Increased erythropoietin Increased RBC production developing RBCs skip cell division and enter peripheral circulation sooner • Usually occurs unless BM response is blunted by other factors like cytokines in ACD, vitamin b 12 deficiency or iron deficiency

• Lack of central pallor • Oval to irregular outline • Blue tint ( polychromatophilia)

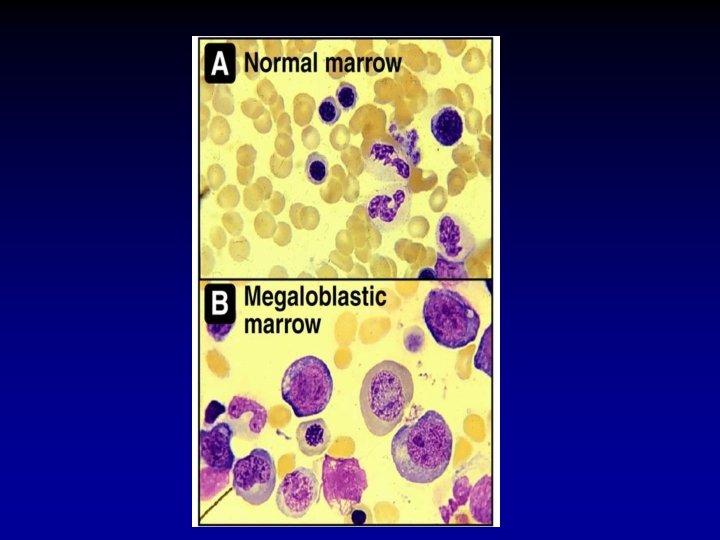
Abnormal RBC development • DNA synthesis and cell division is affected due to nutritional deficiency (vit b 12, folate) or medications. • Asynchrony between nucleus and cytoplasm maturation leads to production of large immature nuclei relative to the cytoplasm along with other megaloblastic changes • All cell lines are affected

Abnormal RBC membrane • RBC membrane is a composed of lipids and proteins. Certain conditions alter membrane composition resulting in increased cell volume. • Example : In liver disease, increased membrane cholesterol content resulting in macrocytosis.

Causes of Macrocytosis Reticulocytosis Megaloblastic anemia • Hemolytic anemia • Vitamin B 12 • Recovering marrow after chemotherapy or BMT • Folate deficiency • erythropoiesis after administration of erythropoietin, repletion of Fe, vitamin B 12, or folate • Medications that interfere with DNA synthesis Multifactorial • Alcohol • Liver disease • Myelodysplastic syndrome • Hypothyroidism • Aplastic anemia • Multiple myeloma • Bariatric surgery

Causes of vitamin B 12 deficiency Nutritional • Decreased intake – only in vegans Malabsorption due to intrinsic factor (IF) deficiency • Pernicious anemia • Prior total or partial gastrectomy Malabsorption due to associated gastrointestinal abnormalities • • Achlorhydria and/or H. pylori infection Celiac disease Crohn’s disease Bacterial overgrowth Parasitic infestation with fish tapeworm (Diphyllobothrium latum) Lymphoma Surgical resection of ileum

Clues from physical exam – Vitamin B 12 • Oral exam • Neurological exam

Oral examination of tongue - Attrition and dysplasia of all exfoliating cell populations - Signs to look for includes - Atrophy - Depapillation - Thinning of epithelium at sides and tip of tongue (causes painful glossitis and angular stomatitis).

Neurologic examination • Test for neuropathy to detect subacute combined degeneration of the spinal cord due to a vitamin B 12 deficiency • Vitamin B 12 deficiency results in demyelination of the posterior and lateral columns of the spinal cord as well as the peripheral sensory nerves.

Causes of folate deficiency Nutritional Malabsorption utilization Drugs • Goat’s milk diet • Tropical sprue • Pregnancy • Phenytoin • Alcoholism • Celiac disease • Hemolytic anemia • Phenobarbital • Crohn’s disease • Psoriasis • Methotrexate • Note: Much less common now that many staple foods are supplemented with folate • Lymphoma • Prior intestinal surgery (short bowel syndrome) • Trimethoprimsulfamethoxazole • Pyrimethamine

Laboratory evaluation

• CBC with differential • Peripheral blood smear • Liver panel with LDH • Reticulocyte count • Serum folate levels • Serum vitamin B 12 • Methyl malonic acid (MMA) and serum homocysteine • Thyroid function test • Bone marrow examination

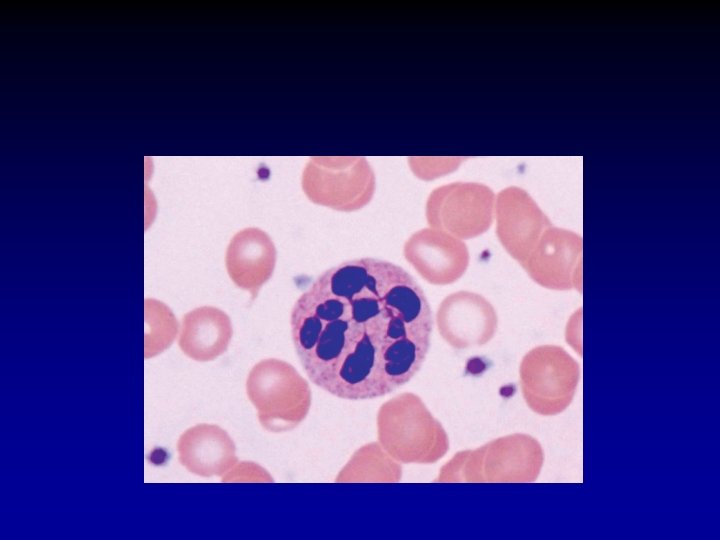
Peripheral smear findings Macro-ovalocytes Hyper segmented neutrophils

Liver panel with LDH • Liver disease is a common cause of macrocytosis, due to abnormalities in the plasma lipids leading to increased RBC membranes • Elevation of lactate dehydrogenase (LDH) and indirect bilirubin levels, reflect high marrow turnover rate and intramarrow premature cell death of red cells (also called ineffective hematopoiesis)

SERUM VITAMIN B 12 • Serum B 12 level is an important diagnostic test for the evaluation of a megaloblastic anemia. Normal – > 300 Borderline – 200 - 300 Low -- <200

Serum folate levels • Earliest indicator of folate deficiency • Respond rapidly to changes in dietary folate • Misguide --Single meal with normal folate content can improve serum folate levels to normal

RBC folate levels • Folate is incorporated into erythrocytes when they are formed, and folate levels do not fluctuate with changes in diet during the lifespan of the RBC • RBC folate < 150 microgram/L is consistent with folate deficiency
 and serum homocysteine")
Methyl malonic acid (MMA) and serum homocysteine
 and serum homocysteine • Vitamin B 12 is required as")
Methyl malonic acid (MMA) and serum homocysteine • Vitamin B 12 is required as a co-factor for the conversion of methyl malonic acid (MMA) to succinyl Co. A • Vitamin B 12 and folate are required as a cofactor for the conversion of homocysteine (HC) to methionine • Vitamin B 12 deficiency: Both HC and MMA values increase in serum • Folate deficiency: HC levels are increased and MMA values are normal

Our patient’s labs

LABS

Methylmalonic acid and homocysteine: normal

Peripheral blood smear • Macrocytosis • Normal WBC • Normal platelets

Clinical course • Considering the patient’s history of gastric surgery and boderline low Vit b 12 Levels her primary care physician decided to maintain the patient on vitamin B 12 (cyanocobalamin) shots. • These did nothing to reverse the anemia. • After few months the patients labs look like:

Test Hb Patient results Normal 8. 8 12 -15. 6 HCT 28. 5% 35 -46 MCV 118 fl 80 -100 RDW 17. 5 9 -15 WBC 5200 4, 800 -11, 000 Neutrophils 67% 42 -75 Lymphocytes 45% 20 -51 Platelet count 338, 000 1. 5 -400, 000 6. 4 >1. 9 1579 230 -1139 Folic acid Vitamin B 12

What is your interpretation of these findings? • Non Megaloblastic anemia

What laboratory tests should now be ordered? • Examine peripheral blood • Perform a bone marrow examination with cytogenetics and flow cytometry

Peripheral smear Pseudo-Pelger-Huet cells

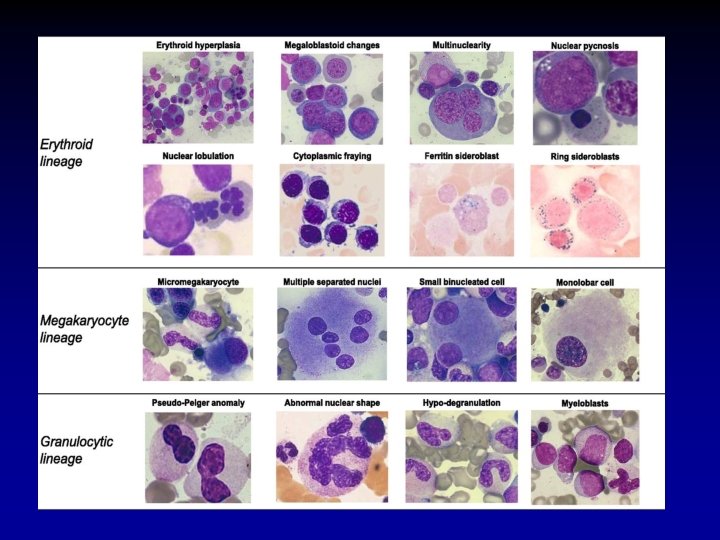
Bone marrow Showed - Dysplastic changes in the erythroids, granulocytes and megakaryocytes with hypercellularity.
 5 q- clone deletion")
Cytogenetics Normal 46 , XX (female karyotype) 5 q- clone deletion

Myelodysplastic syndrome • Comprise a heterogeneous group of malignant hematopoietic stem cell disorders characterized by dysplastic and ineffective blood cell production • Commonly occurs in older adults • de novo or arise years after exposure to potentially mutagenic therapy (ex- radiation exposure, chemotherapy)

MDS - cont • Considered in patients with unexplained cytopenias • PBS and BM aspirate is necessary to identify dysplastic cytologic features • Chromosomal abnormalities helps to distinguish MDS from leukemia and also help in classification of MDS, determining prognostic risk group and therapy

MDS • The patient is started on treatment with lenalidomide, a bone marrow modulating agent approved for the treatment of myelodysplasia associated with the 5 q- chromosomal deletion • After 9 weeks of treatment the patient’s hemoglobin stabilized

Take home points. • Ask h/o diet, alcohol, medications, exposures to chemicals/ radiations, surgeries, gait abnormalities. • Mechanisms are reticulocytosis, abnormal cell development, abnormal RBC membrane. • Vit b 12 deficiency and folic acid is differentiated through HC, MMA. • Peripheral smear of Vitb 12 shows hyper segmented neutrophils. • Older people with cytopenia think about MDS. • BM with cytogenetics and flow cytometry aid us in diagnosing and managing MDS

THANK YOU!

References • Uptodate • Dynamed • ASH

Question 25 • A 79 -year-old woman is diagnosed with new-onset anemia during a routine examination. Medical history is significant for an ischemic stroke 8 weeks ago, which resulted in residual right-sided weakness and admission to a rehabilitation facility. At that time, her complete blood count was normal. She has been eating poorly while in the facility. Her medications are aspirin, lisinopril, and simvastatin. • On physical examination, temperature is 37. 1 °C (98. 8 °F), blood pressure is 120/70 mm Hg, pulse rate is 82/min, and respiration rate is 12/min; BMI is 27. Right-sided motor strength is 3/4 and sensation is normal.
 Mean")
• • • Laboratory studies: Hemoglobin 10. 1 g/d. L (101 g/L) Mean corpuscular volume 102 f. L Folate 2. 5 ng/m. L (5. 7 nmol/L) Homocysteine 10. 2 mg/L (75. 4 µmol/L) Methylmalonic acid Normal

• Which of the following is the most likely diagnosis? • A Folate deficiency • B Iron deficiency • C α-Thalassemia trait • D Vitamin B 12 deficiency

Question 68 • A 30 -year-old woman is evaluated for progressive difficulty walking and numbness in both feet of 1 to 2 months' duration. She is otherwise healthy. She has followed a vegan diet for the past several years. Her only medication is an oral contraceptive pill. • On physical examination, temperature is 37. 0 °C (98. 6 °F), blood pressure is 120/66 mm Hg, pulse rate is 76/min, and respiration rate is 12/min; BMI is 25. She has decreased sensation and vibratory sense in both legs below the knees. No other neurologic deficits are observed. • Laboratory studies: Hemoglobin 10. 4 g/d. L (104 g/L) Leukocyte count 2800/µL (2. 8 × 109/L) Mean corpuscular volume 105 f. L Vitamin B 12 210 pg/m. L (155 pmol/L)

• Which of the following is the most appropriate diagnostic test to perform next? A Bone marrow biopsy B Folate level measurement C Homocysteine level measurement D Methylmalonic acid level measurement
- Slides: 56