Evaluation and Treatment of Pathologic Hearing Deficits Review














![Example 2: Type A • A[d] • A[s] • Hypermobility of tympanic membrane •](https://slidetodoc.com/presentation_image_h/76115394fc51744d2318966236020b85/image-15.jpg "Example 2: Type A • A[d] • A[s] • Hypermobility of tympanic membrane •")



































. Angel Sound: Interactive Listening Rehabilitation and Functional Hearing Test")
- Slides: 55
Evaluation and Treatment of Pathologic Hearing Deficits & Review of New Hearing Aids Available to the Patient Presented By: Dr. Sarah Vonder. Brink, Au. D.
Outline • Pretest • The Audiologic Assessment • Tympanometry • Audiometry • Treatment of hearing loss • Hearing Aids • Aural Rehabilitation • Tinnitus Therapy • Post Test • Questions • References
Learning Outcomes • Identify the necessity for early identification of hearing loss • Summarize audiologic testing and interpretation of results • Evaluate the need for treatment of hearing loss and tinnitus
What is the most common form of sensorineural hearing loss? A. B. C. D. Presbycusis Noise Induced hearing loss 75% are unknown etiology Ototoxicity
Type B tympanogram is indicative of: A. Normal tympanic membrane mobility and middle ear pressure B. Normal ear canal volume with limited or no tympanic membrane mobility C. Abnormal ear canal volume with no tympanic membrane mobility D. B & C only E. None of the above
Affects of hearing loss • Depression • Dementia • Anxiety • Separation • Decreased quality of life
The Audiologic Assessment • Comprehensive Case History • Otoscopy/Cerumen management • Diagnose type/degree of hearing loss • Determine need for treatment/referral to physician or further testing • Counseling for patient, family caregiver on results/recommendations • Assess candidacy and motivation towards amplification • Determine medical clearance as determined by FDA
Case History • Onset, duration, and laterality of symptoms including ear disease, trauma, surgery • Noise exposure • Tinnitus • Dizziness • Family history • Medications
Otoscopy • Wax occlusion • Perforation • Foreign body • Abrasion • Infection • Abnormality of tympanic membrane
Evaluation of hearing deficits • Tympanometry • Audiometry • Air conduction • Bone conduction • Speech Testing • Speech Reception Scores • Word Recognition Scores
Tympanometry • Evaluation of the middle ear
4 Measurements: 1. Ear canal volume/Physical volume: an indirect measure of size of the ear canal (if the TM is intact) or ear canal + middle ear (when there is a TM perforation or PE tube). 2. Peak compensated static acoustic admittance: an indirect measure of peak TM mobility 3. Width (AKA Gradient): also an indirect measure of TM mobility, but not just peak TM mobility 4. Middle ear air pressure peak: an indirect measure of Eustachian tube function
Example 1: Type A 1. Normal ear canal volume: 0. 8 – 1. 6 cm 3 2. Normal pressure: 0. 3 – 1. 4 ml/cm 3/mmho 3. Normal width: 48 -110 da. Pa 4. Normal peak pressure: +200 to -400 da. Pa
Example 2: Type A • A[d] • A[s] • Hypermobility of tympanic membrane • Possible ossicular disarticulation • Thin membrane • Hypomobility of tympanic membrane • Fluid • Tympanosclerosis
Example 3: Type B • Flat tympanogram • Large ECV: Perforation or PE Tube • Small ECV: Obstruction • Normal ECV: middle ear pathology • Abnormal Admittance • Abnormal Width • Abnormal Middle Ear Pressure
Example 4: Type C • • Normal ear canal volume Normal static acoustic admittance Slightly negative pressure peak Normal width
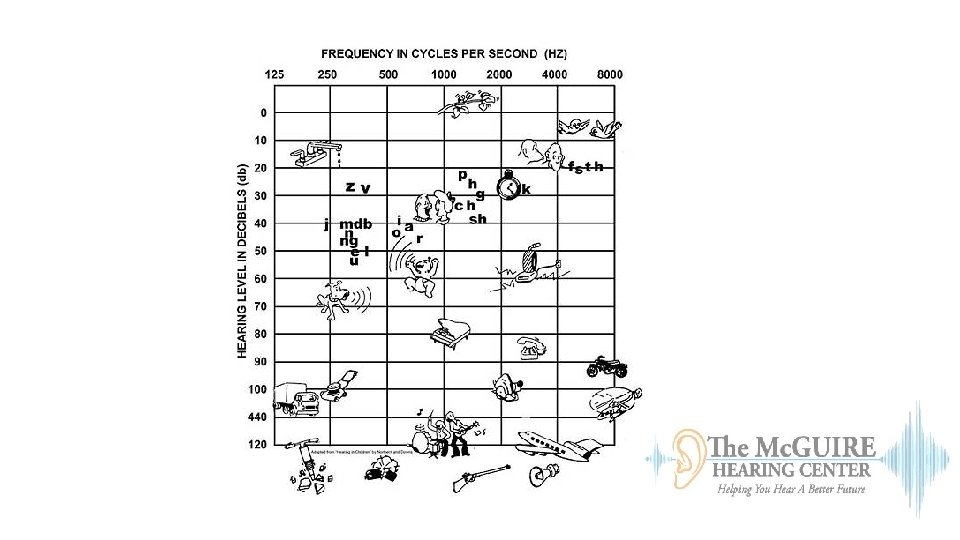
Audiometry Air conduction Bone conduction
Air Conduction: Degree of hearing loss • < 25 d. B normal • 26 -40 d. B mild • 41 -55 d. B moderate • 56 -70 d. B moderately severe • 71 -90 d. B severe • 91+d. B profound
Bone Conduction: Type of hearing loss • Sensorineural • Conductive • Mixed Example 1:
Example 2: • Mixed hearing loss bilaterally • Bone conduction scores outside normal range • Evident air bone gaps, indicative of a conductive component
Example 3: Presbycusis • Most common form of sensorineural hearing loss is presbycusis • Greek derivation: • “presby” meaning elder • “cusis” meaning hearing
Inside the Cochlea • Outer Hair cell loss • 40 to 60 d. B • Inner Hair Cell loss • Addition 25 to 30 d. B • Word understanding declines
Speech Testing Speech Reception Thresholds Word Recognition Scores
Speech Reception Threshold • Minimum intensity level required for 50% recognition of spondees • PTA/SRT agreement • +/- 6 d. B is good agreement • 7 -12 d. B is fair agreement • 13 or more d. B is poorer agreement
Word Recognition Score • Monosyllabic words are presented at an audible level and a % correct is obtained. • As a very general tendency, patients with normal hearing do best, and patients with conductive hearing loss do similarly well • Patients with outer hair cell damage will likely do a little worse • Those with inner hair cell and/or neural damage tend to do most poorly
Degree of HL: Effect on Word Recognition
Reliability of results • Malingering/Pseudohypacusis • False negatives • False positives • Poor/Fair reliability • PTA/SRT disagreements
Hearing loss and neurologic disease • Loss of neurons • Reduction in number of synaptic connections between neurons • Changes in excitatory and inhibitory neurotransmitter systems • Changes in neural transmission along the auditory pathway • Changes in cognitive processing of the acoustic signal • Decrement in long term and short memory
Hearing loss and neurologic disease • Hearing aids may not only improve hearing but preserve the brain • Decline in hearing abilities may accelerate gray matter atrophy and increase listening effort • Early diagnosis and treatment of hearing loss slows the progression of dementia and Alzheimer’s disease
Referrals • • Child under 18 years Visible congenital or traumatic deformity of the ear Active drainage within past 90 days Sudden or progressive hearing loss within 90 days Acute or chronic dizziness Fluctuating hearing loss or tinnitus Pain or discomfort in the ear Unilateral or asymmetric hearing loss • Difference between ears (500, 1000, 2000, and 3000 Hz) of > 15 d. B • Conductive hearing loss • Defined as air-bone gap > 15 d. B at 500 Hz, 1000 Hz, and 2000 Hz
“The audiogram provides a description of the magnitude of the patient’s hearing loss, however, it does not adequately portray the patient’s communication difficulties or aural rehabilitation needs”
Treatment of hearing loss
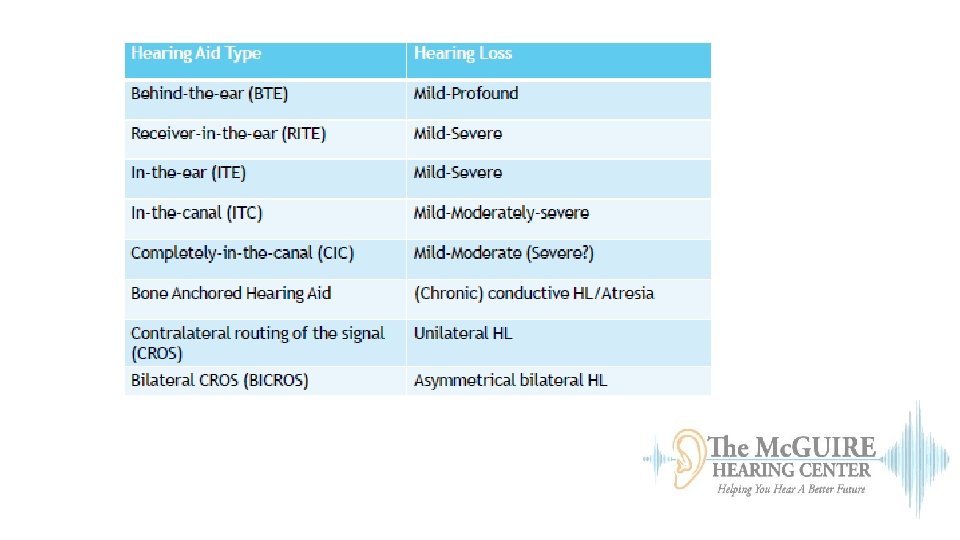
Hearing Aids • Style • Levels of technology • Realistic Expectations • Aural Rehabilitation
Style: One Size does not fit all Custom Standard
Hearing Aids: Today’s Technology • Hearing Aid Components • Microphone Automatic directional microphones • Amplifier • Receiver • Volume or on/off control • Signal Processing: Analog vs. Digital • Algorithm • Signal processing • Amplifying the signal • Telecoil
Levels of technology: Based on life style • Premium • • • Most expensive Best background noise reduction Best speech clarity Wind guard Echo protection Tinnitus Therapy • Mid-level • Similar to premium technology • Does not have automatic features • Basic • For patient who struggles in one on one conversation and rarely in adverse environments
Realistic Expectations A hearing aid is… A hearing aid is NOT… • A medical device • Prescribed by an audiologist or hearing aid dispenser • Can delay progression of neurological disease period • Therapy for tinnitus • A substitute for normal hearing • A substitute for effective communication strategies • A personal amplification system • A preventative measure for hearing loss
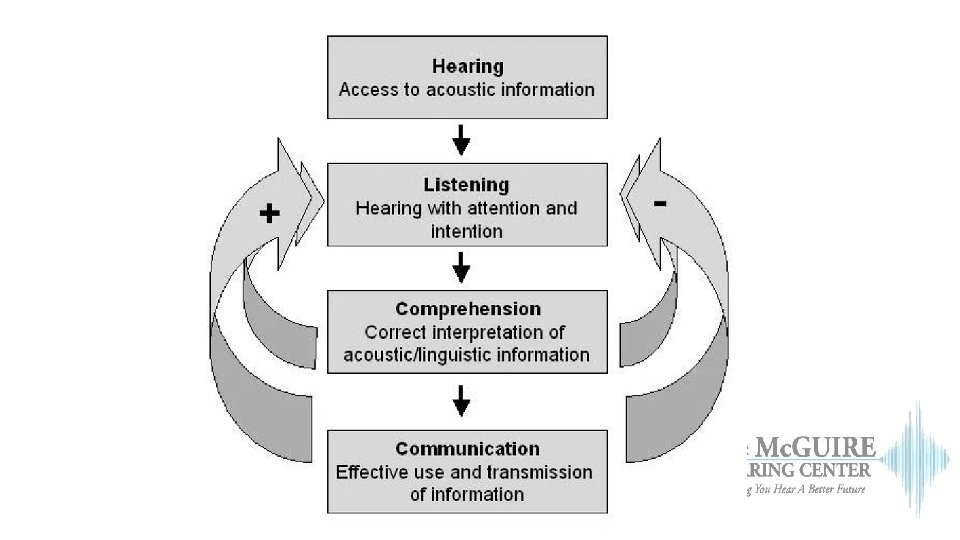
Aural Rehabilitation
• The focus should be placed on communication, not simply hearing • Computer based therapy • Angel sounds • LACE • Partner readings • Group vs Individual therapy • Goal Setting
Tinnitus Treatment
Tinnitus Treatment • Avoid noise exposure • Reduce stress • Get adequate sleep • Limit alcohol • Limit caffeine • Limit tobacco • Limit salt intake • Maintain constant background of noise • Stay busy with meaningful activities
Tinnitus Treatment • Relaxation training/exercise • Cognitive therapy/counseling • Masking Devices • Sound Enrichment • Tinnitus retraining therapy • Amplification
Signal therapy • Consistent signal • Patient can have volume control • Variety of signals • User preference
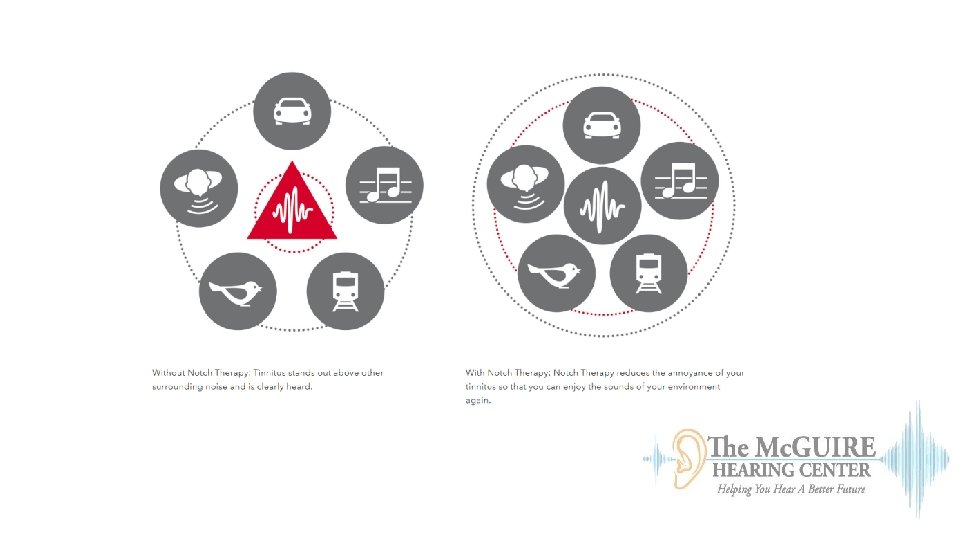
Notch Therapy • Stimulate regions above and below pitch of tinnitus • Improvement after 8 hours of exposure for 6 months • Signal is determined by patient
Learning Outcomes • Identify the necessity for early identification of hearing loss • Summarize audiologic testing and interpretation of results • Evaluate the need for treatment of hearing loss and tinnitus
Post Test
What is the common form of sensorineural hearing loss? A. B. C. D. Presbycusis Noise Induced hearing loss Most hearing losses have an unknown etiology Ototoxicity
Type B tympanogram is indicative of: A. Normal tympanic membrane mobility and middle ear pressure B. Normal ear canal volume with limited or no tympanic membrane mobility C. Abnormal ear canal volume with no tympanic membrane mobility D. B & C only E. None of the above
Questions?
References • Angel Sounds. (2018). Angel Sound: Interactive Listening Rehabilitation and Functional Hearing Test Program. Retrieved from angelsound. tigerspeech. com • Aural Rehabilitation. (n. d. ). Retrieved January 12, 2018, from https: //www. hearingsolutions. ca/services/aural-rehabilitation • Cox, Robyn M. , et al. (2014) Impact of Advanced Hearing Aid Technology on Speech Understanding for Older Listeners with Mild to Moderate, Adult-Onset, Sensorineural Hearing Loss: Gerontology Karger Publishers, Retrieved from www. karger. com/article/fulltext/362547. • Hearing Aids for Tinnitus. (2017). Signia Hearing Aids. Retrieved from: www. signiausa. com/tinnitus/solutions-for-tinnitus. • Lin, F. R. , & Albert, M. (2014). Hearing Loss and Dementia: Who’s Listening? Aging & Mental Health, 18(6), 671– 673. http: //doi. org/10. 1080/13607863. 2014. 915924 • Miller, E. (2014). Hearing Aids I [PDF Document]. • Tye-Murray, Nancy. (2015) Foundations of Aural Rehabilitation: Children, Adults, and Their Family Members (3 rd ed. ). Clifton Park, NY: Cengage Learning. • Sonstrom, K. (2015). Auditory Training in Adults [PDF Document]. • Steiger, J. (2014). Tinnitus Audiologic Evaluation and Treatment [PDF Document]. • Sweetow, Robert, and Catherine V. Palmer. (2005) Efficacy of Individual Auditory Training in Adults: A Systematic Review of the Evidence. Journal of the American Academy of Audiology, vol. 16, no. 7, pp. 494– 504. , doi: 10. 3766/jaaa. 16. 7. 9. • Van, K J, et al. (1986) Principles of Tympanometry. ASHA Monographs. , U. S. National Library of Medicine, www. ncbi. nlm. nih. gov/pubmed/3730039.